

🦋doctor doubt🦋
@reverendofdoubt
Followers
10,328
Following
3,480
Media
496
Statuses
8,389
Emergency Physician
Everywhere All at Once
Joined April 2012
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
Mother's Day
• 2156128 Tweets
Arsenal
• 538453 Tweets
Ángel
• 209581 Tweets
Travis
• 168200 Tweets
Cataluña
• 86422 Tweets
Spurs
• 86392 Tweets
Sarah
• 84942 Tweets
Racing
• 55788 Tweets
Illa
• 53989 Tweets
#Amici23
• 53671 Tweets
Pacers
• 42119 Tweets
The Knicks
• 35075 Tweets
Hawks
• 34768 Tweets
Vitória
• 34619 Tweets
Trae
• 34362 Tweets
Abel
• 27024 Tweets
#ConexiónHonduras10
• 23492 Tweets
Rony
• 23454 Tweets
الزمالك
• 22967 Tweets
Pistons
• 22434 Tweets
Costas
• 17938 Tweets
雨の月曜日
• 17758 Tweets
Veiga
• 17112 Tweets
Rory
• 12743 Tweets
Belgrano
• 12439 Tweets
土砂降り
• 11729 Tweets
Rossi
• 11127 Tweets
Jara
• 10760 Tweets
Last Seen Profiles




















@toxicologist12
I may or may not have been responsible for telling said patient to go for it when asked if they could order door dash while I was screening them in triage… in fairness, I didn’t know they were going to throw a pizza party 😂
8
20
4K
Y’all I’m gonna be honest, they need to have an on-call emergency physician or trauma physician to Zoom in to ESPN to explain what’s going on since I don’t think it’s being explained well what happened…
76
119
4K
"too sick for the ICU" is a new one... guess the ED is appropriate...
100
128
2K
ED doc here — not worth it. Watch the game at home.


74
115
2K
If you work in the outpatient setting and are sending your patient to the ER, please don’t say they’ll be seen immediately since you’re calling ahead, and don’t tell them the ER is expecting them.
… volumes are high everywhere, and false expectations make things difficult 🙏🏻🙏🏻
49
124
1K
Avoiding IV access in the ipsilateral arm of those who had lymph node dissection or mastectomy is a Thing We Do For No Reason and likely has contributed to more harm than preventing the very, very rare lymphedema
This practice is from the days of radical mastectomies.

What’s your unpopular medical opinion that would land you in this position?
Drop it in this thread

2K
241
2K
43
57
923
Should Twitter ban
@elonmusk
? Let the people speak. Vox Populi, Vox Dei.
Ban Musk
12692
Keep Musk
1689
55
1K
872
Now that I’m at a place that uses procalcitonin regularly after not having it during residency, I am convinced it is one of the most useless lab tests out there.
65
43
827
Being an attending is way better than being a resident.
35
21
599
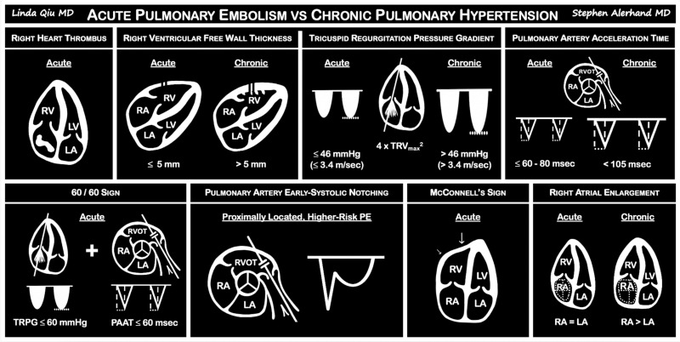
Damn good article!
What echocardiographic findings differentiate acute pulmonary embolism and chronic right pulmonary hypertension? |
#AJEM
7
181
483
Ketamine, summarized. Excitement outpaces evidence, but some indications for it below.
From
@CritCareMed
.
Link:
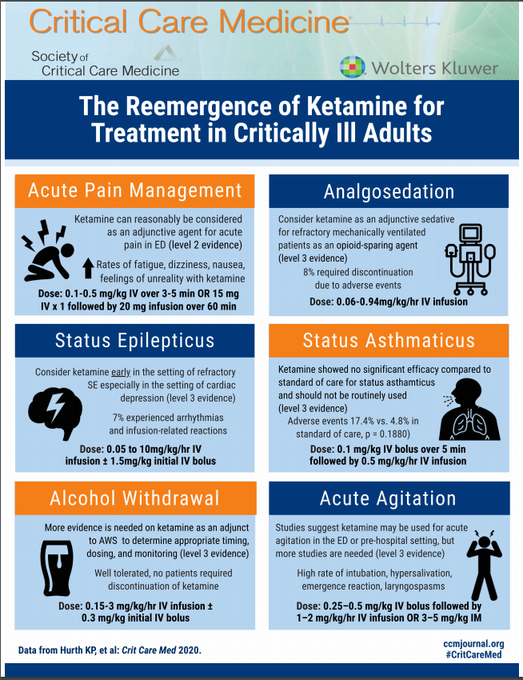
5
157
438
why are we still using eponyms in medicine?
Legg-Calves-Perthes disease... or, ya know, just say what we actually mean, like avascular necrosis of the femoral head
38
27
425
Emergency medicine is tough. It’s hard right now not gonna lie.
But you know what? It’s a great group of people to work with, I still love it, I still wouldn’t choose any other specialty.
There’s 500+ unmatched EM positions. If you didn’t match, join our family. We want you!!
8
31
413
Another state-of-the-art research paper out of
@JohnsHopkinsEM
by
@MichaelEhmannMD
@Hinson_EM
debunking contrast-induced nephropathy!!
This time, those with GFR < 30 were also added!
Published in
@yourICM
!!

9
137
403
I love telling junior residents that ceftriaxone is an impressively broad spectrum antibiotic
24
27
386
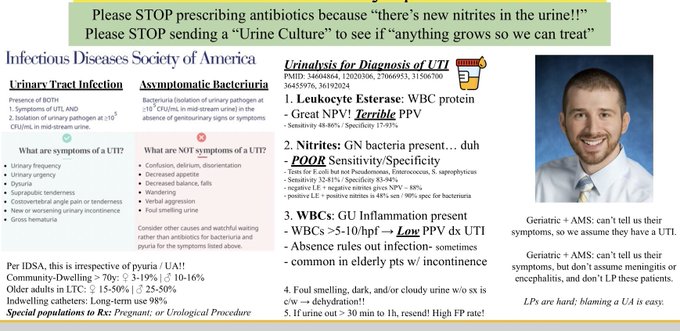
Just putting this here since apparently there’s an entire cohort of people in medicine who know nothing about UTIs and honestly it’s kind of alarming
24
52
355
Me: *sees normal looking ECG on Twitter*
ECG Twitter: Duh this is slam dunk OMI of OM2 went to Cath lab from their car
Me:
11
28
346
Saved a heart/life today based on remembering this pattern by
@PendellM
@smithECGBlog
et al.
7
60
319
My go-to neurology resources:
1.
@caseyalbin
's "The Acute Neurology Survival Guide"
2.
@AaronLBerkowitz
's "Clinical Neurology & Neuroanatomy"
3.
@MicieliA_MD
's "The Code Stroke Handbook"
4.
@iBookCC
's
#IBNCC
5.
@a_charidimou
's Twitter illustrations
6.
@emrap_tweets
's Corependium
4
58
283
A single dose of toradol in the ED for a patient with CKD or who is on AC is fine.
What’s your unpopular medical opinion that would land you in this position?
Drop it in this thread
2K
241
2K
12
12
272
Per ACC, 3 new STEMI equivalents that warrant *emergent angiography*:
-LBBB or ventricular-paced rhythm with *either* original OR *modified* Sgarbossa Criteria
-DeWinter's sign
Let's be 100% clear- EM research led to these updates by e.g.
@PendellM
@smithECGBlog
(check ref!)
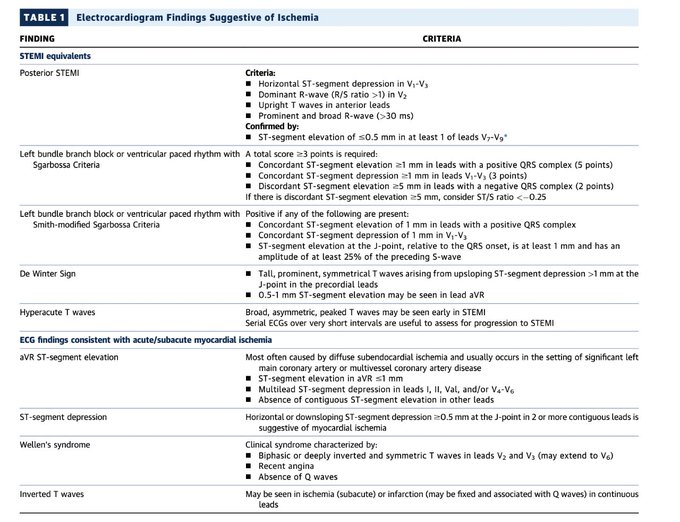

Here’s the proper article: 2022 ACC Expert Consensus Decision Pathway on the Evaluation and Disposition of Acute Chest Pain in the Emergency Department
#foamed
1
30
93
7
73
261
Butter sweet to get the research award and the PGY4 teacher of the year award
@JohnsHopkinsEM
. Nothing excites me more than teaching residents, and doing research with friends.
On my last shift right now, officially done with residency at 3pm, and off to
@MadtownEM
@UWEmerMed
!

36
3
259
Just an observation from the last 9yrs:
Every specialty thinks their niche area should be something the ED focuses on & should provide care for, which really could happen in an outpatient setting. The answer is NEVER: later hours and weekends for outpatient subspecialty care.
10
24
247
Friendly reminder to new trainees: ignore the "that urine smells like a UTI"
It's not part of the diagnostic criteria for UTI!
Urine can smell from dehydration, food, meds, etc
The "sniff test" for UTI:
- PPV 54% for bacteriuria
- PPV 28% for pyuria

18
86
244
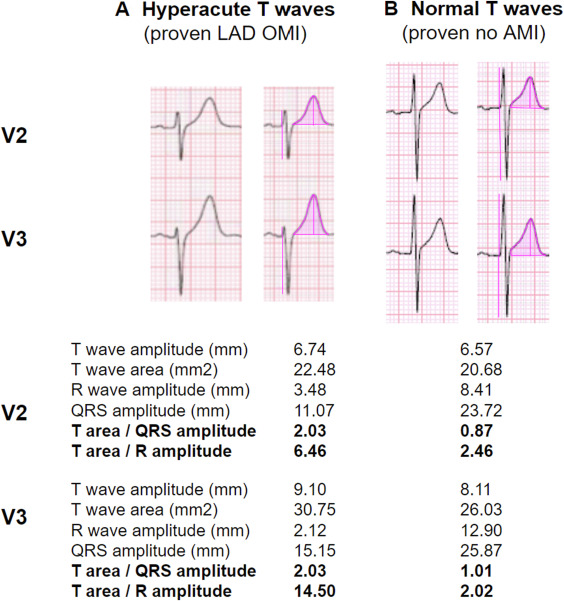
Hyperacute T-waves Can Be a Useful Sign of Occlusion Myocardial Infarction if Appropriately Defined
Great reply in
@AnnalsofEM
by
@smithECGBlog
&
@PendellM
1
76
239
“Clinical guidelines recommend [insert recommendation].”
Start reading the citations that support said recommendations and you’ll soon realize much of what we do in medicine is built on a house of cards.
@TheSGEM
17
35
223
I'm sure it's pretty obvious by now given which university accounts I RT on Twitter ☺️, but if you didn't already know...
I'm super stoked to be joining the faculty
@UWEmerMed
/
@MadtownEM
in July!
34
9
215
When there are 70 in the WR and a bed is available and the patient is just stable enough to transfer — palliative and GOC and all that jazz can be done upstairs, while we keep others from dying downstairs in the hallway and our ER nurses work miracles
5
2
191
2023 technology transition:
- iMessages / SMS texting to
@signalapp
/
@WhatsApp
- Gmail to
@ProtonMail
- Google drive to
@ProtonDrive
- minimizing apps on my phone, tracking turned off
- MacBook internet to
@ProtonVPN
Anything else I’m missing?
34
17
186
A very well-written, concise approach to this topic in
@ClevelandClinic
Journal of Medicine.
How do we maximize diuresis in acute decompensated heart failure?

9
62
185
First EM attending shift next week. Pro-tips and pearls appreciated.
58
4
182
Wow....

28
21
176
when the radiologist calls you in the ED with an important finding on imaging before the preliminary read is posted, take a moment to thank them ! couldn’t do this job without them !
5
6
152
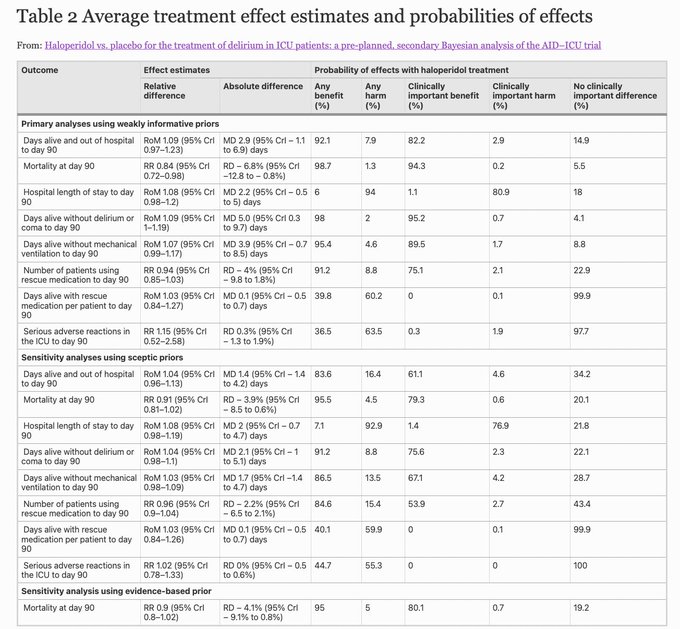
Haloperidol vs. placebo for the treatment of delirium in ICU patients: a pre-planned, secondary Bayesian analysis of the AID–ICU trial |
@yourICM
High prob of benefits, low prob of harm w/ haloperidol rx c/w placebo in adult ICU patients w/ delirium
8
37
148
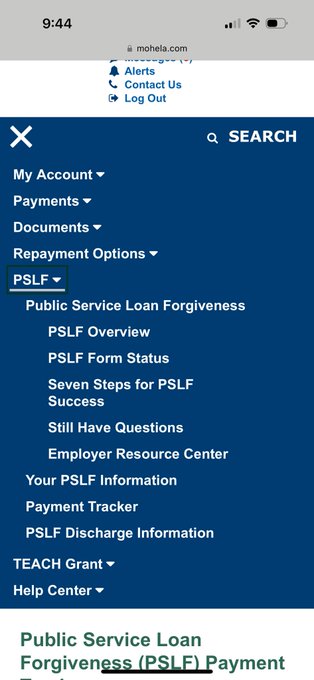
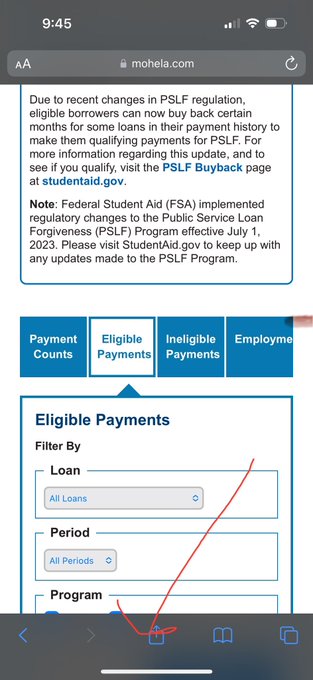
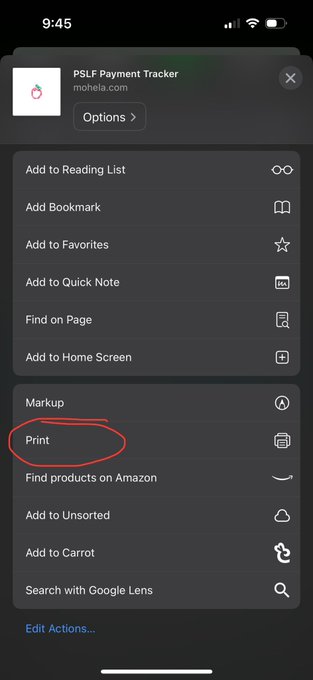
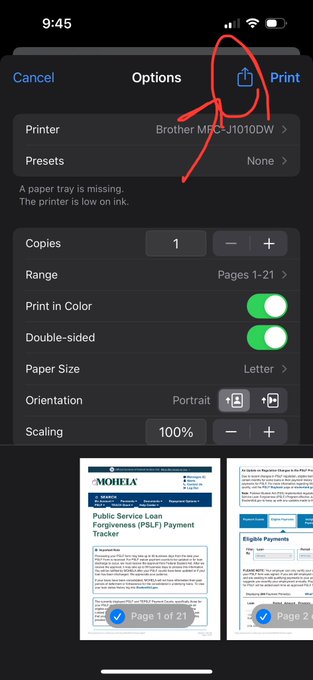
Don’t forget to save your PSLF information at Mohela!!! Here’s how to do it on your iPhone:
PSLF —> Payment Tracker —> Eligible Payments —> Click arrow/box on Safari —> PRINT (now it’s a PDF!) —> click arrow / box —> email it to yourself!
6
14
150
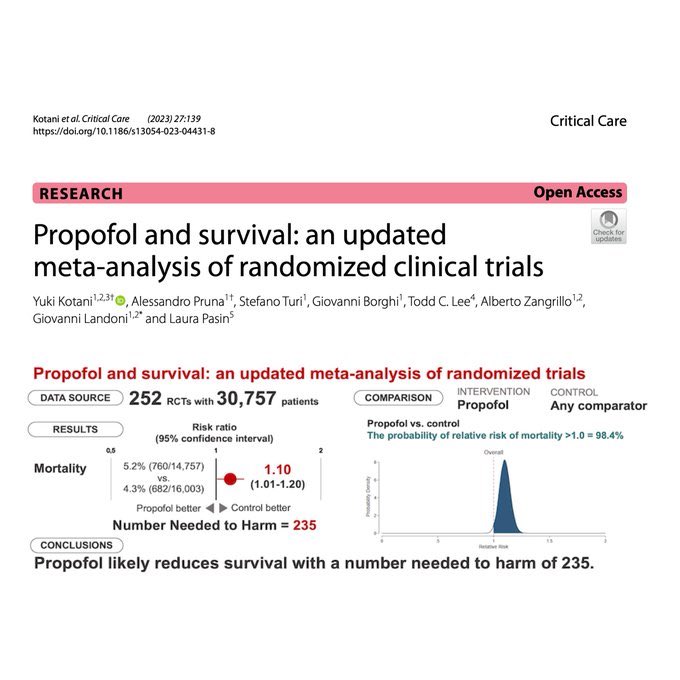
Time to black box propofol (likely used daily throughout the U.S ***orders of magnitude more*** than etomidate) if you want to black box etomidate.
6
13
145
@PhysicianDoodle
Verbally or physically abusing ED staff is inversely related with likelihood of having an actual emergency, at least what I’ve observed the last 5 years
3
2
137
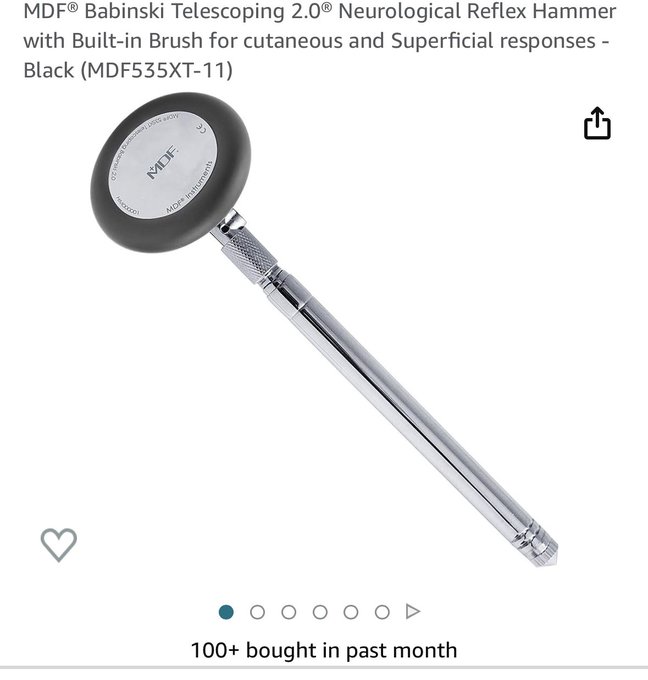
I recently bought this reflex hammer & I LOVE it. But… I decided to start doing reflexes on all my patients to get a better idea of physical exam variability and…
is this a reliable exam maneuver?
the variability is WILD!!
Neurologist, neurosurgeons, orthopedic - thoughts?
39
11
131
you don't want to electrically cardiovert a patient in AFRVR given the embolic risk (say, not on AC, > 24h in rhythm), but then you order amiodarone bolus and infusion...
10
13
129
@SPuro88
it’s because people in the U.S. have a fast food expectation for healthcare services, especially in the ED where they can get huge work-ups and avoid a hospital admission but still angry their soda didn’t have ice in it or it took 8 hours
5
7
114
And yet again (another paper on this topic!), more evidence that many, many medications that we used to think REQUIRED a central line or IO in fact do not...
Safety of peripheral 3% hypertonic saline bolus administration for neurologic emergency
9
28
111
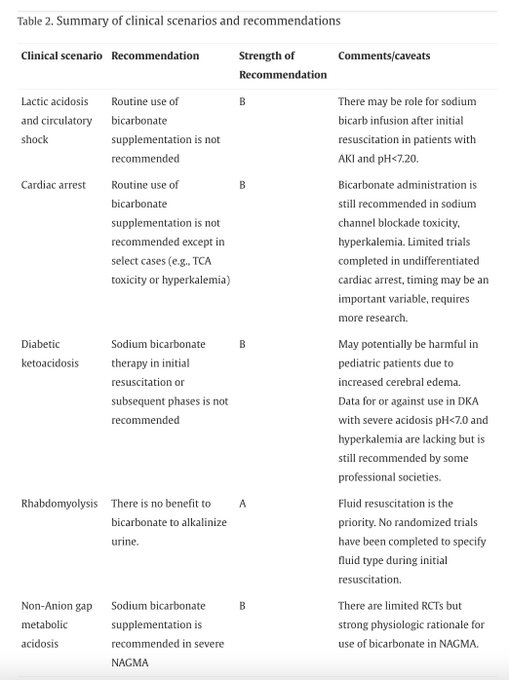
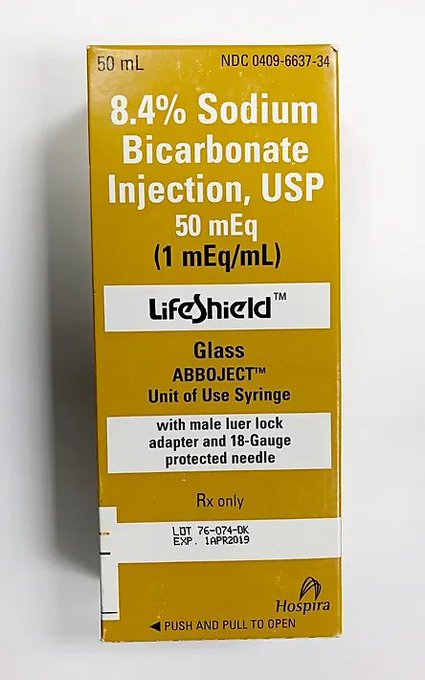
Great thread!!!!!! Good reminder hypertonic bicarbonate is not recommended by the AHA for all-comers in ACLS.
It’s always terrible when in a code, the code leaders continues to give bicarbonate, and it’s a prolonged code 2/2 to continual “we got a transient increase in ETC02!”

You've probably heard that Bicarbonate has to turn into CO2 to raise the pH. “Don’t give bicarb if you can’t increase ventilation.”
But how much CO2 is there in an amp of sodium bicarbonate?
A bicarb 🧵
1/
97
1K
4K
7
15
111
my favorite case of aortic dissection was when the CTA didn't show an AoD, but our pre-test probability was still super high and we did aggressive HR / BP control and admitted to the CVICU anyway, and repeat imaging 6 hours later showed the dissection, pt had great outcome.
10
7
110
Some of y’all clearly work in EDs where patients have easy access to primary care! I suspect a lot of this drives differences in clinical decision-making
10
3
109
Diastolic BP is probably one of the most ignored vitals

A patient presents in shock:
BP is 100/35
A wide pulse pressure (low diastolic) is suggestive of a distributive shock
With an important exception
👇
1/
#FOAMcc
#foamed
#MedTwitter
10
239
1K
7
5
107
I’m so happy right now — meet Greta! She’s 8 weeks old. 8hr drive to Madison here we go!

6
1
107
I really love emergency medicine. I’m glad I chose this career.
5
2
99
Since it's abundantly clear most have not read these asymptomatic HTN papers, let's see if our pt w/ BPs > 240 / > 130 are represented
They are GREAT papers and I cite them frequently on shift! Patients at the tail of the bell curve are not well-represented here in these studies
4
11
93
Four- and three-year emergency medicine residency graduates perform similarly in their first year of practice compared to experienced physicians
6
15
97

Going to one of the best ERs in the world —
@TamingtheSRU
.

I’m told Damar Hamlin has a pulse, but is not breathing on his own. He is being transported to UC.
Needed AED and CPR on the field.
4K
34K
224K
1
13
94
is anyone actually starting methylene blue in septic shock before norepinephrine levels reach 0.5mcg/kg/min..... interesting commentary in
@accpchest
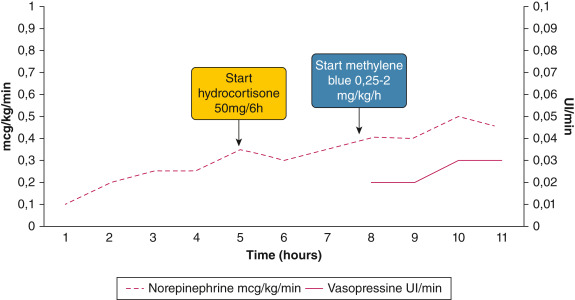
11
13
93
@AlanaKinrich
there’s been a few calls to the ED I’ve overheard recently where outpatient doctors are furious a patient is waiting 5-6 hours in the waiting room when they are 1) not acutely ill and 2) > 60 people in the waiting room… and it’s abundantly clear they have ZERO clue how EDs work
3
5
94
Incredible- I read every comment and thank you!!! 🙏🏻🙏🏻🙏🏻
Heading into my first EM attending shift today!!!!
First EM attending shift next week. Pro-tips and pearls appreciated.
58
4
182
10
0
91
@AlexJankeMD
It’s hard to be a medical student, hear all of this, see how crazy it is in the ED with boarding, dumb workforce papers that are crap, treating sick patients in the hallways, patients constantly yelling at us because of wait times, etc and think “hey! this looks fun!!”
6
2
92
Management of atrial flutter and atrial fibrillation with rapid ventricular response in patients with acute decompensated heart failure: A systematic review

1
18
88
driving back to Baltimore tomorrow for my last 6 shifts of residency and residency graduation-- officially done w/ residency on June 22!
8
0
82
I’m convinced most* physicians have no idea what the evidence is for what they do or do not do, but rather practice based on how they were taught in residency and/or hospital pathways that are implemented.
*
#medtwitter
is a great cohort of curious docs! But not representative

If you think the guideline is too aggressive/not aggressive enough, let's have the debate. I agree w
@srrezaie
re the data. But whether you agree or not, don't pretend the GL says something it doesn't & use that as fuel to criticize docs doing what they think is right for the pt.
0
1
10
9
10
81
"Medicare patients aged 65 to 89 years treated by emergency physicians aged under 40 years had lower 7-day mortality rates than those treated by physicians aged 50 to 59 years and 60 years or older within the same hospital." |
@AnnalsofEM
9
16
80
almost 3.5 years into residency and i still think … dang, so cool I get to train
@HopkinsMedicine
and
@JohnsHopkinsEM
#letsgo
#teamnights
!

0
0
76
@EMFFguru
none of these rules out pulmonary embolism though -- this just helps push us away from thinking that if there is a pulmonary embolism present, there is no electrocardiographic or ultrasound findings of submassive pulmonary embolism or acute pulmonary hypertension
@LWestafer
4
0
77
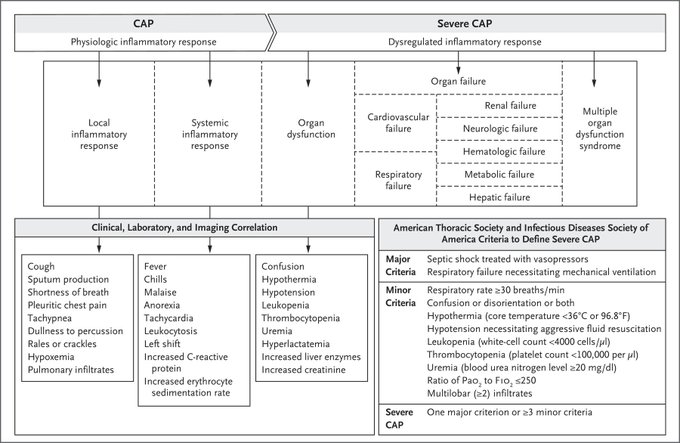
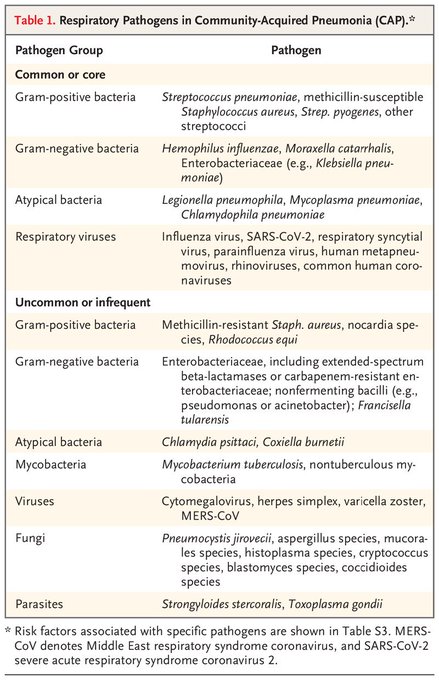
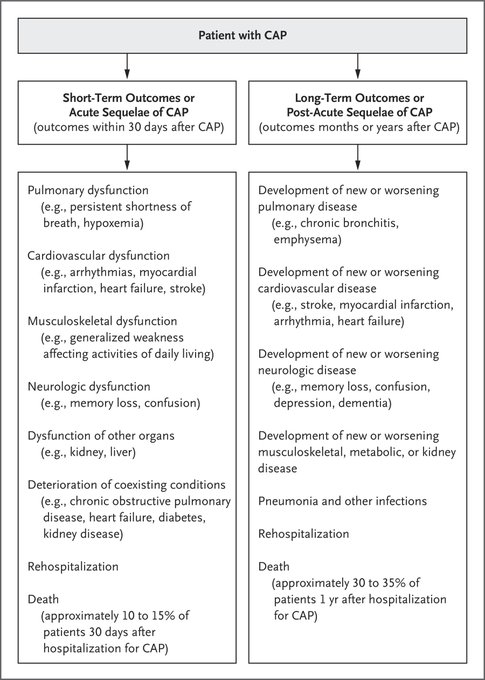
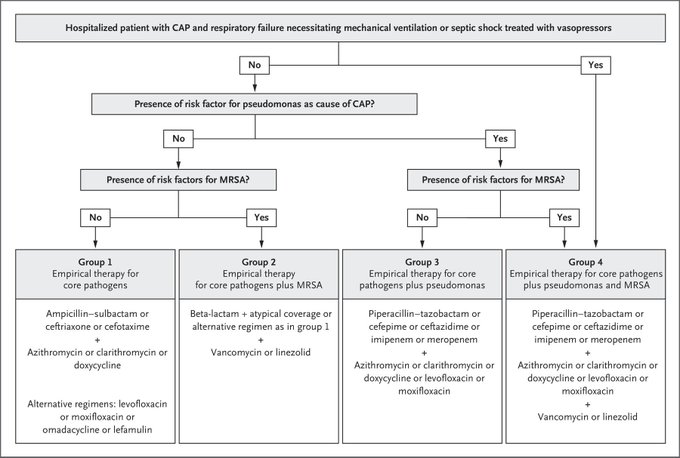
Nice brief overview of community-acquired pneumonia in
@NEJM
(August 2023) looking at pathogenesis, common pathogens, short/longterm outcomes, empiric therapy, and areas of uncertainty.
One of my favorite topics to talk about on-shift in the ED!
3
18
76
Steroids: 5 Pearls Segment | Core IM Podcast

0
12
72
In pts with traumatic fractures, NSAIDs appear to reduce post-trauma pain, reduce the need for opioids, have small effect on non-union
@EAST_TRAUMA
/ OTA conditionally recommend NSAIDs for traumatic fx: benefits outweigh the small potential risks.
3
19
70
🔥 article in
@JournalGIM
SpPin and SnNout Are Not Enough. It’s Time to Fully Embrace Likelihood Ratios and Probabilistic Reasoning to Achieve Diagnostic Excellence
I find these more confusing than just knowing the definition of sensitivity / specificity

8
16
71
POC STI testing in the ED with 1 hour turnaround time for results!!! 🙌🏻🙌🏻🙌🏻🙌🏻🙌🏻
#antibiotic
#stewardship
8
1
71
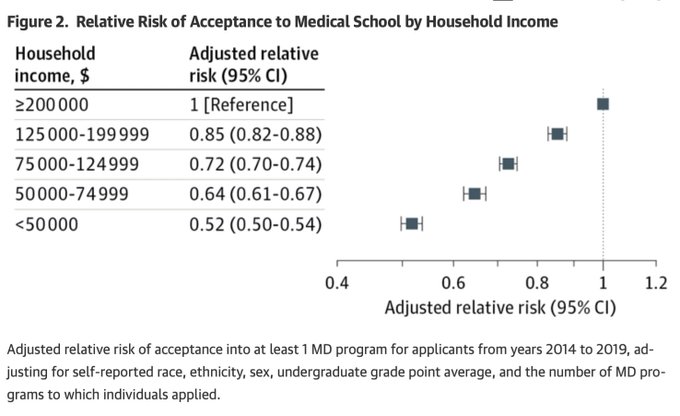
I was in this cohort of medical students (2014) and in the <<< $50k group. Still surprised I made it into medical school tbh...
9
3
69
Excited to start my new faculty job in July! Excited to be coming back to the Midwest 😍
Now if only the rental market wasn’t so 🔥🔥🔥 haha
8
0
68
I'm not going to comment on VIP treatment or NYU EM specifically, but what I will say, and what is abundantly clear in this article, is that NYU in general seems to have a fabulous track record of publicly gas lightning it's physicians / trainees over the last handful of years.

For years, New York University's emergency room has secretly given priority to donors, trustees, politicians, celebrities, and their friends and family, a New York Times investigation has found.
55
175
533
9
3
68
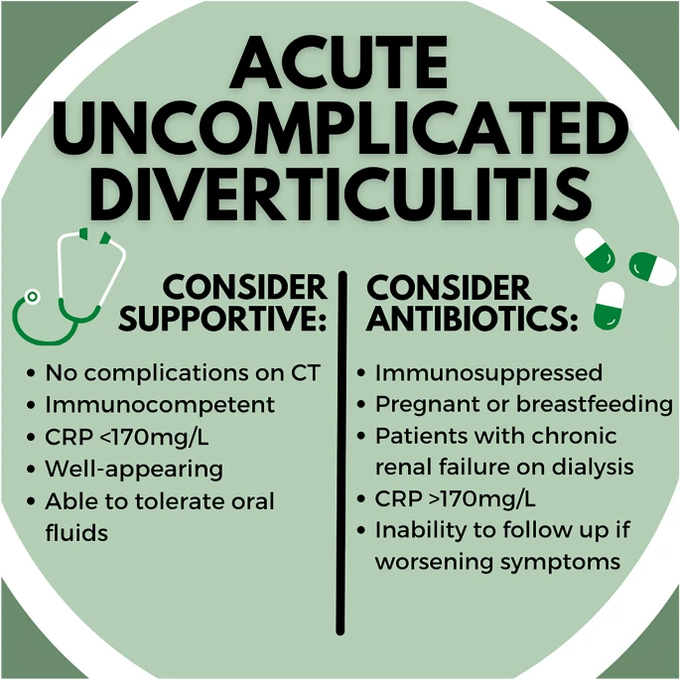
Just the facts: revisiting the role of antibiotics in acute uncomplicated diverticulitis |
@CJEMonline
what's your practice?
7
22
66
a lot of people on here (consultants, especially) have no idea what it's like in the ER with our current volumes and it shows... it's sad to see so many people in other specialities who clearly hate their jobs or their practice environment.
1
1
66
Each 0.3 mEq drop in potassium below normal correlates with an approximate 100 mEq total body deficit.
#RoshReview
#EMBoards
1
13
64
Graduation tonight
Last shift of residency tomorrow (7am 😂)
Pick up our new puppy in Ohio on Friday
Back *home* to Wisconsin on Saturday
4
0
63
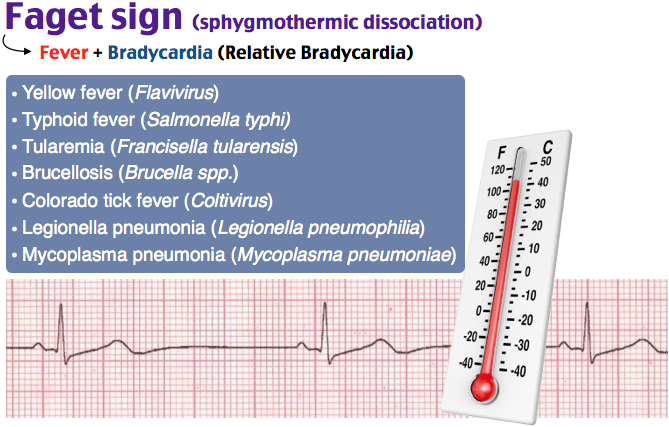
I think given how many people are on beta-blockers and/or have autonomic dysfunction (older age), Faget sign is likely highly unreliable at identifying which organism a person is infected with.
#RoshReview
#EMBoards
8
14
63
It Is Chloride Depletion Alkalosis, Not Contraction Alkalosis

4
16
61
The apps I use most frequently and couldn't live without:
-
@emrap_tweets
Corependium
-
@PyrlsApp
-
@PathwayMedical
-
@unboundmedicine
Johns Hopkins Guides
-
@mdcalc
-
@WikEM_org
3
10
61

Ah yes it’s radiologist bashing on emergency physicians day today.
21
1
56
My final EM conference presentation of residency is this coming Friday. PGY4s
@JohnsHopkinsEM
do a "Case Conference" where they present a number of cases, usually with a theme.
I'm not doing any exciting case, but focusing on the importance of mastering the basics of EM.
5
0
57
@blondemedSJW
@DRitterMD
I have a very low tolerance for verbal abuse to staff and trainees. It’s often the people NOT having the worst day of their life, as well as those often NOT having an emergency or something even urgent care worthy, who often are the most vulgar and verbally abusive IMHO
5
0
54
Note how much easier it is to access the subclavian veins when the shoulders are shrugged. Think about this when doing subclavian central lines. Cc
@PulmCrit
@emcrit

What it looks like as blood drains into the SVC from the upper extremities 🤯
Via
@CardioSurgPost
#MedTwitter
32
778
4K
3
17
55
ABEM… pay $480 to register for a website, then to pay $960 to register for the test. Clever, clever business model.
11
3
54
@Dr_mac2
Just finished my PGY4 year doing 90% supervisory shifts:
1. Trust but VERIFY; it’s still your responsibility
2. Don’t cut corners, but focus on what’s important for each patient
3. Be kind, they’re learning — being angry helps no one
4. Teach on-shift even if the Attendings don’t
2
3
54
So before y’all start dumping on her valid point, what’s the evidence-base argument that this makes better doctors?
We did pro-sections 2hr/week only in medical school.
Who’s to say virtual reality anatomy isn’t better?
Y’all need to think more critically as doctors tbh

We don’t talk enough about how horrifying it is that medical students spend months dissecting dead human bodies.
589
39
635
30
6
52