

Brendon Neuen
@brendonneuen
Followers
4,236
Following
1,656
Media
905
Statuses
6,666
Nephrologist & Director, Kidney Trials @NthSydHealth | @NHMRC supported @GeorgeInstitute Fellow | Secretariat, SMART-C | via @BrighamWomens @Oxford_NDPH
Sydney, Australia
Joined March 2009
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
Bronx
• 967481 Tweets
LOVTITUDE FANMEETING
• 717581 Tweets
namjoon
• 631957 Tweets
Rafah
• 370209 Tweets
Xavi
• 291675 Tweets
The ICJ
• 157363 Tweets
Flick
• 153101 Tweets
クロリンデ
• 100701 Tweets
LEAVE SEVENTEEN ALONE
• 100516 Tweets
Ten Hag
• 93966 Tweets
シグウィン
• 93937 Tweets
Laporta
• 88920 Tweets
Memorial Day
• 58346 Tweets
#SRHvsRR
• 49880 Tweets
Congratulations LISA
• 47027 Tweets
العدل الدوليه
• 41092 Tweets
McKenna
• 40718 Tweets
Coutinho
• 29953 Tweets
تشافي
• 29311 Tweets
Sokak Köpekleri Toplatılsın
• 26763 Tweets
Super Size Me
• 24820 Tweets
Morgan Spurlock
• 24495 Tweets
INEOS
• 23468 Tweets
#NickiAnnouncement
• 20843 Tweets
#تتويج_الهلال
• 18127 Tweets
Knives Out
• 18117 Tweets
Tyga
• 12396 Tweets
Kylie
• 10725 Tweets


















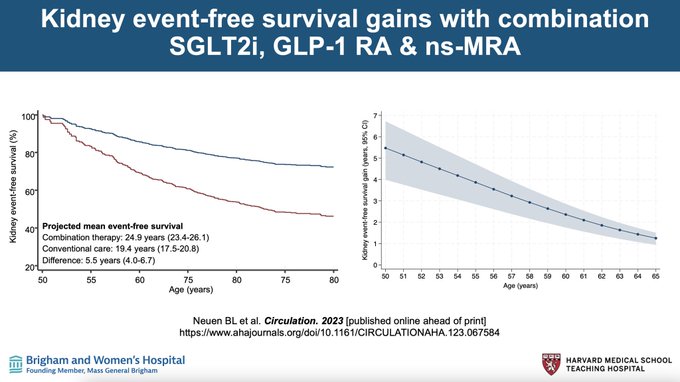
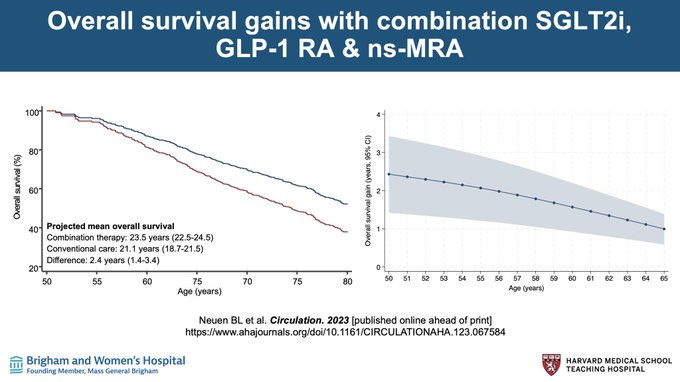
Pinned Tweet

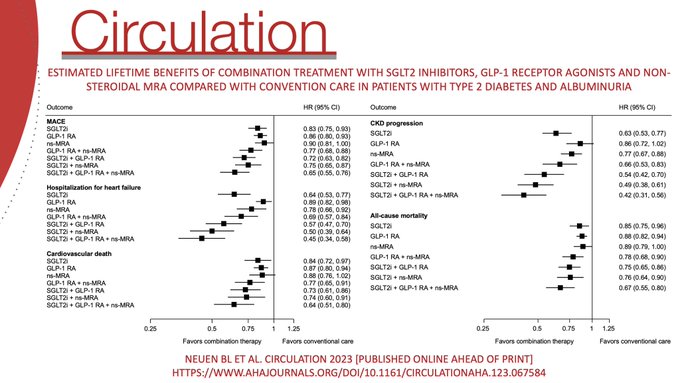
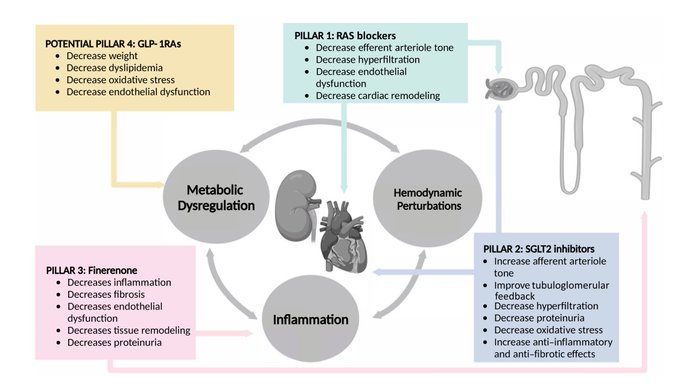
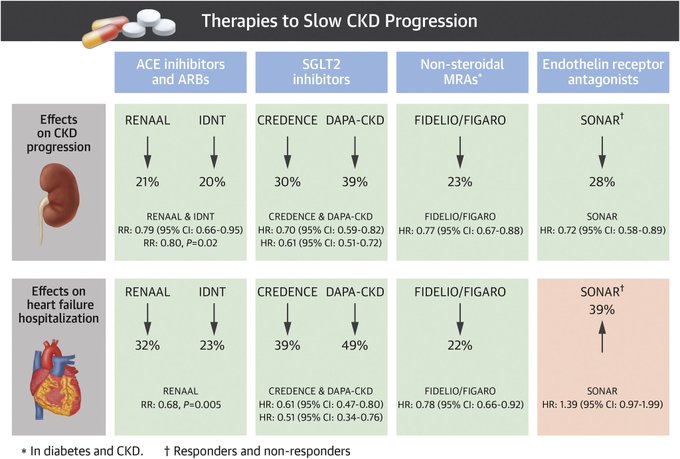
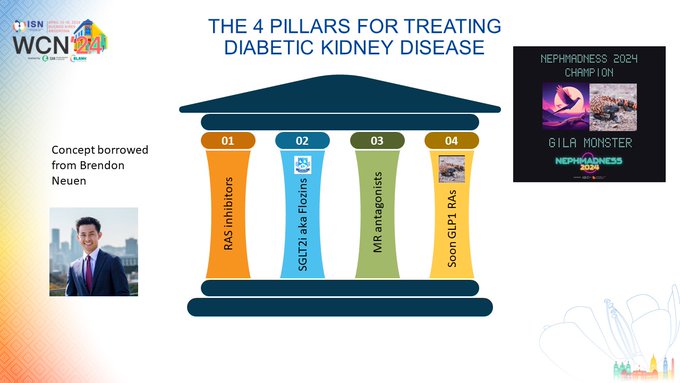
Time to implement the
#4pillars
of “kidney GDMT”
- RAS blockade
- SGLT2i
- ns-MRA
- GLP-1 RA
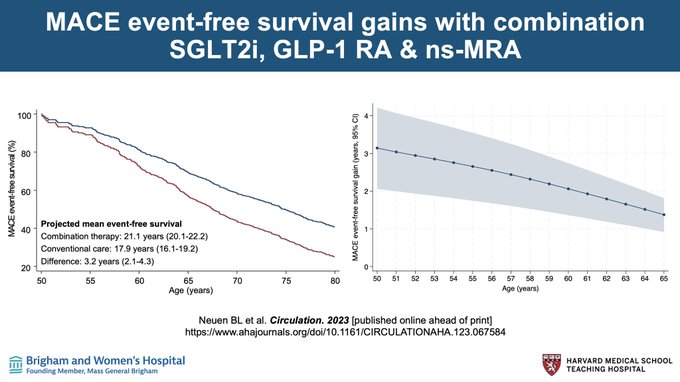
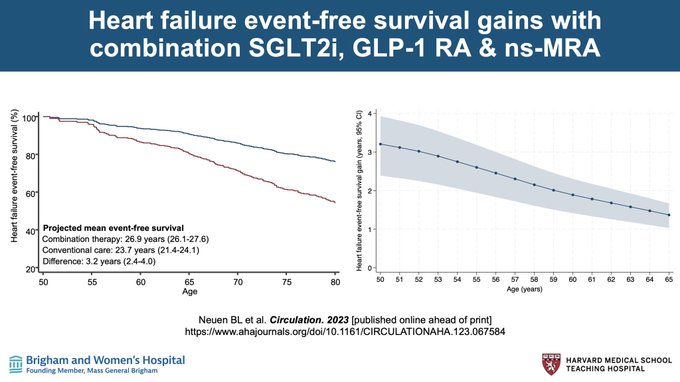
Lifetime cardiovascular, kidney & mortality benefits of combination therapy in people with diabetes with albuminuria
Now
#openaccess
in
@CircAHA
for
#AHA23
17
264
707
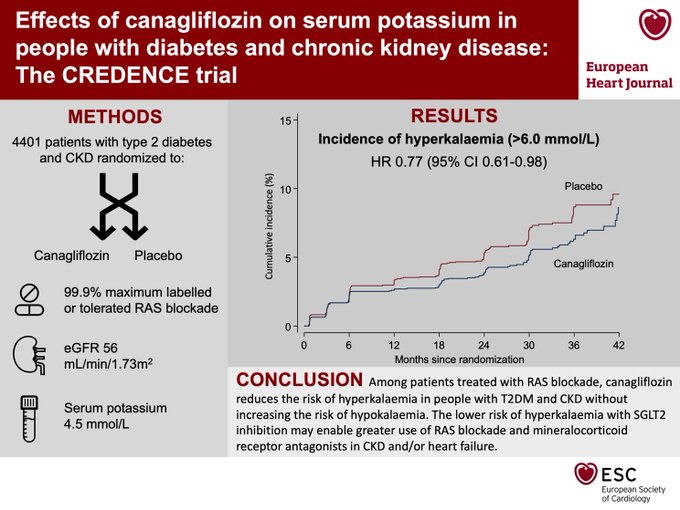
SGLT2 inhibition reduces the risk of serious hyperkalemia in people with diabetic kidney disease, which may enable greater use of RAAS inhibitors in CKD and/or heart failure
New CREDENCE data presented this week at
#ESCCongress
, now in
@ESC_Journals
:
10
217
527
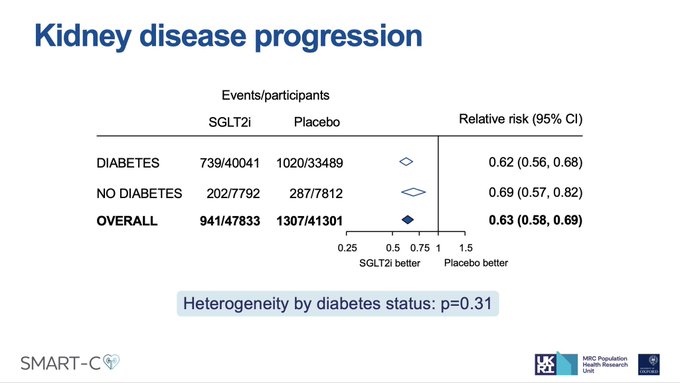
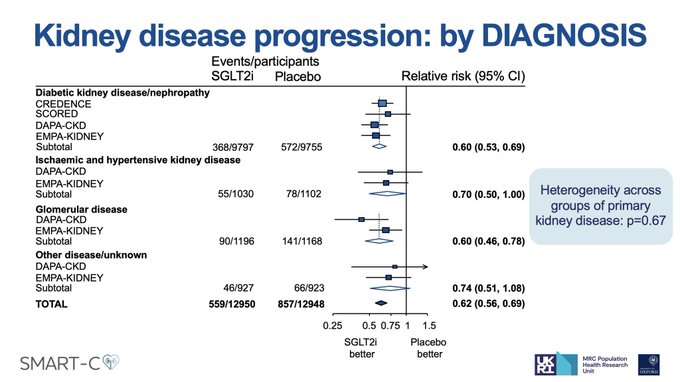
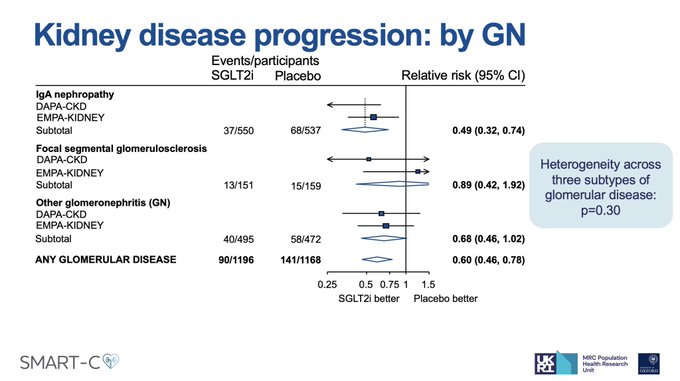
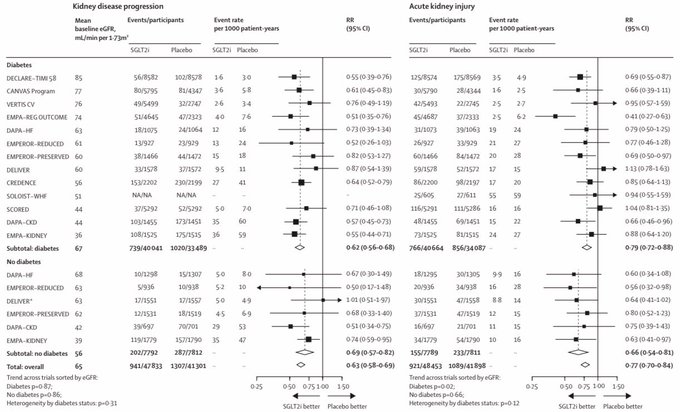
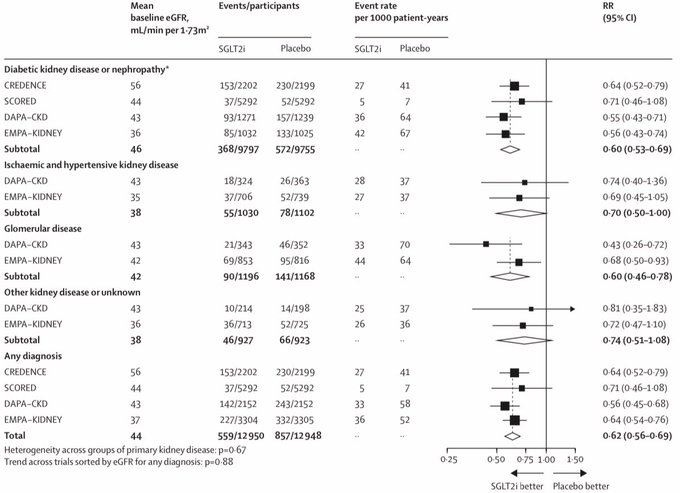
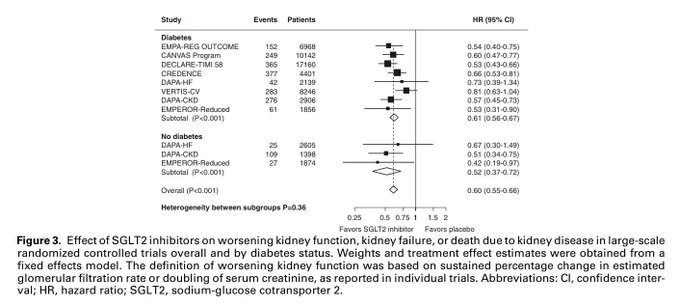
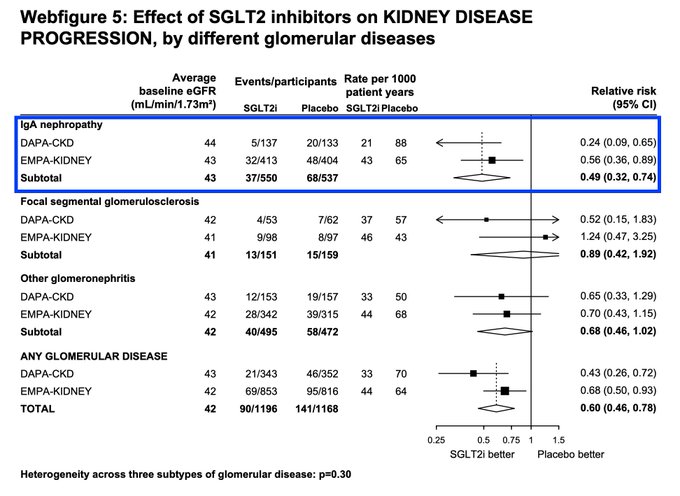
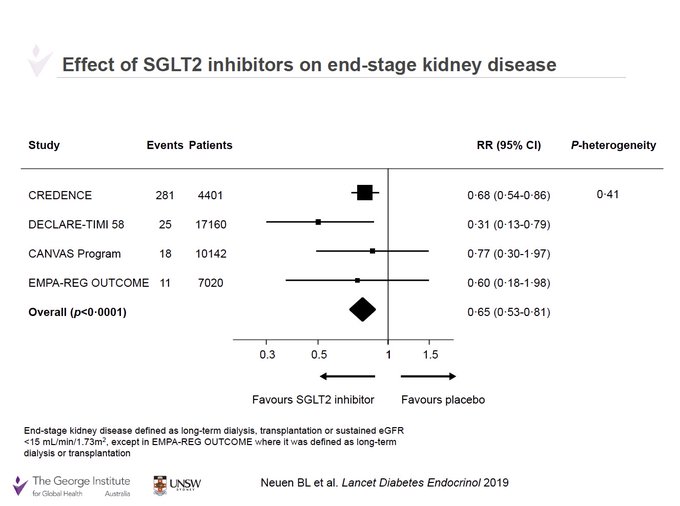
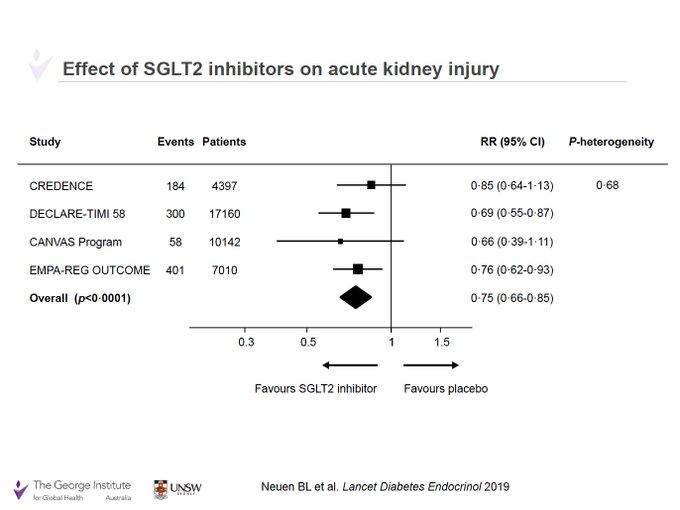
SGLT2 inhibitors reduce CKD progression by ~40%, regardless of:
- Diabetes
- CKD aetiology
- Type of glomerular disease
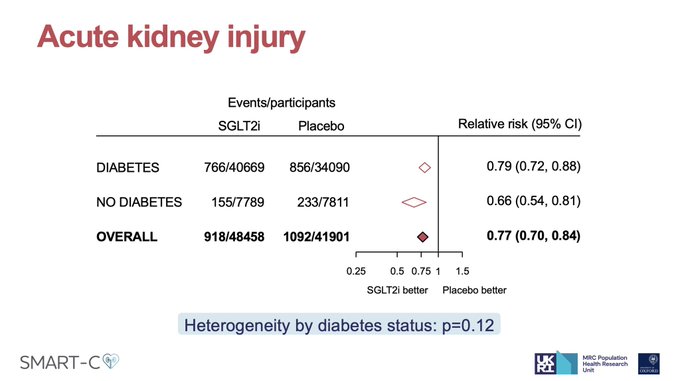
And reduces AKI by ~20%
Presented by
@NatalieStaplin
on behalf of
@Oxford_NDPH
Renal Studies Group & SGLT2 Trialists Consortium (SMART-C)
#KidneyWk
3
174
492
A remarkable transformation of care for people with diabetes and kidney disease in less than a decade.
Before? Limited to only to RAS blockade.
Now? Combination therapy with:
- RASi
- SGLT2i
- GLP-1 RA
- ns-MRA
4 pillars of care for diabetes & CKD
7
177
415
New
@TheLancet
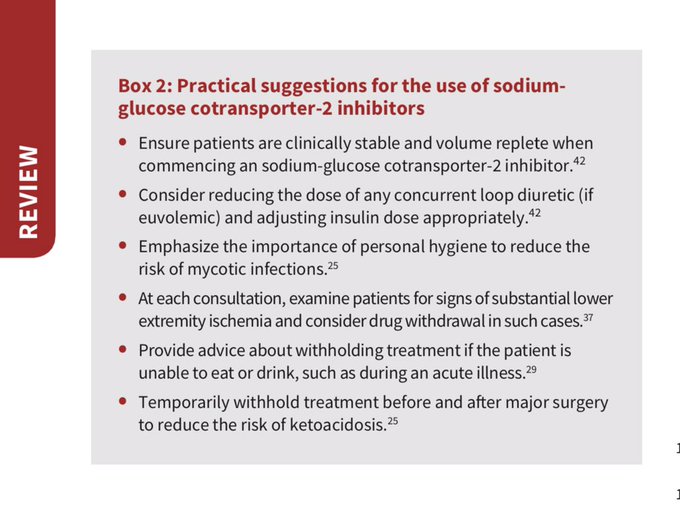
review on chronic kidney disease: Summarising the evidence for lifestyle and pharmacological strategies to preserve kidney function and improve outcomes
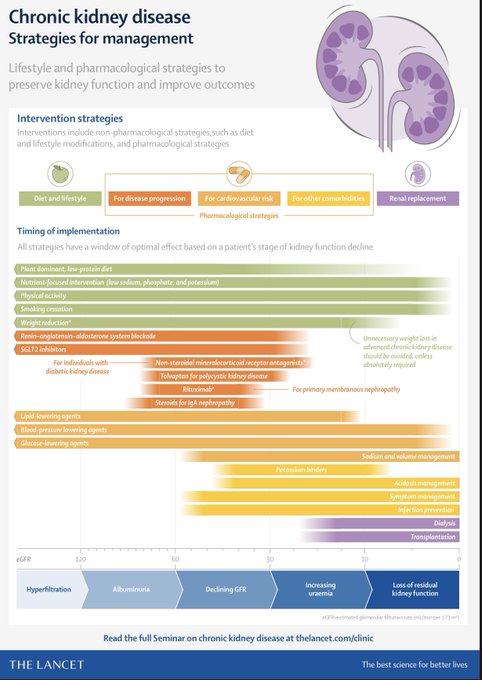
7
157
402
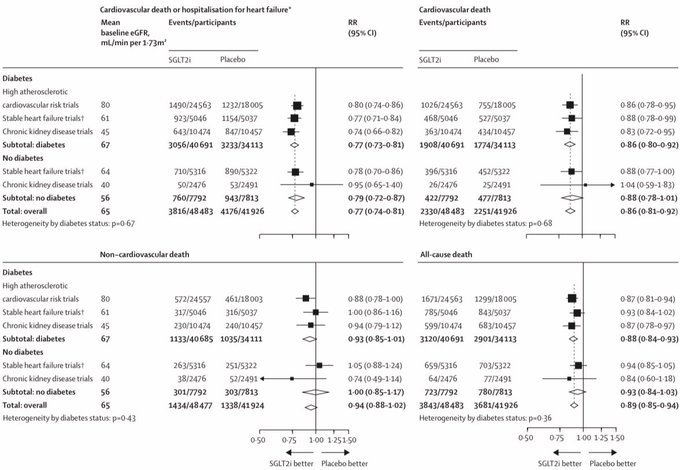
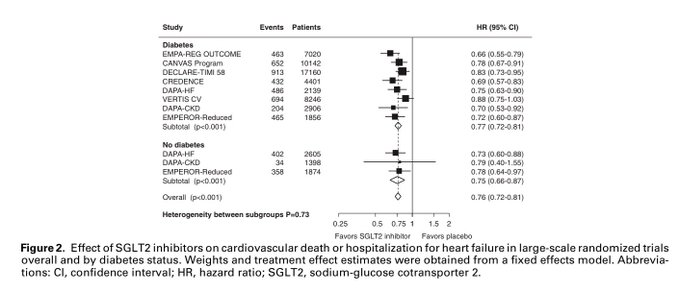
Our SGLT2 Trialists Consortium meta-analysis *the largest ever* in
@TheLancet
Definitive evidence that SGLT2i ⬇️:
- Kidney failure
- AKI
- CV death
- All-cause death
Regardless of diabetes
Led by
@NatalieStaplin
@RichardHaynes3
@willkidney
#AHA22
3
159
393
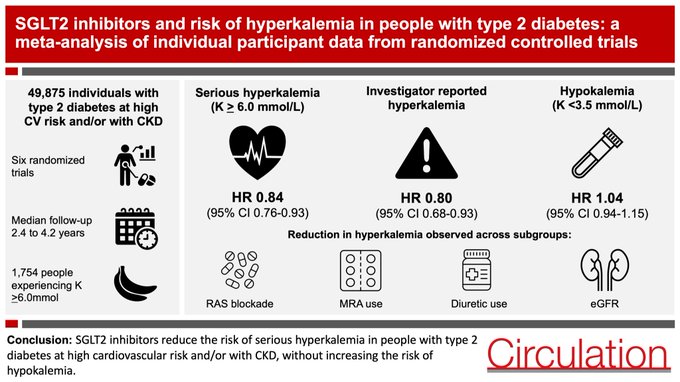
NEW
#openaccess
in
@CircAHA
SGLT2i reduces the risk of serious hyperkalemia (K>=6.0) by ~15% in people with diabetes, without increasing the risk of hypokalemia
This may facilitate better use of RAS blockade & MRAs to further reduce cardiorenal risk
8
148
390
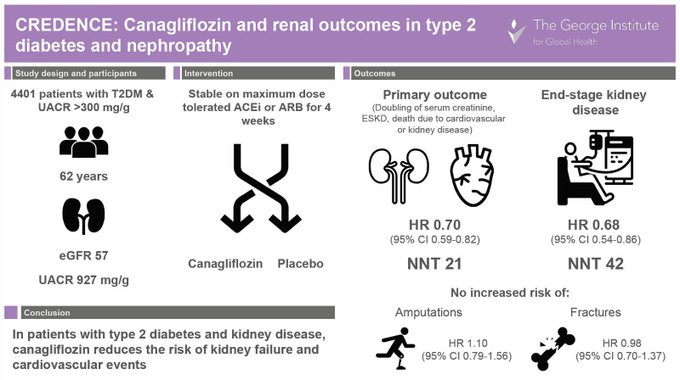
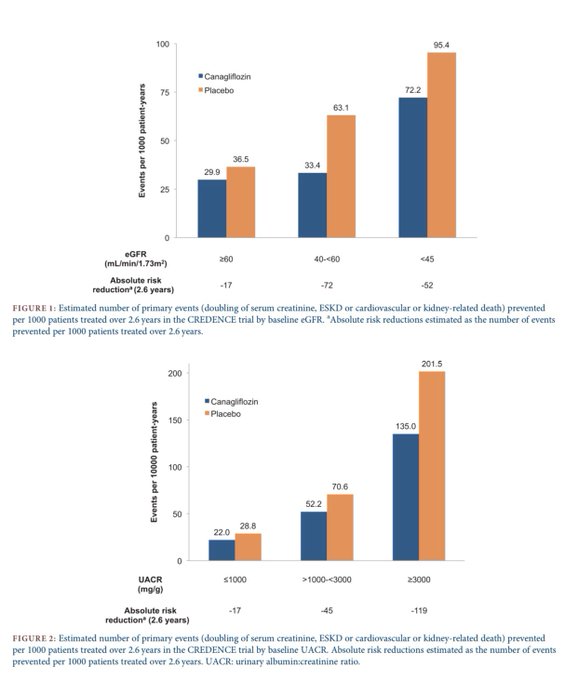
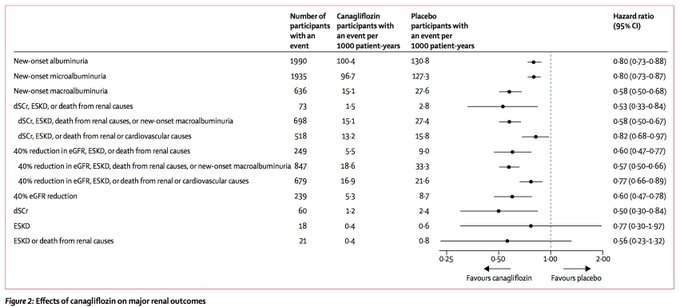
Canagliflozin reduces the risk of kidney failure or death due to cardiovascular or kidney disease by 30% compared to current standard of care.
Read the full CREDENCE trial now published in
@NEJM
#VisualAbstract
9
292
359
New insights from the CREDENCE trial on the blood pressure lowering effects of canagliflozin in type 2 diabetes and CKD now published in
@CircAHA
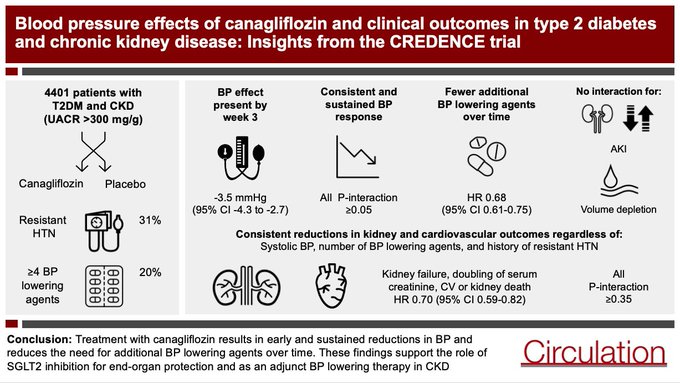
4
81
256
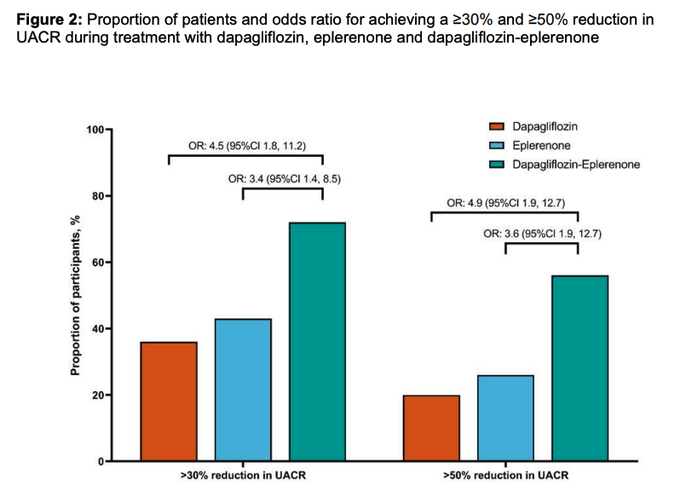
Important new randomized trial in
@JASN_News
from
@HeerspinkHiddo
et al.
- SGLT2i + MRA lowers albuminuria more than either alone
- SGLT2i attenuates increases in K associated with MRAs
Demonstrating efficacy & safety advantages of combination treatment
3
107
252
For a 50 year old patient with diabetes & chronic kidney disease, combination treatment with SGLT2 inhibitors & finerenone is projected to result in ~5 additional years free from kidney failure Our cross trial analysis of CREDENCE, DAPA-CKD & FIDELIO:
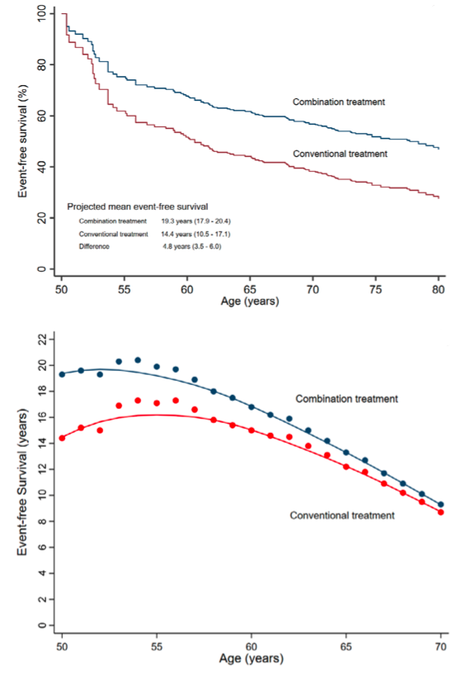
5
113
243
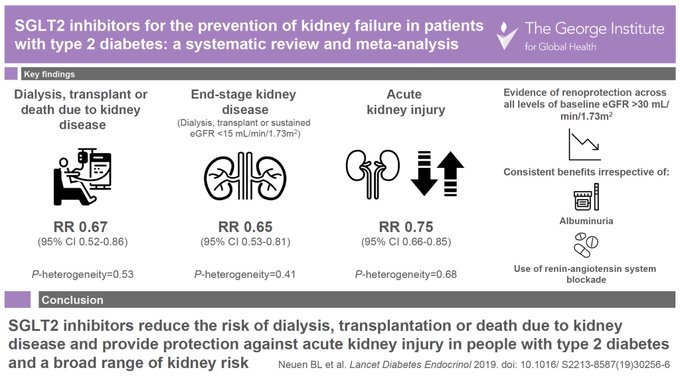
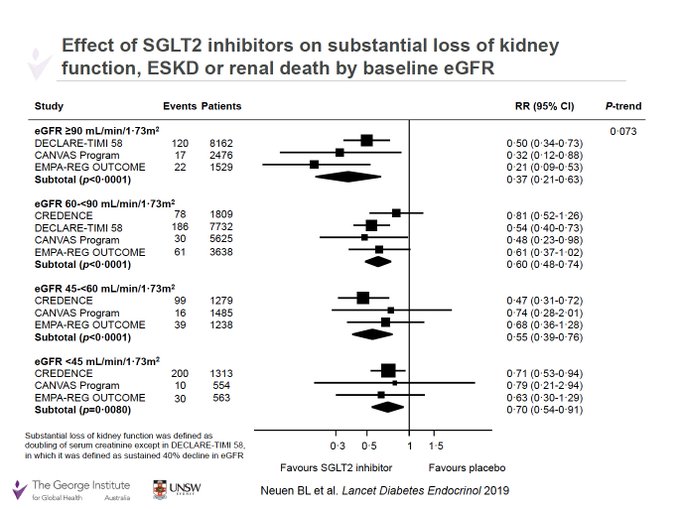
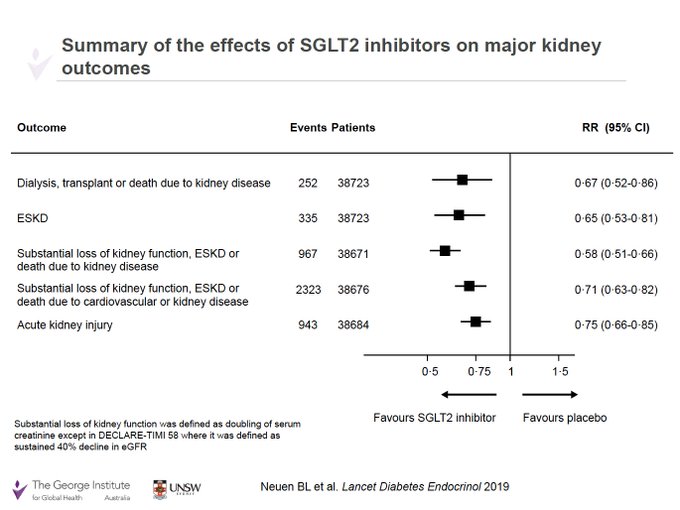
SGLT2 inhibitors reduce the risk of dialysis, transplant or renal death - the most important patient-centred renal outcome - AND provide protection against acute kidney injury
Our latest meta-analysis in
@TheLancetEndo
with
@jardine_meg
&
@VladoPerkovic
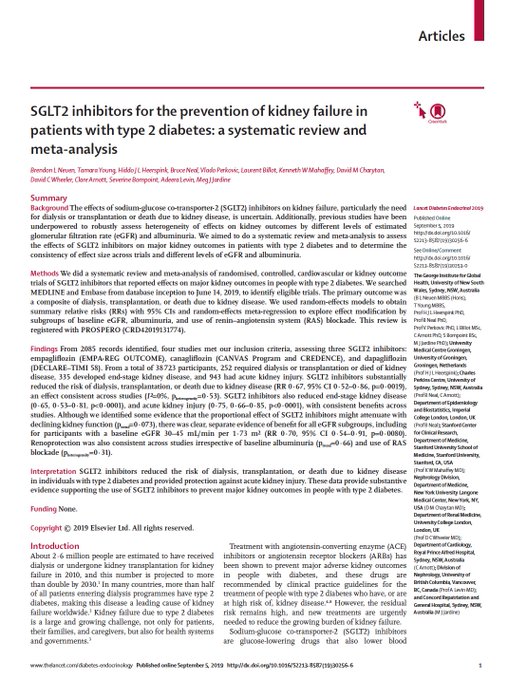
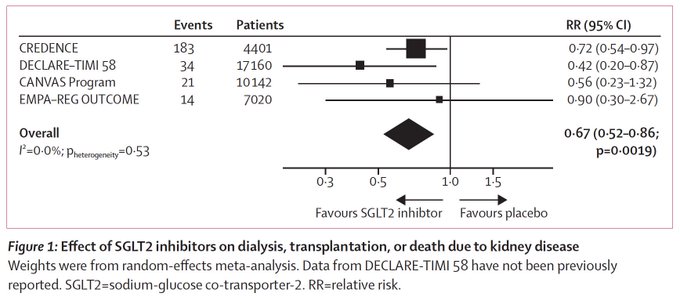
7
140
235
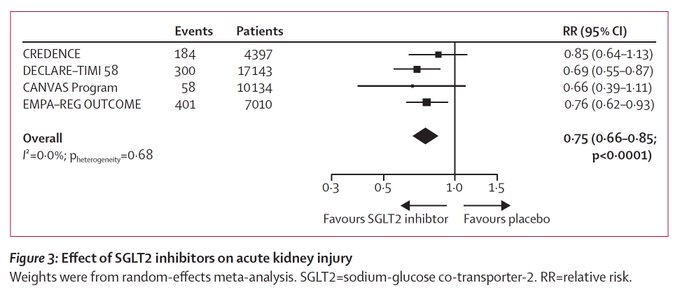
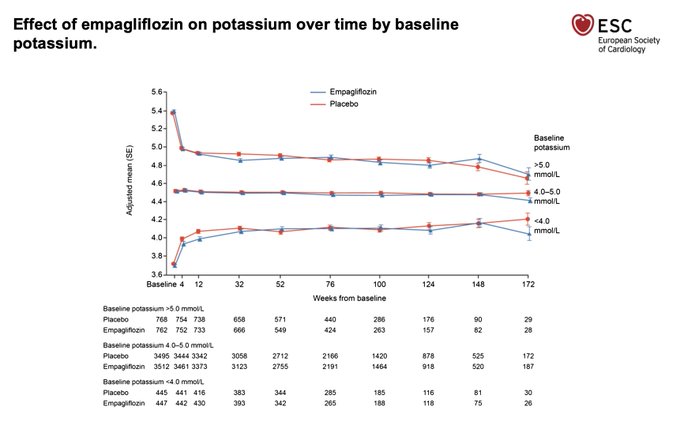
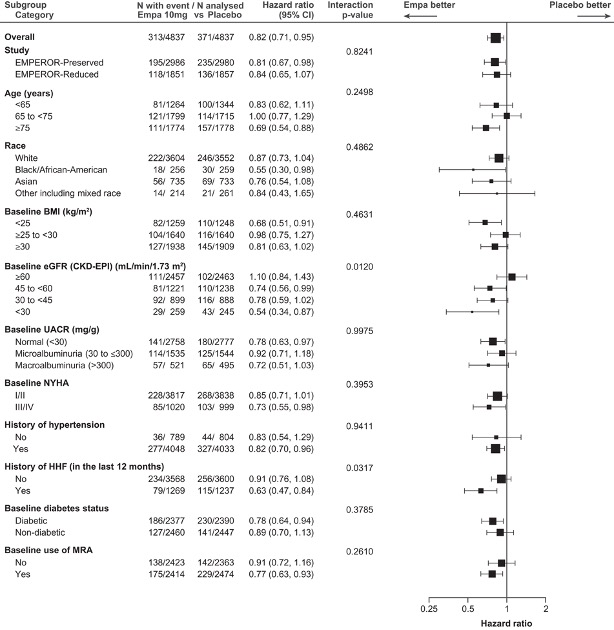
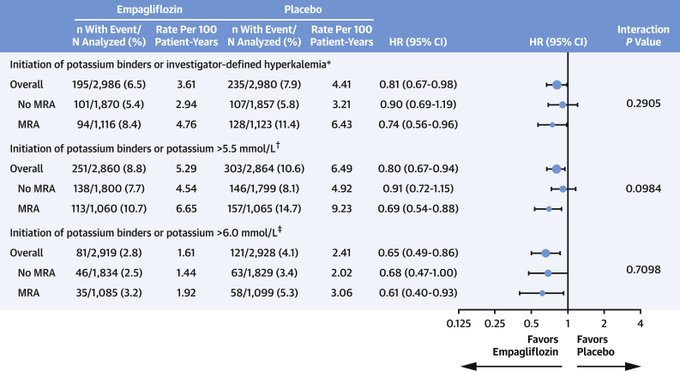
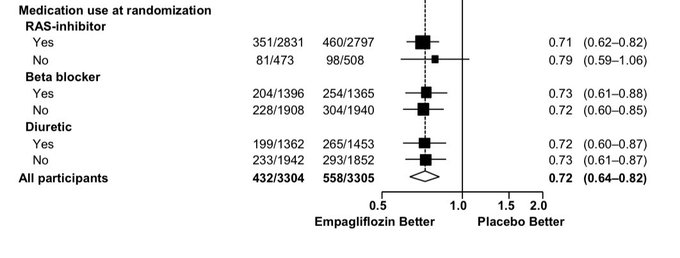
More evidence that SGLT2i ⬇️ hyperK, this time in heart failure
Empagliflozin reduces:
- K>6.0: HR 0.62 95% CI 0.48–0.81
- Investigator reported hyperK or K binders, HR 0.82 95% CI 0.71-0.95
- Effect modified by GFR - larger in CKD
- Regardless of MRAs
1
74
208
Announcement from
@novonordisk
re the FLOW trial:
Semaglutide reduced the risk of 50% decline in eGFR, kidney failure, or death due to kidney or cardiovascular disease by 24%
Results to be presented this year by trial PI
@VladoPerkovic
& colleagues

7
85
199
It’s not everyday that your primary supervisor is also the Dean of Medicine awarding your PhD 😀 A special day for me and my family
Thanks to everyone on here that I get to collaborate with & learn from - I’m extremely lucky and very grateful



Heartiest congratulations to
@brendonneuen
for successfully completing PhD under the supervision of
@VladoPerkovic
and
@jardine_meg
at
@UNSWMedicine
@georgeinstitute

12
4
93
28
6
189
I’m delighted to serve as founding Secretariat of the SGLT2 Trialists’ Consortium (SMART-C) with
@HeerspinkHiddo
Goal: Provide definitive evidence on the effects of SGLT2 inhibition on a wide range of outcomes in different patients
More soon
#KidneyWk
#AHA22
9
30
183
Our letter in
@NEJM
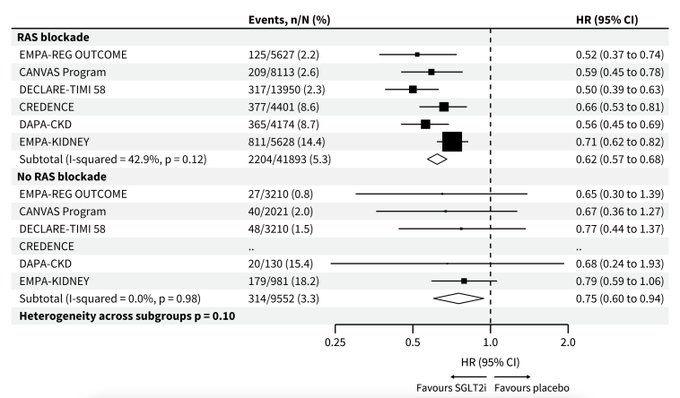
in response to the EMPA-KIDNEY editorial that suggested that the benefits of SGLT2i were "not as evident" in those not on RAS blockade:
Our letter was accepted with an accompanying figure, but was removed by the editors. Here it is:

2
58
175
A first in class observation for SGLT2 inhibitors:
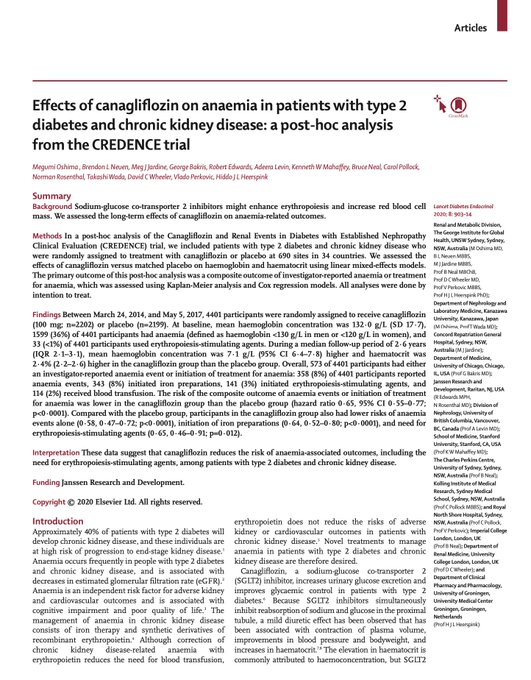
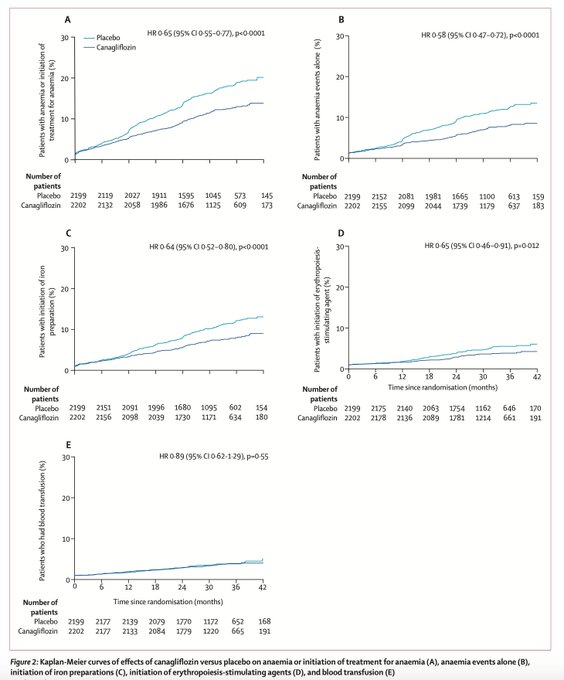
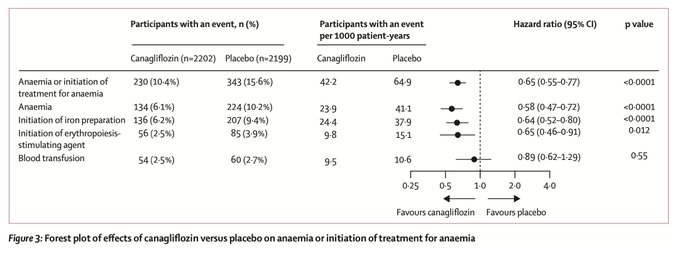
Canagliflozin reduces the risk of anemia-related outcomes, including the need for ESAs, in people with diabetic kidney disease
Our new findings from the CREDENCE trial now published in
@TheLancetEndo
5
61
173
Personal milestone for me: today I started as a consultant nephrologist & Director of the Kidney Trials Unit, Royal North Shore Hospital
@NthSydHealth
Really pleased to continue my affiliation w/
@georgeinstitute
as a Senior Research Fellow. Thanks to all who’ve supported me -
30
1
163
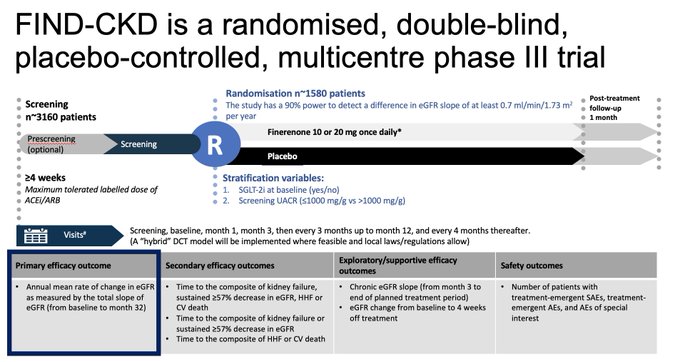
FIND-CKD is fully recruited!
Assessing the effects of finerenone in 1⃣5⃣8⃣4⃣ patients with non-diabetic CKD
Primary outcome: Total GFR slope to 32 months
Thanks to all investigators & patients worldwide who are involved in the
#FINDCKD
trial
3
41
151
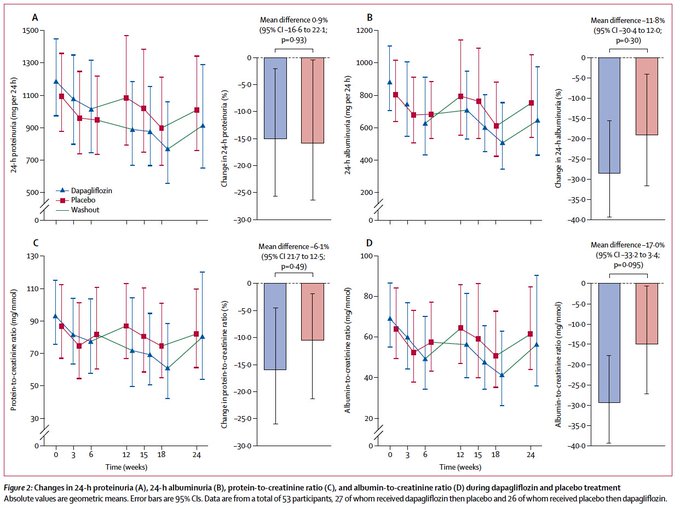
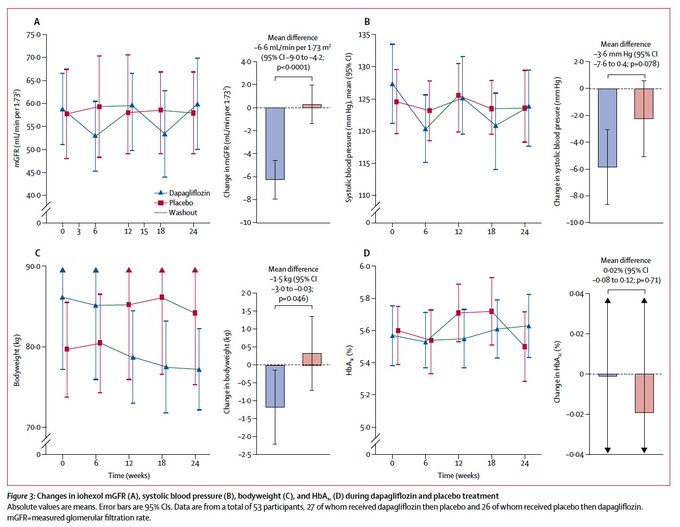
First in human RCT of SGLT2 inhibition in non-diabetic kidney disease. In this cross over trial, 6 weeks of dapagliflozin did not lower albuminuria, but did induce acute & reversible declines in GFR
Fascinating data whilst awaiting DAPA-CKD
7
76
137
For this patient, what might the ***lifetime*** cardiovascular, kidney and overall survival benefits be for combination treatment with:
- RASi
- SGLT2i
- ns-MRA AND
- GLP-1 RA?
Looking forward to presenting these data on Sunday morning at
#AHA23

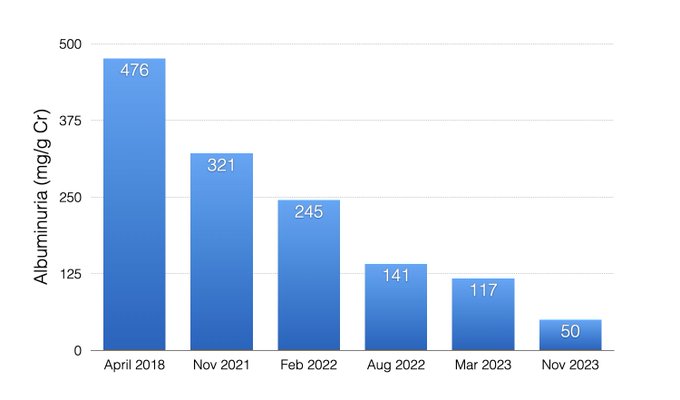
CKD Stage 3a with diabetes.
90% reduction in albuminuria with losartan, dapagliflozin, and finerenone.
26
68
383
4
26
132
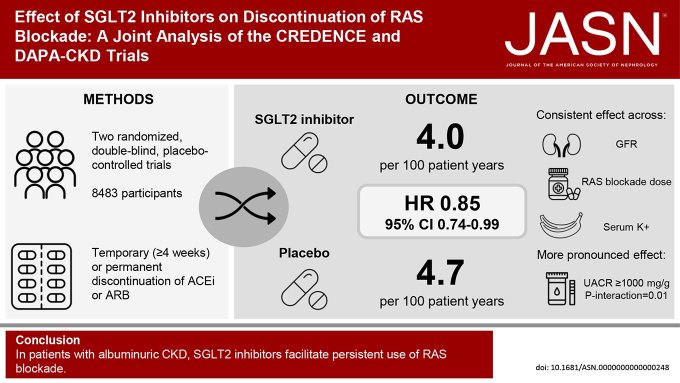
Strategies to enable persistent use of RAS blockade in CKD have long been sought after
In a joint analysis of CREDENCE & DAPA-CKD, we found that SGLT2i ⬇️ discontinuation of ACEi & ARB by 15%
Our latest work led by
@Fletcher_RA
, now online in
@JASN_News
2
58
128
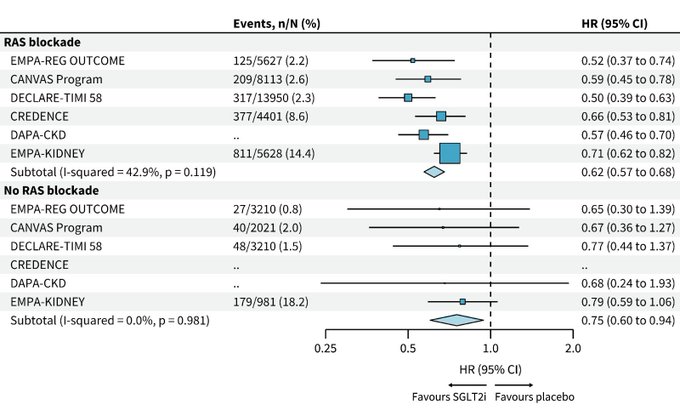
Pooled data after EMPA-KIDNEY:
No evidence that renoprotection with SGLT2i is modified by RAS blockade (P-interaction 0.10; figure by
@Fletcher_RA
)
Check out
@FreelyFiltered
for more
@kidney_boy
@hswapnil
@PriRenalAKI
@sophia_kidney
@Jwaitz
#nephjc
2
31
122
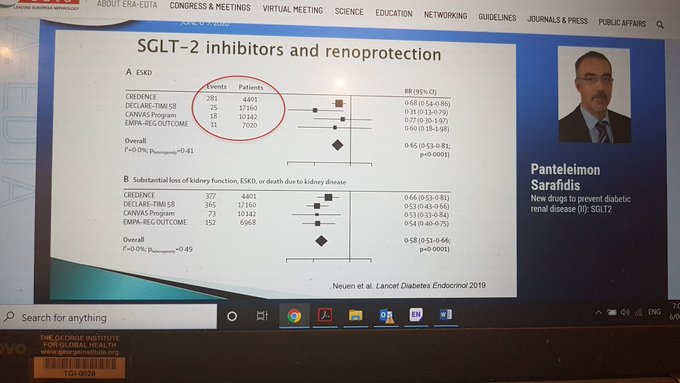
Are you looking forward to the presentation of the CREDENCE trial at
@ISNWCN
?
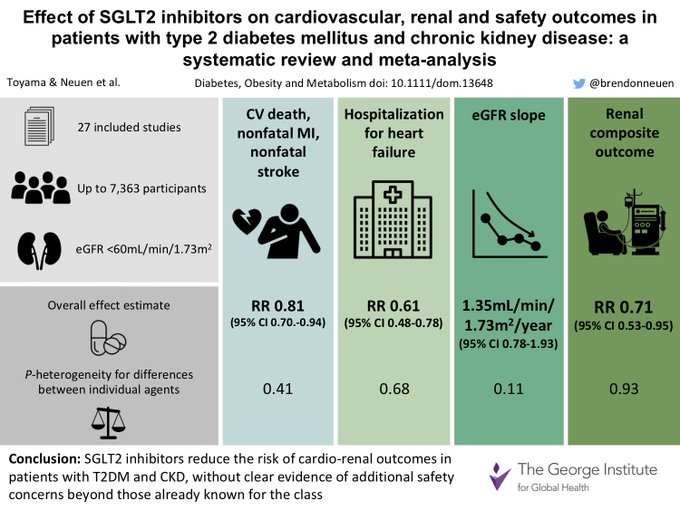
Check out our new meta-analysis, led by
@VladoPerkovic
, summarising data on the effects of SGLT2 inhibitors on CV renal & safety outcomes in CKD
#ISNWCN
#VisualAbstract
9
66
124
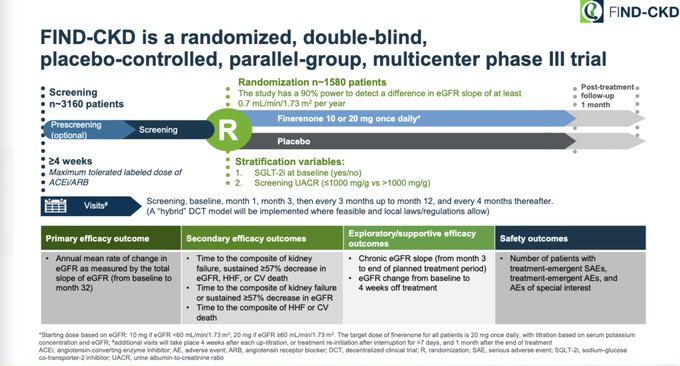
Introducing the FIND-CKD trial: evaluating the effect of the non-steroidal MRA, finerenone, on a primary outcome of total eGFR slope in approximately 1580 patients with non-diabetic CKD, with SGLT2i use permitted
#KidneyWk
6
42
122
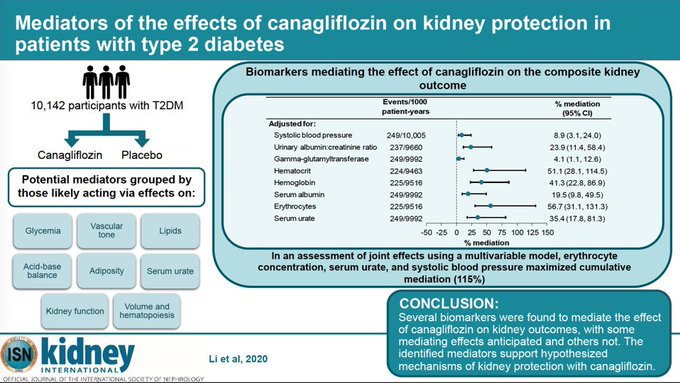
How do SGLT2 inhibitors slow progression of kidney disease in type 2 diabetes?
Our new paper assessing potential mediators of kidney protection with canagliflozin in the CANVAS trials:
Now published in
@Kidney_Int
:
3
48
117
44 years ago, my grandparents arrived in Darwin - they were lucky in every way from the sturdy boat, calm seas & help from Indonesia along the way. But the lottery moment was when Fraser welcomed them in with open arms. We are forever grateful
#Afghanistan
#Kabul
#auspol
@Kon__K



Fraser admitted 60,000 Vietnamese.
Australia has a moral, legal & political obligation to help the Afghans.
Australia—let’s start with helping Afghan refugees, living in Australia. They are living in destitution.
It’s is a cheap, short process. It just requires a signature.
12
174
670
4
19
112
Finally made the journey from Sydney to Boston! Looking forward to a really productive 6 months, working with
@mvaduganathan
@scottdsolomon
at
@BrighamWomens
/
@harvardmed
and
@LAInker
at
@TuftsMCKidney
on heart failure and CKD
All Boston recommendations welcome!


17
2
113
Canagliflozin, an SGLT2 inhibitor, is the first new drug approved to reduce the risk of end-stage kidney disease due to type 2 diabetes in almost 20 years.
Huge news, and a great outcome for patients
2
40
106
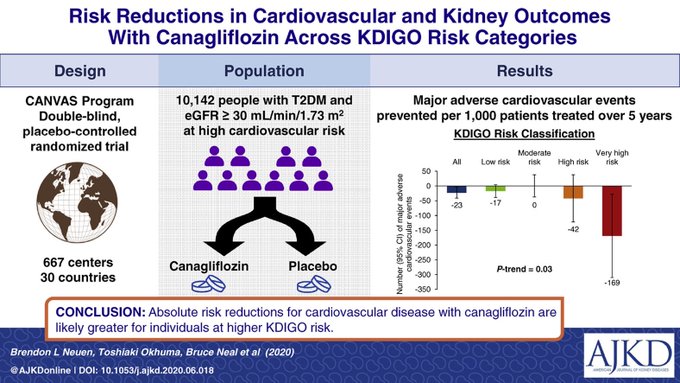
Delighted to share our latest paper with
@DavidCWheeler2
(DAPA-CKD co-chair), now published online in
@AJKDonline
Using the KDIGO classification system to identify people with CKD who might benefit most from
#SGLT2
inhibition
1
29
105
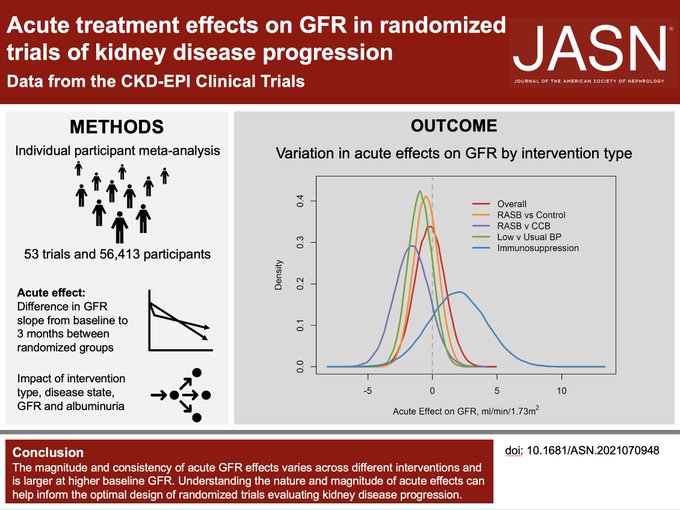
Many interventions (e.g. ACEi/ARBs, SGLT2i, MRAs, CNIs) have acute effects on GFR that differ from their long term effects
How can this affect the design & interpretation of trials assessing CKD progression?
🧵Our new CKD-EPI analysis now in
@JASN_News
:
3
33
106
Very grateful to receive an
@NHMRC
Emerging Leader Investigator Grant to support my work over the next 5 years 🙏
Look forward to working with many incredible colleagues to improve kidney disease care - so much work to do
@georgeinstitute
@NthSydHealth
@north_fndn

We're proud that four of our researchers have secured
@nhmrc
Investigator Grants!
Find out how these grants will help tackle some of the biggest causes of death and disease in Australia and globally
@daisyhcoyle
@brendonneuen
@julieB_Injury
@davidpeiris

0
3
28
17
6
107
Almost all guidelines recommend SGLT2i as 2nd line in T2DM & CKD/HF if not achieving glucose control on metformin
But should “metformin 1st for all” be revisited given the latest trial evidence?
A thread on metformin, guidelines & our new meta-analysis
6
30
104
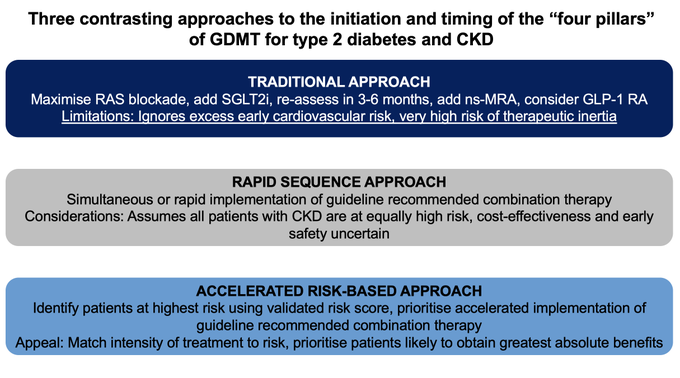
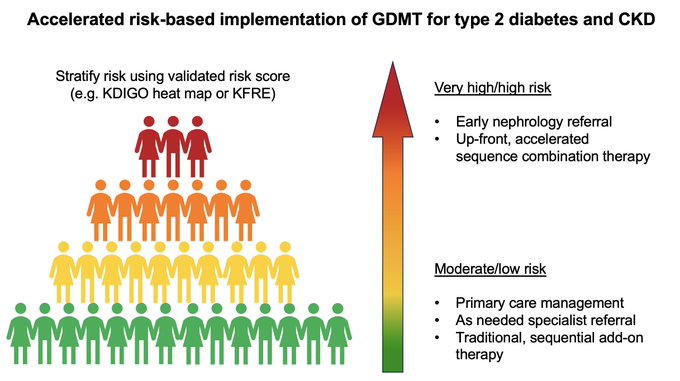
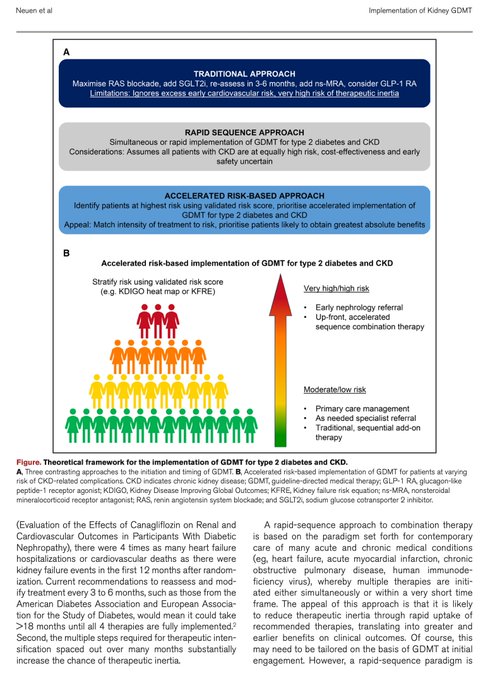
How can we prioritise accelerated therapeutic implementation of the "four pillars" of GDMT for diabetes & CKD?
-RASi
-SGLT2i
-ns-MRA
-GLP-1RA
@mvaduganathan
@KatherineTuttl8
& I outline what an "accelerated, risk-based approach" might look like
@CircAHA
2
35
101
It's finally up! Come & explore the SGLT2 Inhibitor Meta-Analysis Cardio-Renal Trialists Consortium (SMART-C) website
Find out about:
- Our goals
- Leadership
- Trials
- Publications
- Resources (SMART-C GitHub)
@DLBHATTMD
@scottdsolomon
@NatalieStaplin

2
35
100
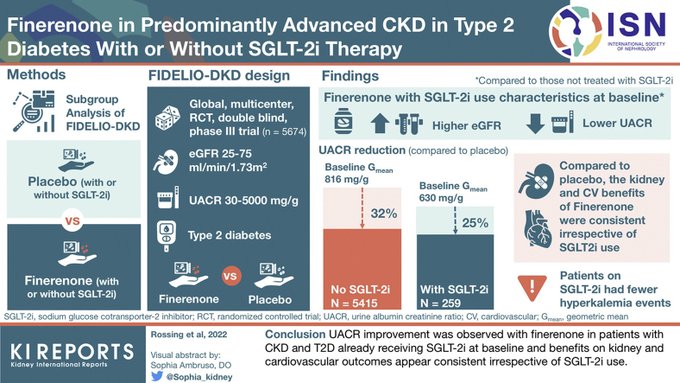
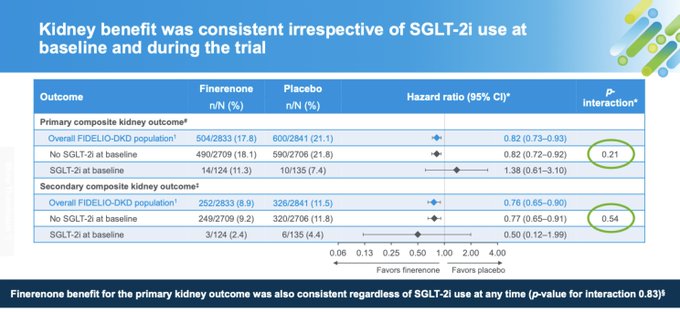
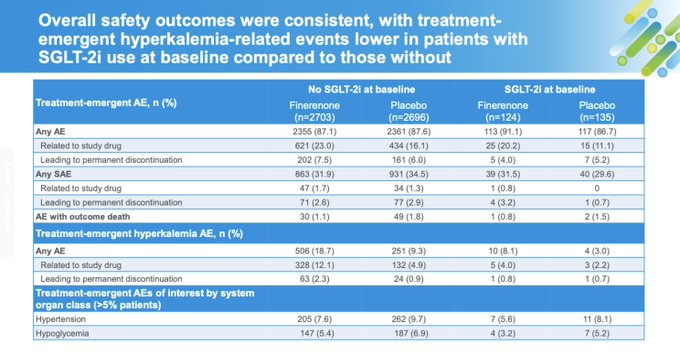
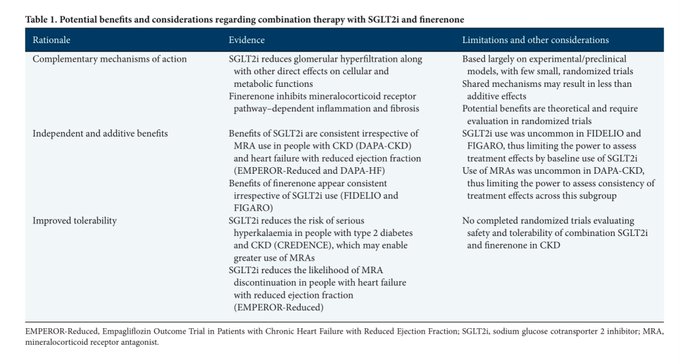
Important data form FIDELIO-DKD on combination SGLT2i + finerenone. Incidence of hyperK AEs was lower in SGLT2i treated patients, with no episodes of K>6.0.
Potential safety advantage of adding MRA to SGLT2i?
from
@P_Rossing
et al. in
@KIReports
0
31
99
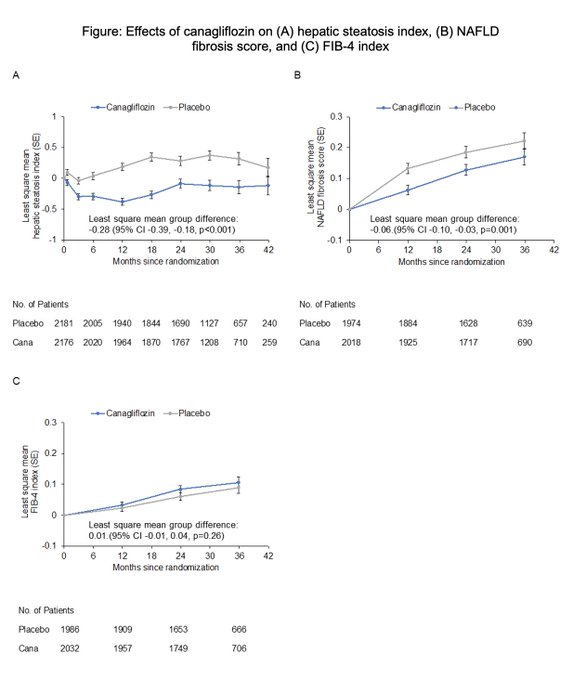
New data from CREDENCE:
SGLT2 inhibitors may improve liver steatosis/fibrosis, data which support further evaluation of this drug class in people with NAFLD
@fletcher_RA
@jardine_meg
@themahaf
@bakrisgeorge
@arnottclare
@VladoPerkovic
Free link:
0
28
99
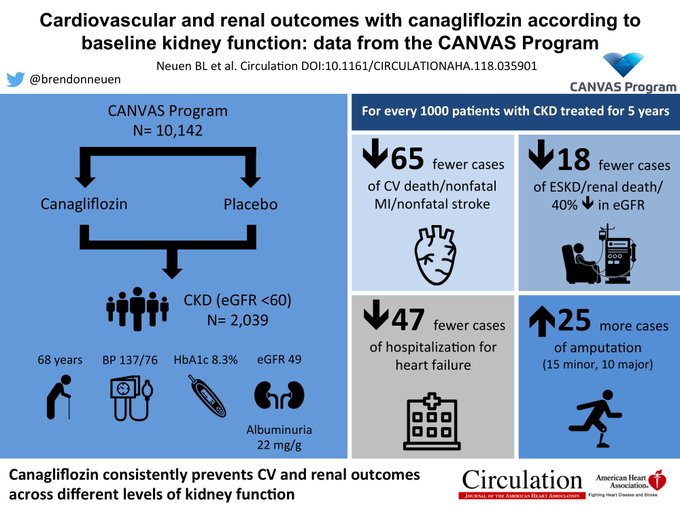
Our paper now parallel published in
@CircAHA
for
#2018ADA
!
*Open access*
Cardiovascular & renal outcomes with canagliflozin by baseline kidney function: data from the CANVAS Program
#VisualAbstract
Link:
Next: TWEETORIAL summary of the paper (1/9)
2
46
99
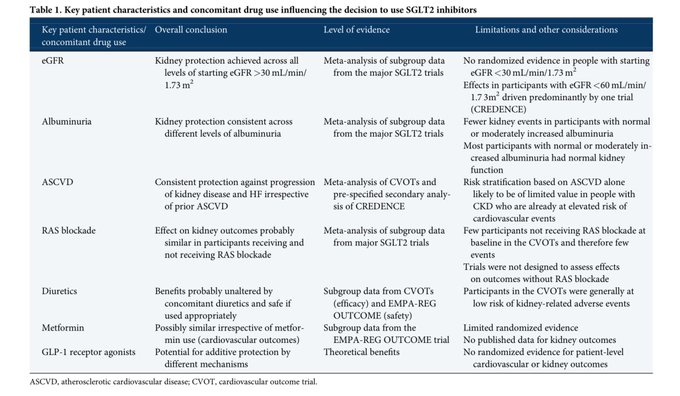
Which patients with CKD should be treated with SGLT2 inhibitors, today and in the future?
Very pleased to contribute to a special themed issue of
@NDTsocial
on
#SGLT2
inhibition with
@jardine_meg
and
@VladoPerkovic
Whole issue is free
#openaccess
2
29
98
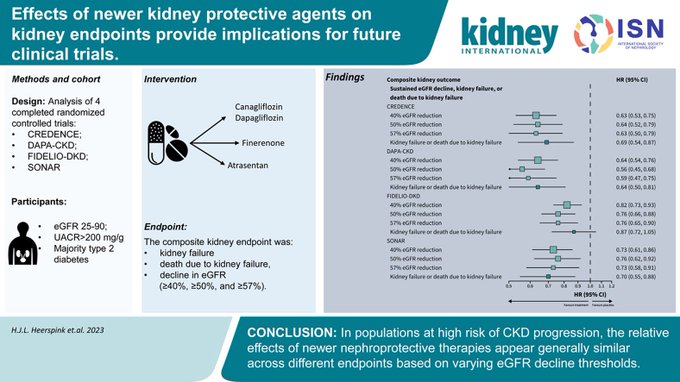
How does endpoint definition (40%, 50% or 57% decline in eGFR) impact the assessment of the effects of SGLT2 inhibitors, finerenone & atrasentan on kidney disease progression?
Our new analysis in
@Kidney_Int
now online:
1
43
96
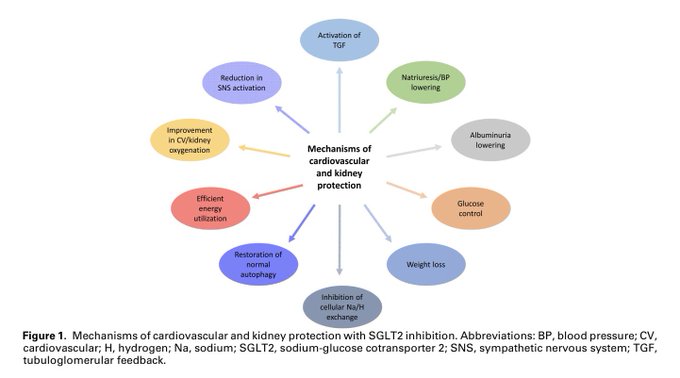
SGLT2 Inhibition: Rationale and Mechanisms for Kidney and Cardiovascular Protection in People With and Without Diabetes
Prof Carol Pollock AO & I summarise everything we do (and don’t) know about how these agents protect the heart and kidney

3
27
95
I was honoured to receive the Ida Browne Early Career Medal from
@RoyalSocNSW
last Friday
Thanks to
@AmandaMather7
&
@Emma_Olone
, who attended the ceremony at NSW Parliament House on my behalf
A testament to the incredible colleagues I am lucky to work with - in Sydney & abroad



Congratulations again to those honoured for their distinguished achievements at the Royal Society of New South Wales' Presentation of Awards on Friday night! The 2023 Career Excellence Awards went to
@HM_Christensen
,
@Qilin_Wang_
, Aunty Frances Bodkin, and
@brendonneuen
.
1
0
9
18
1
88
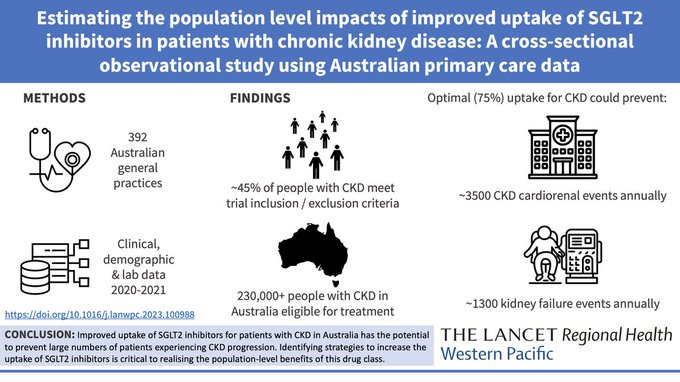
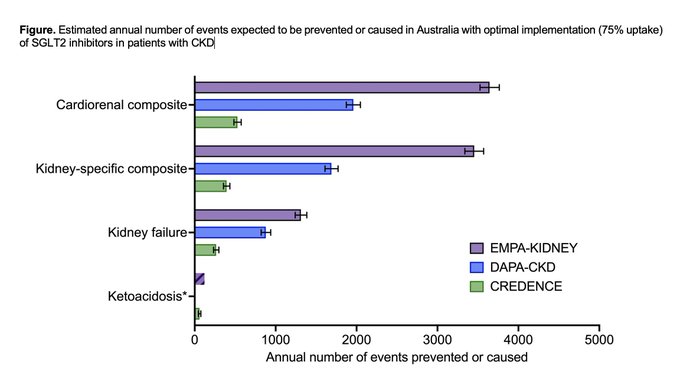
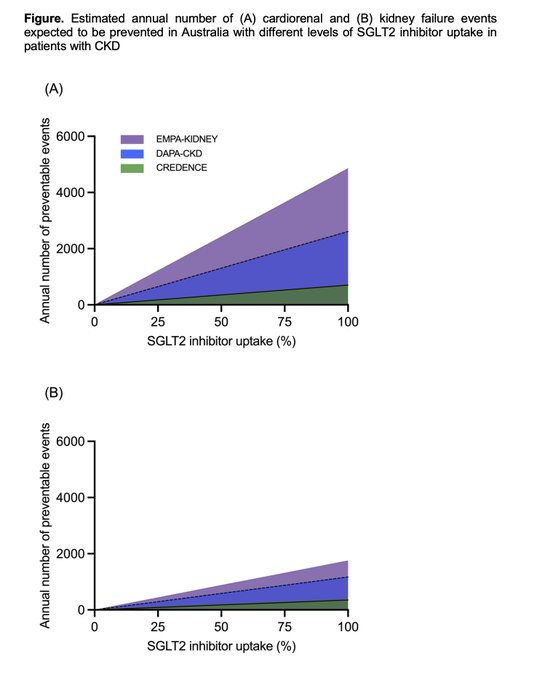
Improved uptake of SGLT2i in people with CKD has the potential to substantially reduce the incidence of kidney failure in Australia
Implementation now critical to realising these population level benefits
Our new paper
#openaccess
in
@LancetRH_WPac
2
32
87
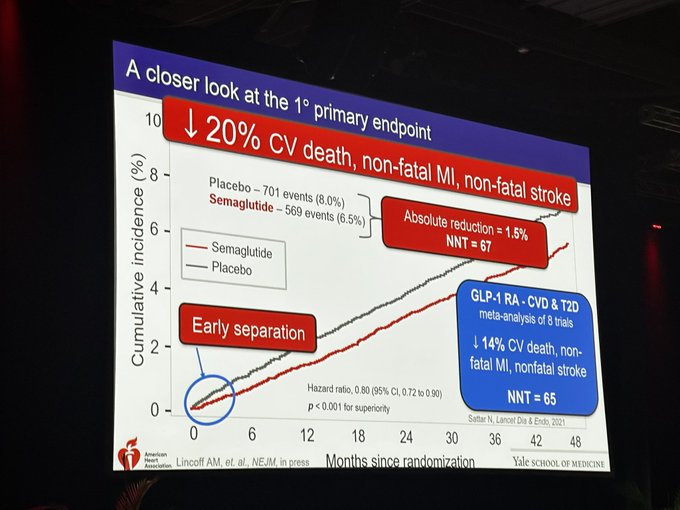
Early effect of semaglutide on the primary outcome occurred early, before the 65 week plateau in weight loss, raising the questions - what is the mechanism of CV benefit, and how much benefit is mediated by weight loss?
#AHA23
3
26
86
Our new paper in
@DiabetesCareADA
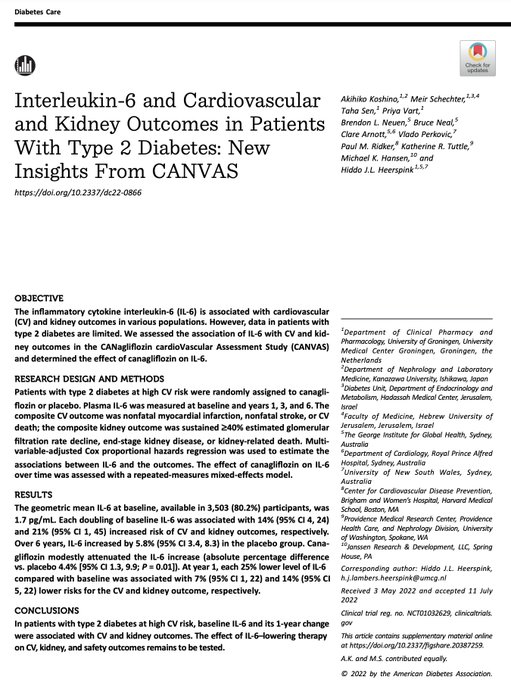
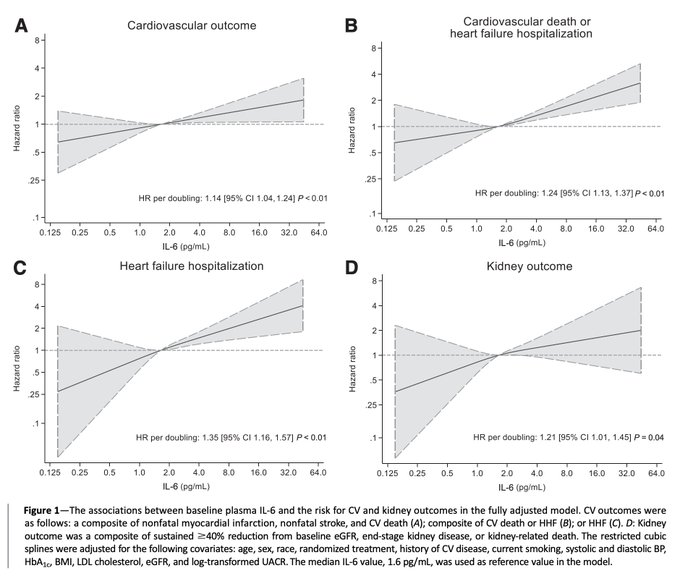
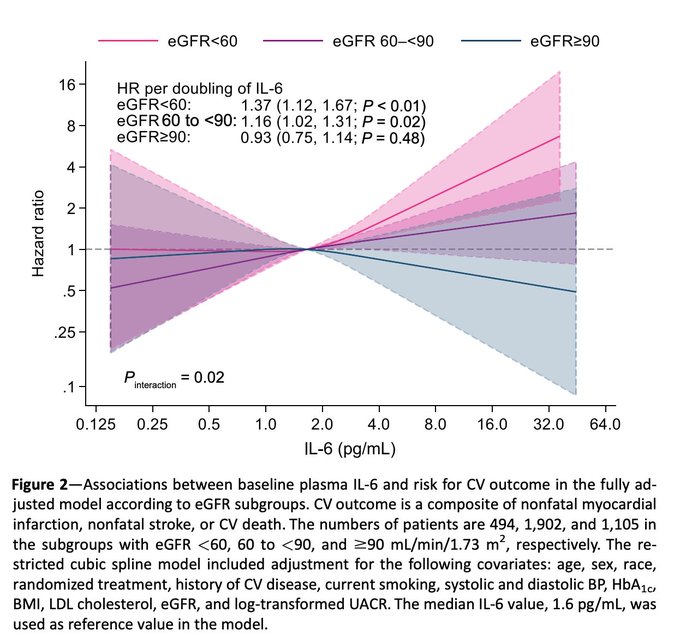
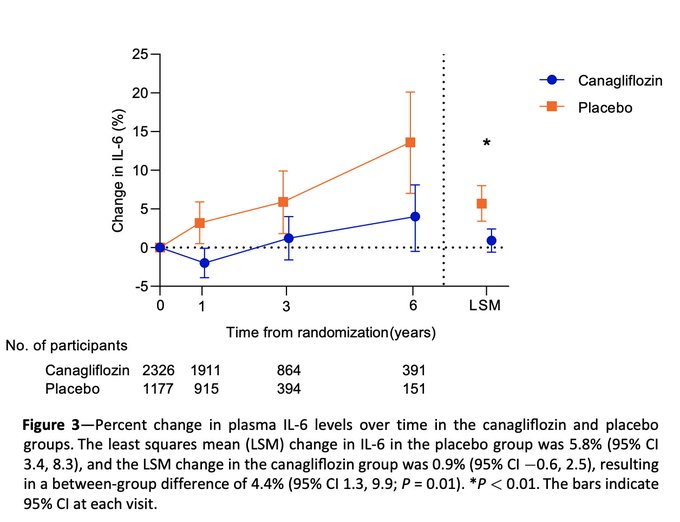
demonstrating that higher levels of interleukin-6 are independently associated with increased risk of cardiovascular disease & CKD progression, and that SGLT2 inhibition reduces IL-6 over time:
1
23
82
One ancillary benefit of SGLT2i is that pooling CREDENCE and DAPA-CKD there was a ~15% reduction in risk of RASi discontinuation (not yet published), so combination might enable better use of RASi (less hyperK, hospitalization, GFR decline?)
#nephJC
1
30
81
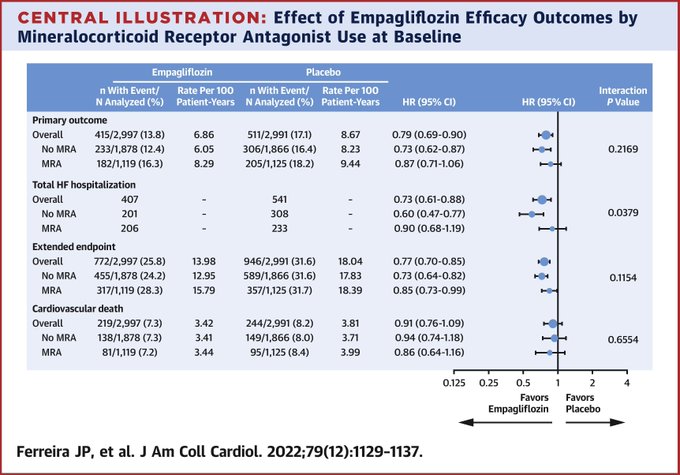
In people with heart failure with preserved ejection fraction, empagliflozin reduces HF hospitalization & risk of hyperkalemia, irrespective of MRA use, with numerically less MRA discontinuation
Accumulating data that SGLT2i enables optimal MRA use
3
35
82
Our CKD-EPI CT analysis of 66 trials (including SGLT2i, GLP1RA, nsMRA) showed that effect on total slope at 3 yrs strongly predicts effect on kidney failure. In contrast, chronic slope only moderately associated with kidney failure
In
@NatureMedicine
:

1
29
80
Very pleased that our paper on the effects of canagliflozin
on cardio-renal outcomes across different levels of albuminuria has been selected for "Best of
@CJASN
/
@JASN_News
at
#KidneyWk
2019
Join the Editors at this great session: 2-4pm Thursday
3
15
79
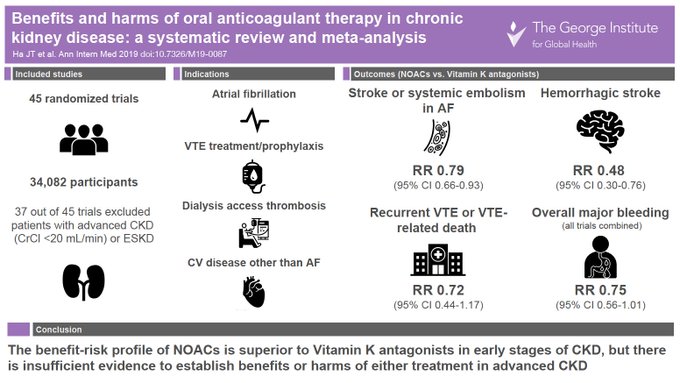
Our new systematic review & meta-analysis of the benefits & harms of anticoagulation in CKD, led by Jeff Ha &
@Badves
, now online in
@AnnalsofIM
Comprehensive data on a range of indications including AF, VTE treatment/prophylaxis & more
1
40
79
It is worth reiterating that SGLT2 inhibition can and should be continued until dialysis, as was done in CREDENCE and DAPA-CKD
#ADA2021

@mvaduganathan
@JavedButler1
@lamcardio
@brendonneuen
@DavidCWheeler2
@kaulcsmc
@AmDiabetesAssn
@drpatrickholmes
@AliceYYCheng
@ArodaMd
@drkevinfernando
@paomorejon
@fikkumamoto
@GoggleDocs
@pabeda1
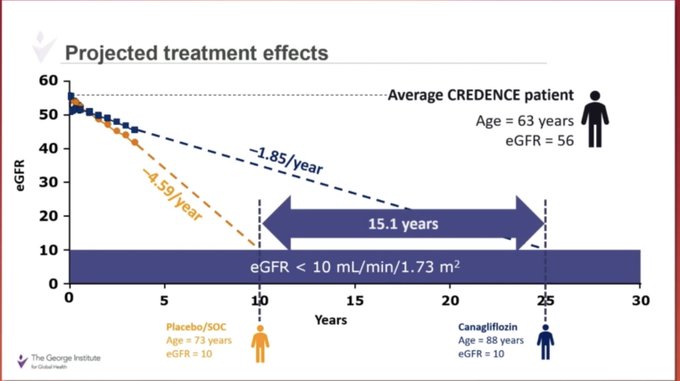
Nice data from CREDENCE
@brendonneuen
- Canagliflozin resulted in potential 15 years dialysis free compared to placebo 👍🏽
#ADA2021
@BritRenalSoc
@drpatrickholmes
3
22
55
0
35
78
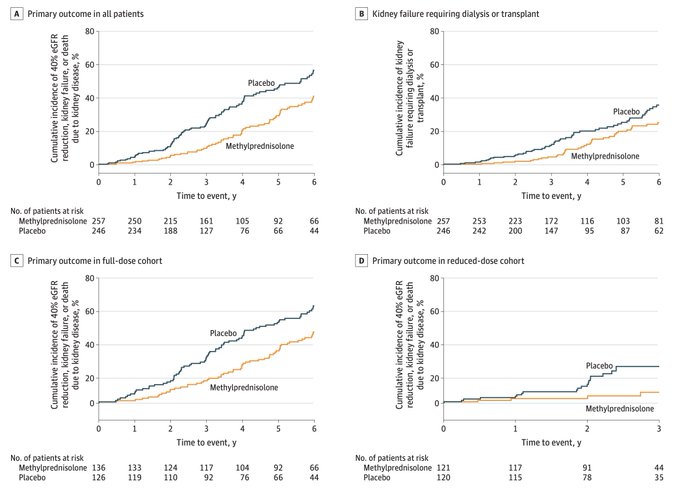
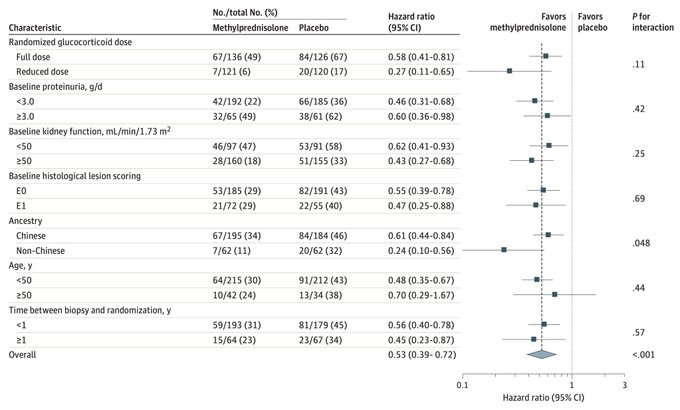
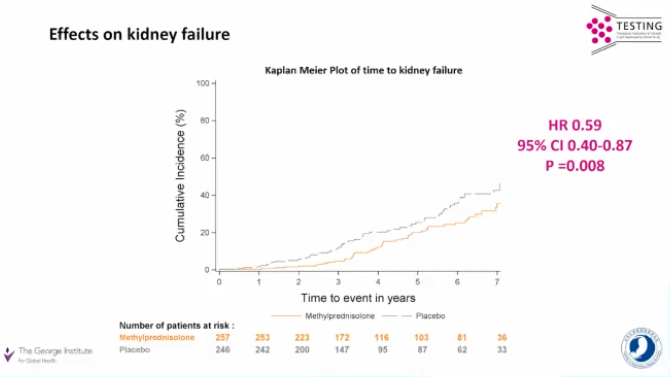
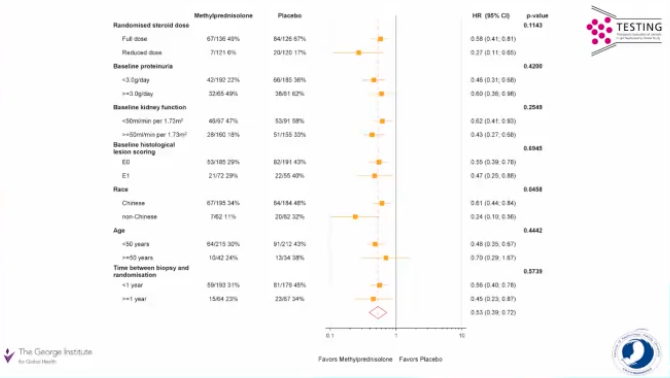
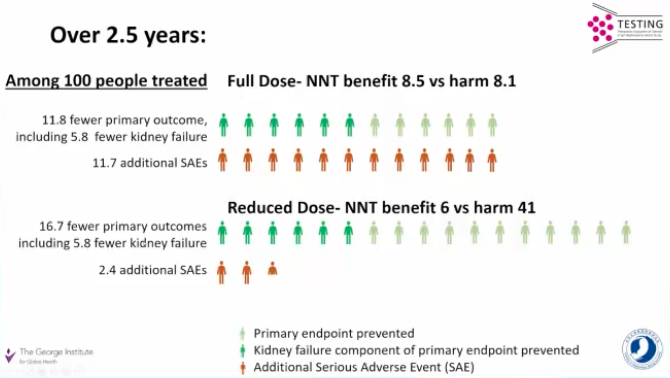
In the largest ever IgA trial (mean eGFR 61 & proteinuria 2.46g/day), corticosteroids almost halved the risk of kidney failure with similar effects in reduced vs. full dose, with adverse effects (i.e. infections) primarily observed in the full dose cohort
0
33
77
.
@mvaduganathan
& I recently summarised the fluid retention issue with ERAs as well as discussed ongoing trials of ERAs in CKD (including several IgAN/FSGS trials that have met proteinuria based endpoints, with ongoing evaluation of slope)
#nephjc

2
33
75
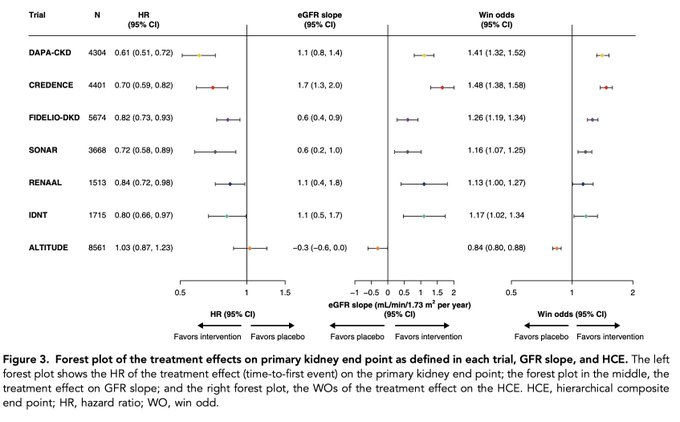
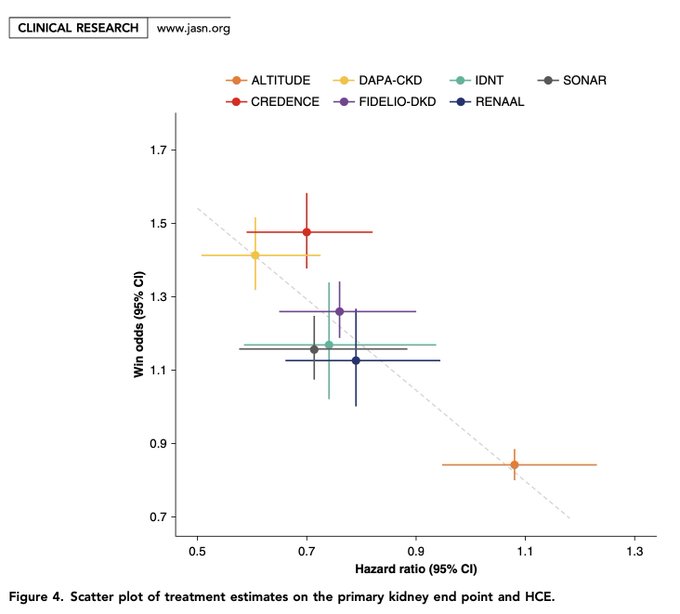
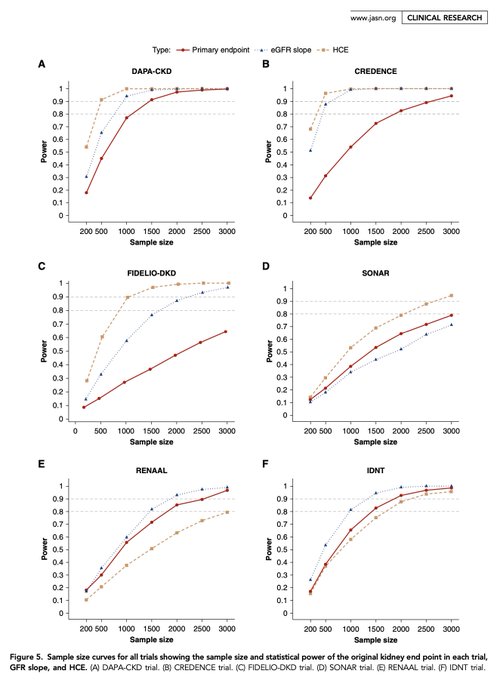
This is a very important paper for the nephrology clinical trials community - hierarchical composite endpoints are increasingly used in cardiovascular trials - here applied & modified for 7 landmark CKD progression trials
Open access in
@JASN_News
:
0
24
75
As
@hswapnil
points out, our task at implementation is going to become even more critical after FLOW
We need to reimagine, develop & refine a new framework that addresses urgency of optimising GDMT in ppl at high cardio-renal risk
Full text in
@CircAHA


We have excellent therapies available now - they have robust data from multiple RCTs, easier to implement than diets
Concept via
@brendonneuen
, also feat
@Gila_NephMad
the
#Nephmadness
winner
and we will soon have data on GLP1RAs in 5 weeks at the
#ERA24
#ISNWCN

1
10
27
2
19
73
New
#SGLT2
data presented today at
#EASD2019
- relative & absolute effects of
#canagliflozin
on kidney and cardiovascular outcomes across different levels of albuminuria
Now published online at
@JASN_News
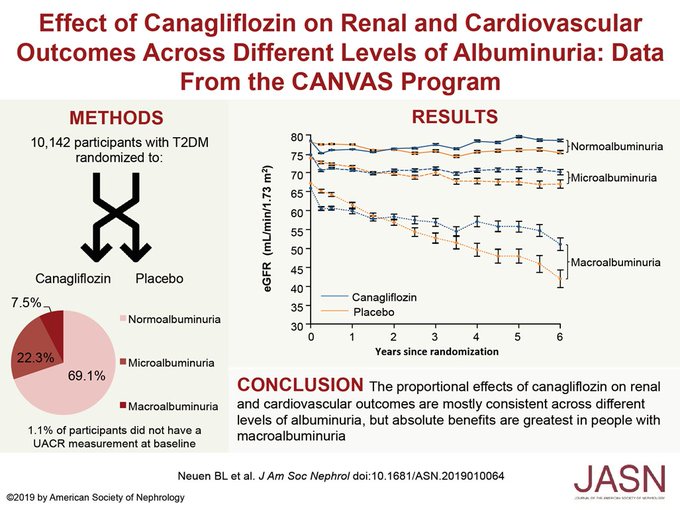
2
43
72
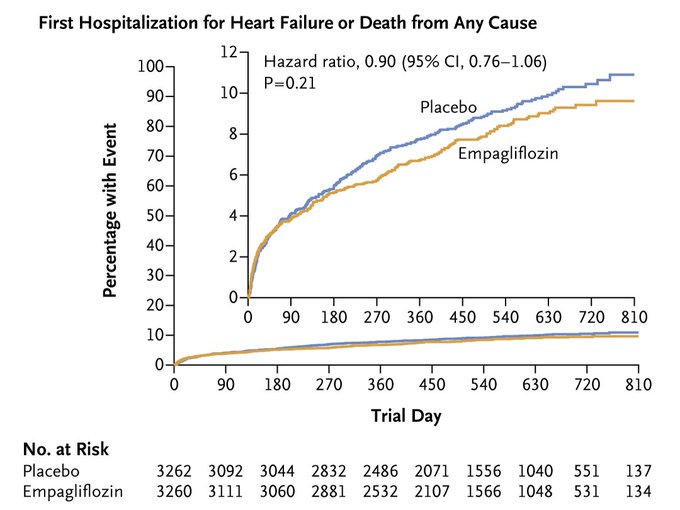
An incredible breakthrough & great news for our patients - the first ever treatment proven to reduce hospitalized heart failure or CV death in people with heart failure with preserved ejection fraction
Results being presented next month at
#ESC2021

5
21
71
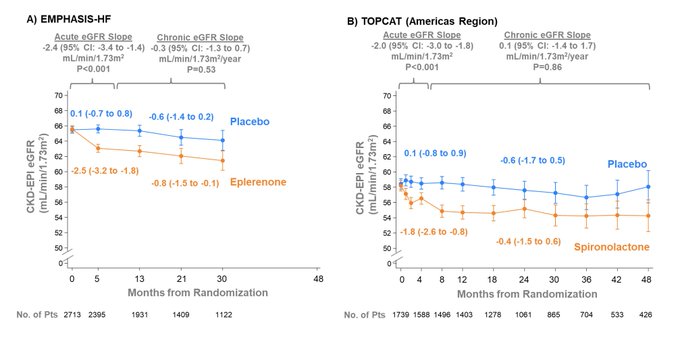
What are the effects of steroidal MRAs (spironolactone & eplerenone) on kidney function in heart failure? After an initial acute decline in GFR, chronic GFR slope is *not* modified by steroidal MRAs
Important work led by
@mvaduganathan
&
#JoaoFerreira
:
1
21
70
Delighted & honoured that our paper on the benefits of canagliflozin across
@goKDIGO
risk categories has received a 2021
@AJKDonline
Editors’ Choice Award for outstanding original investigation
Many thanks to all the editors for this recognition
1
7
71
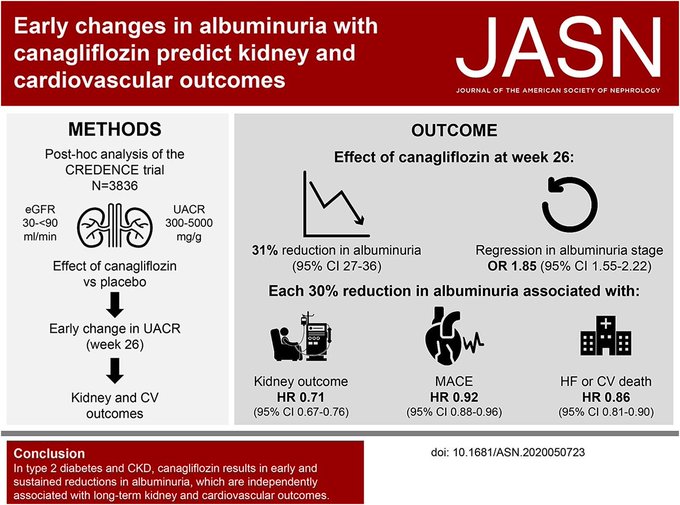
Our most detailed analysis yet of the albuminuria lowering effects of canagliflozin in the CREDENCE trial now published in
@JASN_News
, led by superstar
@georgeinstitute
Visiting Fellow Dr Megumi Oshima
A brief tweetorial on our key findings:
2
26
69
Chronic Kidney Disease Progression in Heart Failure: What We Know, Don’t Know, and Where to Next?
Our thoughts on GFR slope & assessment of kidney outcomes in heart failure trials, with
@HeerspinkHiddo
&
@LAInker
in
@JACCJournals
0
21
69
I'm delighted to be an investigator on RENAL LIFECYCLE, the largest SGLT2 inhibitor trial in ***dialysis and kidney transplant patients***
A global, collaborative, investigator initiated trial sponsored by
@univgroningen
@ArnottClare
@Badves
@rebeccakozor
@VladoPerkovic
Congratulations to Prof Craig Anderson and
@Badves
,
@ArnottClare
for receiving
#MRFF
grants totalling in $4.4 million for their respective research on
#stroke
and chronic
#KidneyDisease
!
Know more:

3
6
32
3
5
68
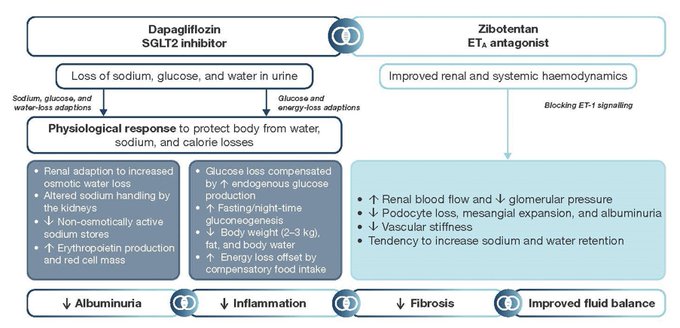
Could combination treatment with SGLT2i & endothelin receptor antagonists further reduce risk of kidney failure in people with chronic kidney disease?
Design and rationale of the phase 2B ZENITH-CKD trial
1
22
67
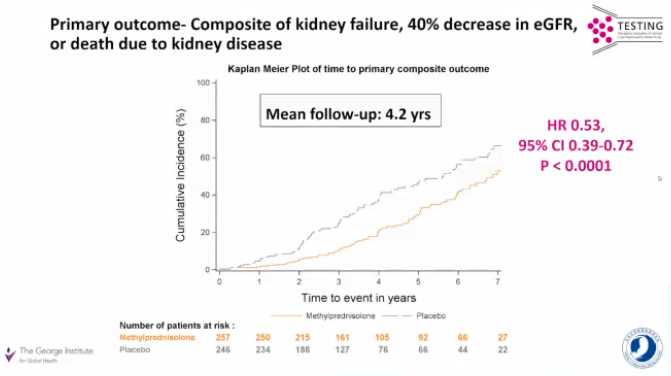
Remarkable results from TESTING - look at the number of events! 40% reduction in risk of kidney failure with corticosteroids - with consistent benefit regardless of endocapillary proliferation, and other subgroups including race
#KidneyWk
5
18
65
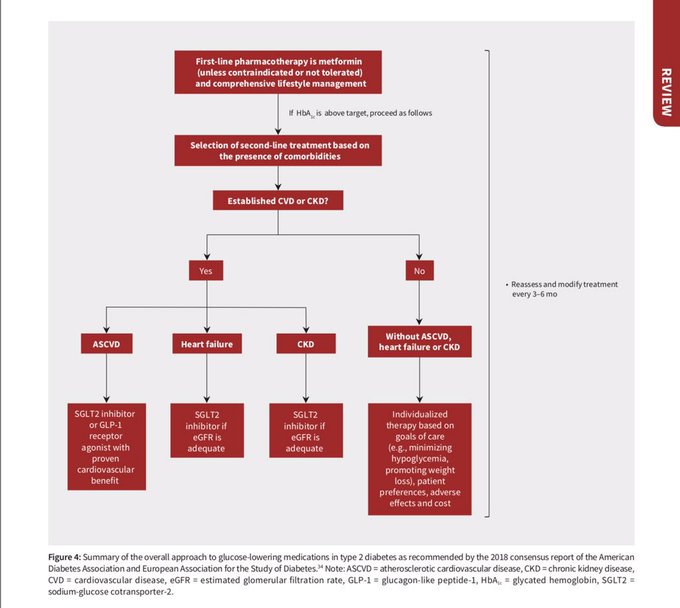
Treatment recommendations for diabetes are changing more quickly than ever before. Find out more in our new review of SGLT2 inhibitors & diabetes guidelines, with contributions from David Cherney,
@jardine_meg
&
@VladoPerkovic
Free this week in
@CMAJ
:
0
29
66
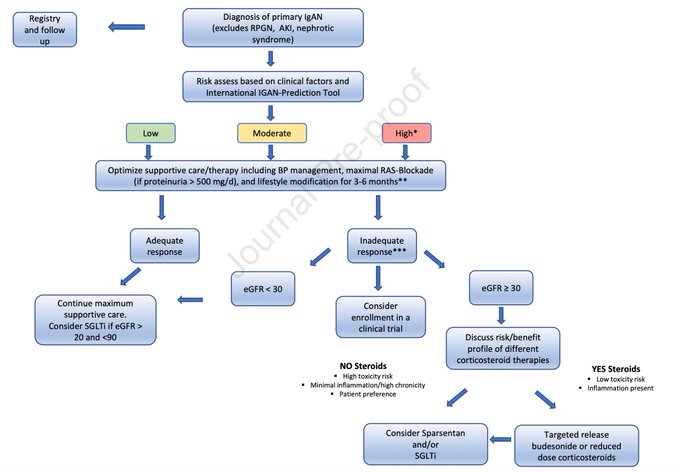
There are prob 2x as many clinical events in IgAN popn in the SGLT2i trials than Nefecon & PROTECT combined, with a very clear effect - so I'm a bit surprised SGLT2i isn't higher up as part of optimal supportive care, which is certainly my practice in IgA & that of my colleagues

Review by
@dawn_caster
and Richard A. Lafayette:
The Treatment of Primary IgA Nephropathy: Change, Change, Change
1
72
177
3
22
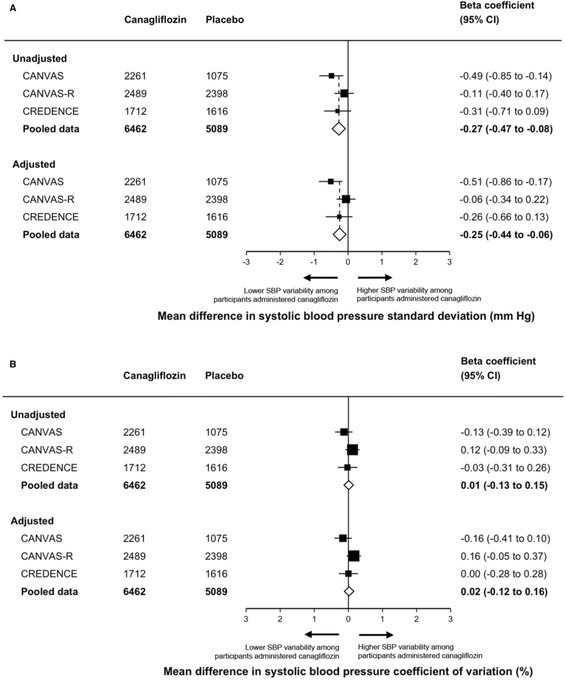
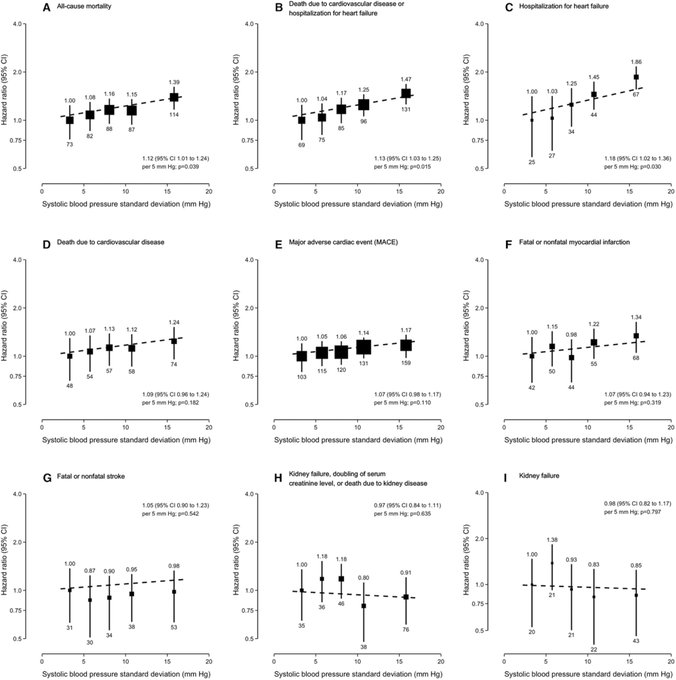
65
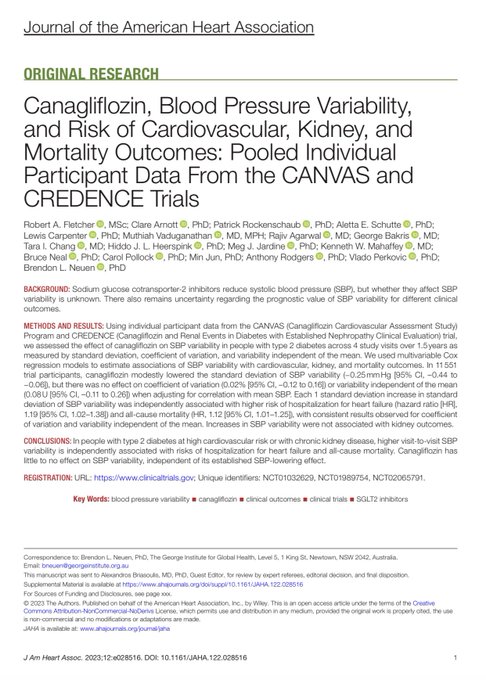
The largest & most comprehensive analysis of the association between SGLT2i, blood pressure variability & cardiorenal outcomes
While SGLT2i reduce BP, they have little to no effect on BP variability
New
#openaccess
in
@JAHA_AHA
led by
@Fletcher_RA
2
25
64
Join me
@hvanspall
@FaiezZANNAD
@kaulcsmc
&
@mvaduganathan
at
#AHA22
Nov 4 2- 3PM for "Heart & Kidney Outcomes Trials: A Deep Dive into Trial Design"
As we discuss:
- eGFR slope in CKD trials
- Renal outcomes in HF trials
- Novel cardiorenal endpoints
- Regulatory perspectives
6
24
64
Reading the EMPA-KIDNEY editorial in NEJM this week -
A case of where
@FreelyFiltered
gets it right -
@NEJM
suggests the benefit of SGLT2i is modified by RASi (it isn’t in EMPA-KIDNEY, or when totality of data examined)
Check out the podcast to find out why
@hswapnil


Listen to this great question by
@sophia_kidney
and then see how
@hswapnil
confabulates his way through it followed by
@brendonneuen
answering like a boss.
@FreelyFiltered
#EMPAkidney
0
2
10
3
19
63
Fascinating DAPA-CKD data at
#ERAEDTA21
- despite consistent protection against kidney failure with DAPA, albuminuria lower is attenuated in non-diabetic CKD, suggesting that mechanism unrelated to albuminuria lowering are important in these patients

3
21
64
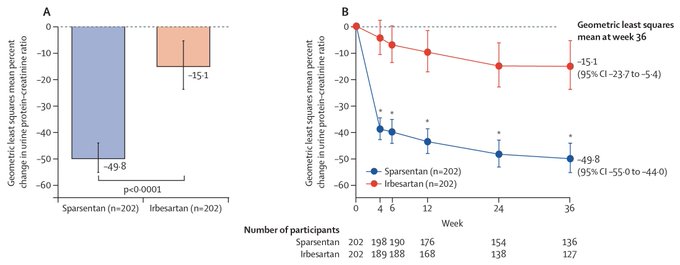
Sparsentan in 404 patients w/IgA
▪️2/3 white
▪️Proteinuria 1.8g/day
▪️41%⬇️ in uPCR at week 36
▪️OR 3.1 for complete remission (95% CI 1.6–5.8; p=0·0005)
▪️40%⬇️ in GFR/ESKD/death: 7 (3%) sparsentan, 13 (6%) irbesartan
More oedema, but no HF
#ISNWCN
3
26
62
What a treat to have Professor
@DrDeidraCrews
, President-Elect of
@ASNKidney
, delivering this week’s Cardiovascular Grand Rounds at
@BrighamWomens
.
A tour de force through her work on health disparities in CKD & how we can address inequities to improve outcomes for all
2
9
63
Dedicated 75-min
@ERAkidney
late-breaking session on the FLOW trial on May 24 featuring:
- Baseline data
@RpratleyMD
- Key findings
@VladoPerkovic
- Safety data
#JohannesMann
- Summary & clinical implications
@KatherineTuttl8
- Independent commentary
@ChristophWanne4
#ERA24

President of ERA prof Wanner announced FLOW semaglutide in type 2 DM with CKD will be presented in Stockholm at ERA on May 24

0
26
74
3
23
63
The accompanying slides for our Lancet D&E meta-analysis () on SGLT2 inhibition & major kidney outcomes can be downloaded here:
#ERAEDTA20

2
31
63
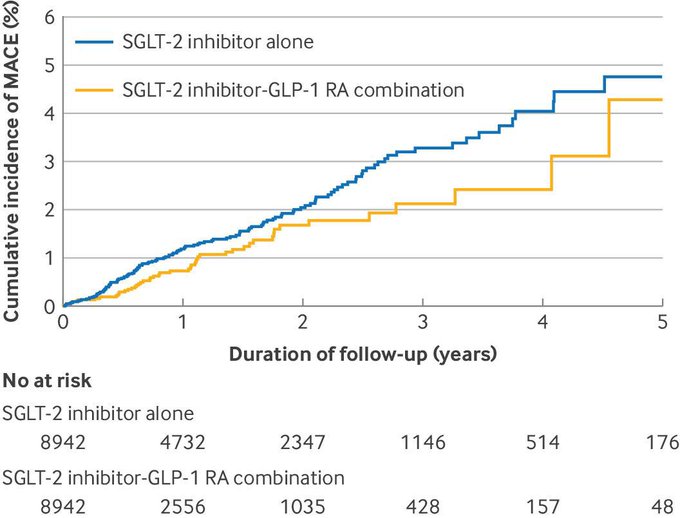
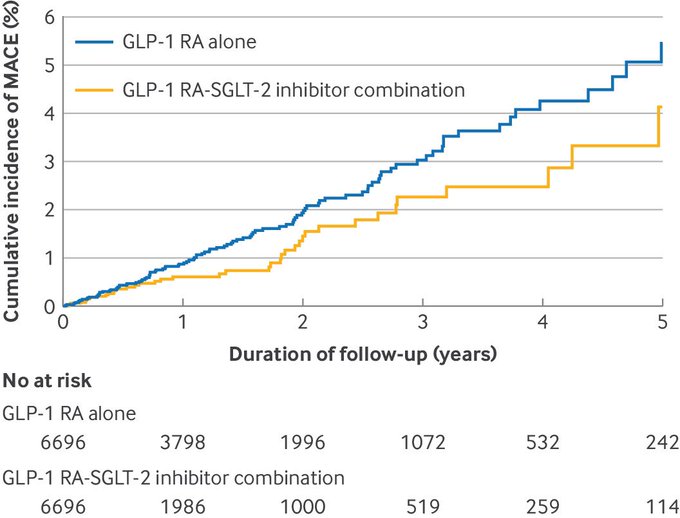
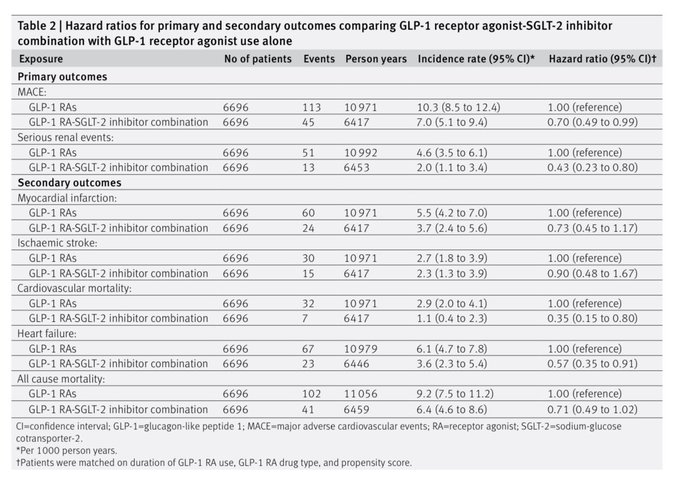
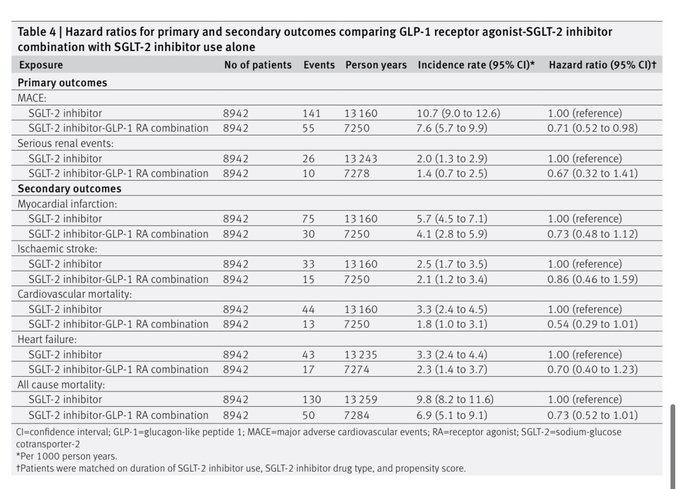
Routinely collected primary care data from UK:
Combination SGLT2i and GLP1-RA associated with reduction in risk of major cardiovascular events and serious renal events compared to either alone
From
@profLAzoulay
& colleagues in
@bmj_latest
1
22
63
Really honoured to receive the
@UNSWMedicine
Faculty Award for Outstanding Contribution to Research by a doctoral student - sorry that I couldnt be there!
Feel very lucky to work with so many great people at
@georgeinstitute
@Oxford_NDPH
@JASN_News
& beyond

Recognition of some of our best
@UNSWMedicine
2019 award presentations...so proud of their super achievements. How great is the diversity in this group.
0
2
17
12
3
60
**New 🐨🇦🇺 data**
SGLT2i use in diabetes & CKD in 2021: 14.4%
SGLT2i use in CKD (EMPA-KIDNEY eligible) 4.1%
Improved uptake of SGLT2i in CKD has the potential to prevent large numbers of ppl reaching kidney failure in Australia
Our preprint now online:
2
15
59
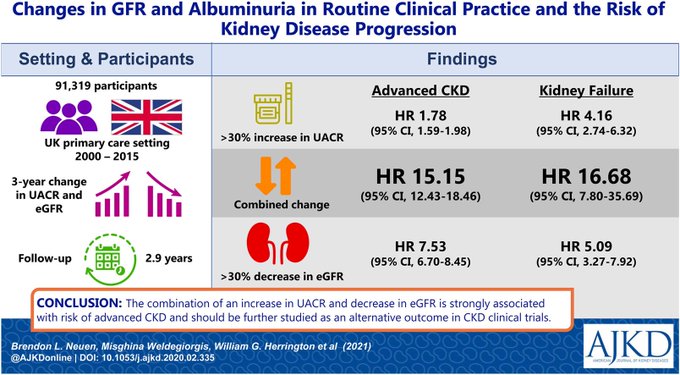
Our new
@AJKDonline
paper:
Evaluating combined changes in eGFR & albuminuria as an alternative endpoint for kidney failure in CKD trials
@georgeinstitute
/
@Oxford_NDPH
collaboration with my friend (and EMPA-KIDNEY PI)
@willkidney
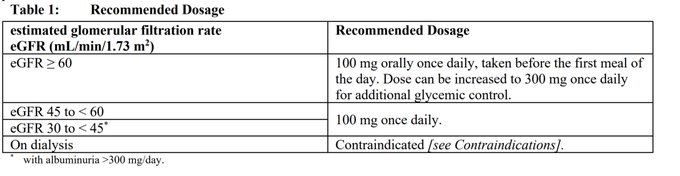
1
21
60

Major change: canagliflozin now approved for use with starting eGFR 30-45 ml/min AND can be continued when eGFR falls below 30 ml/min as was done in CREDENCE

0
25
58
Nice surprise to receive a copy of the
@JCardFail
focus issue on cardio-renal-metabolic medicine - thanks so much
@robmentz
&
@dranulala
!!
With great contributions from
@KaitlinMayne
@willkidney
@drpaddymark
@JavedButler1
@AndrewJSauer
@RyanTedfordMD
@ErinMichos
& many others

0
14
57
Are you analysing GFR slope in a study?
See our new SMART-C GitHub page (by
@Fletcher_RA
) with reproducible R code, synthetic data & explanation on how to calculate acute, chronic & total slope like in the CREDENCE and DAPA-CKD trials
More coming soon:

2
16
58
***Final
@ERAKidney
late-breaking abstracts announced***
Shortly after the FLOW results
Join us for the presentation of the SGLT2i Trialists Consortium (SMART-C) pooled data on the effects of SGLT2i on cardio, kidney & safety outcomes, with & without GLP-1RA
#kidneyGDMT
#ERA24
0
4
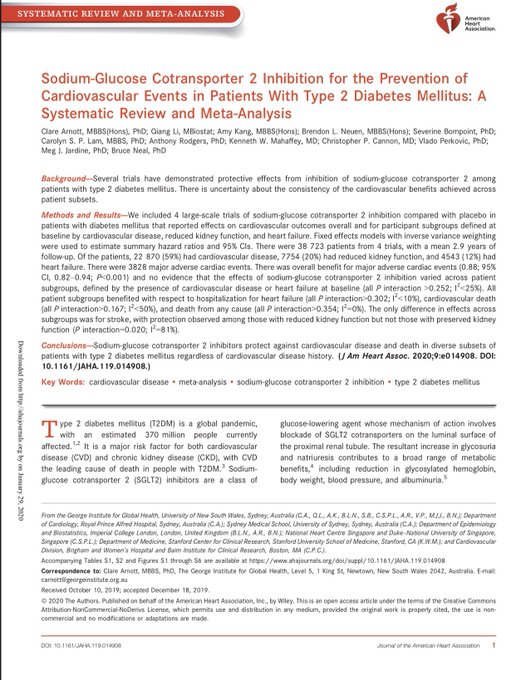
57
Our updated
#openaccess
meta-analysis of
#SGLT2
inhibitors & cardiovascular outcomes, including CREDENCE, led by
@ArnottClare
Now in
@JAHA_AHA
:
Growing evidence that these drugs should be used in most patients with diabetes at high CV risk
@cpcannon
1
32
57
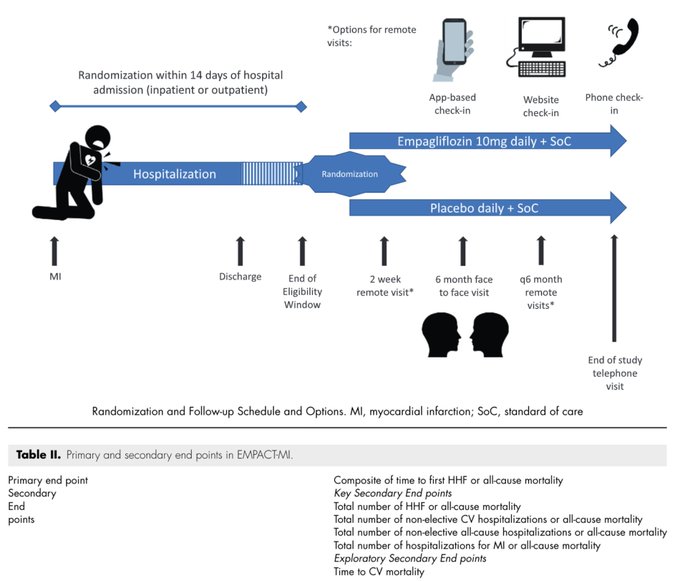
EMPACT-MI is a streamlined randomized trial assessing the efficacy and safety of empagliflozin in ~5000 people post myocardial infarction
Design and rationale paper from
@JLHarrington_MD
&
@JavedButler1
:
0
20
54
*Open access & free* Our Editorial in
@GlobalHealthBMJ
: it's time for global action on kidney disease
#NCDs
2
37
56
Great news - key renal points IMO:
- Lowest eGFR cutoff of any SGLT2 trial to date - down to 20ml/min
- 50% non-diabetic
- Improvement in chronic eGFR slope & renal endpoint (88 events, 40% decline in eGFR or ESKD)
<24 hours until DAPA-CKD results presented...!
#ESCCongress

🐧EMPEROR-REDUCED:
#Cardiovascular
& Kidney Outcomes with
#Empagliflozin
in Heart Failure
#SGLT2i
#VisualAbstract
@NEJM
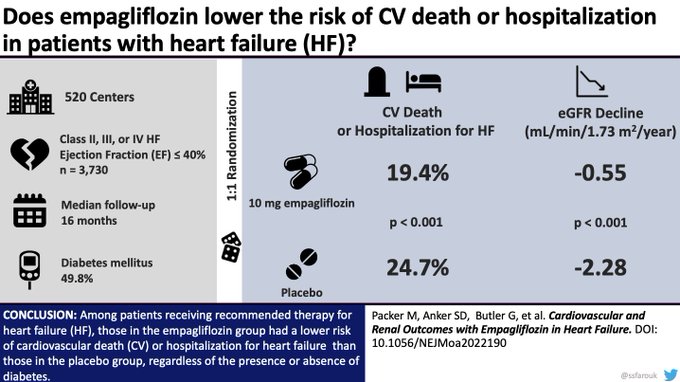
2
43
103
1
17
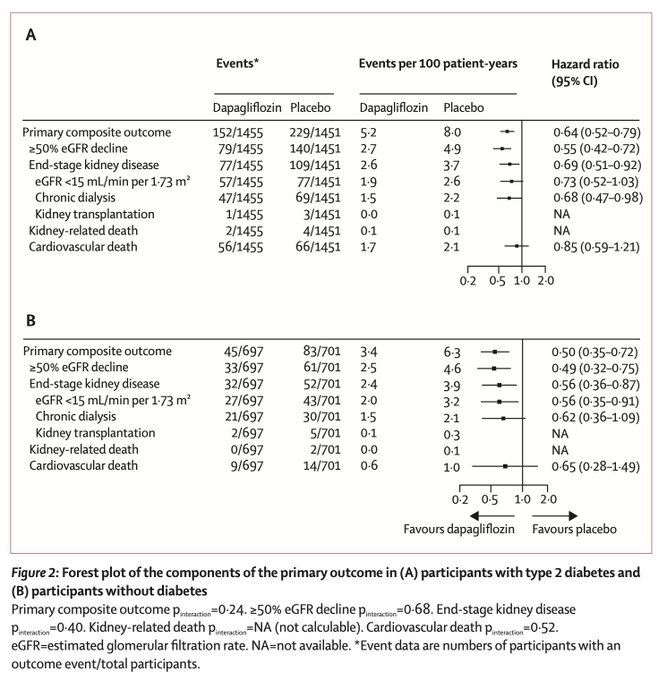
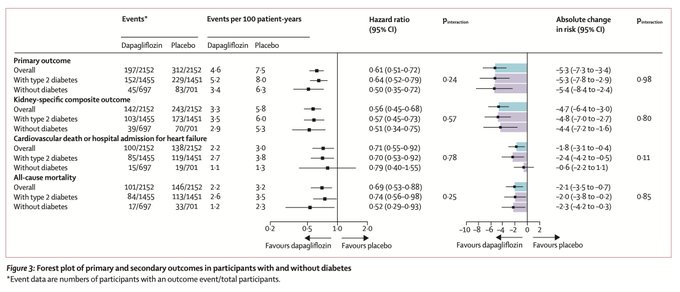
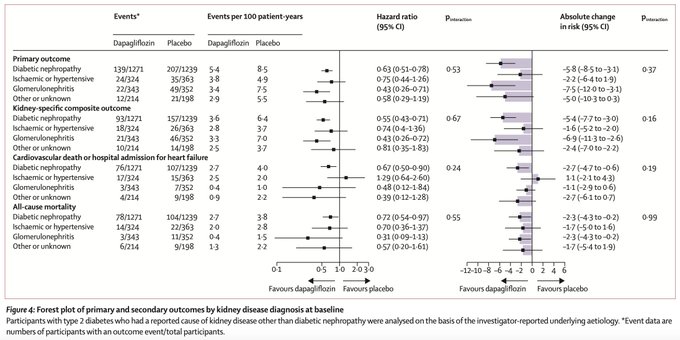
54
Effects of
#SGLT2
inhibition with dapaglflozin on kidney & cardiovascular outcomes by diabetes status and kidney disease aetiology: Results from DAPA-CKD
From
@DavidCWheeler2
&
@HeerspinkHiddo
et al. in
@TheLancetEndo
1
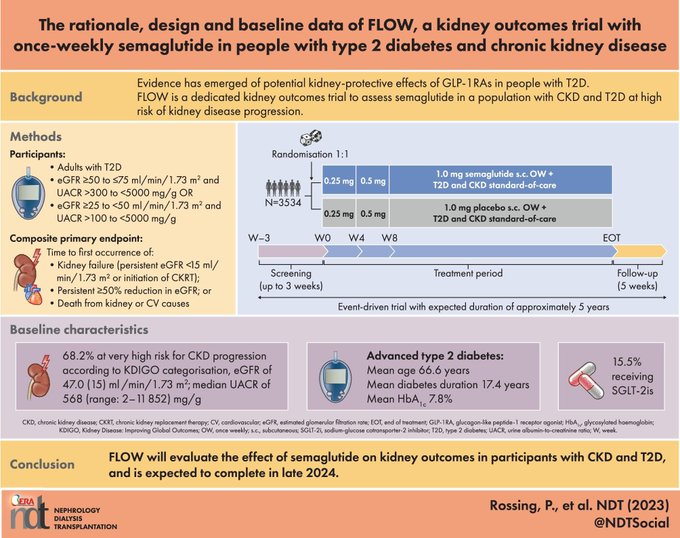
21
55
The role of semaglutide in reducing the risk of kidney failure in patients with diabetic kidney disease is being evaluated in the FLOW trial - expected completion in 2024
N=3534
Outcome=50% ⬇️ GFR, ESKD, CV/renal death
@VladoPerkovic
@RpratleyMD

#PRESS
Novo Nordisk product reduces the risk of major adverse cardiovascular events by 20% in adults with overweight or obesity in trial
10
58
208
3
23
53
In my view, the 23% & 33% ⬇️ in first & total hospitalised HF w/ SGLT2i post-MI is a welcome finding, consistent w/the totality of the evidence
Difficulty for any trial to demonstrate ⬇️ in all-cause mortality over median F/U 18 months given the standard-of-care in 2024
#ACC24

2
14
53
Finerenone, which slows progression of kidney disease and reduces CV events in people with diabetes and CKD, is being evaluated in 1500+ non-diabetic CKD individuals in the FIND-CKD trial

2
12
53
Want to know updates on the validity and use of GFR slope as an endpoint for CKD progression in clinical trials?
Join me at
#UKKW2023
on Tuesday where we discuss the latest developments - session chaired by
@jennifer_s_lees
&
@PaulCockwell
1
16
52
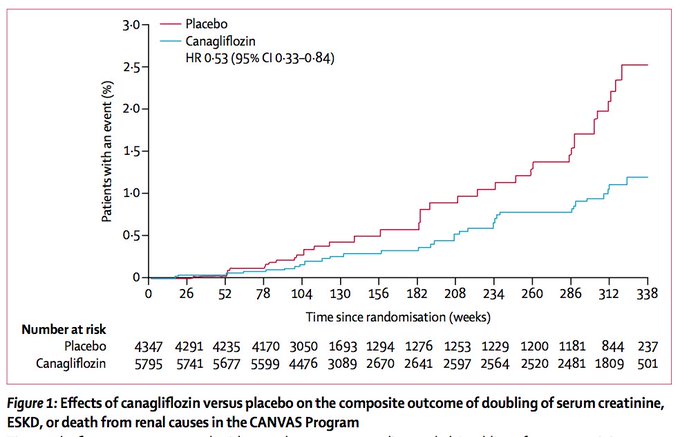
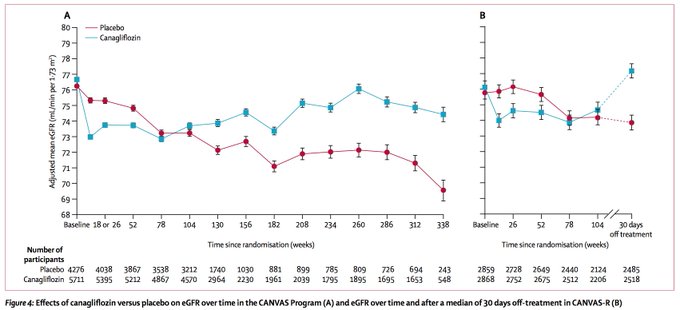
Big week in
#diabetes
&
#kidneydisease
: CANVAS renal outcomes, led by
@VladoPerkovic
, finally published in
@TheLancetEndo
!
#2018ADA
#ADA2018
4
39
49
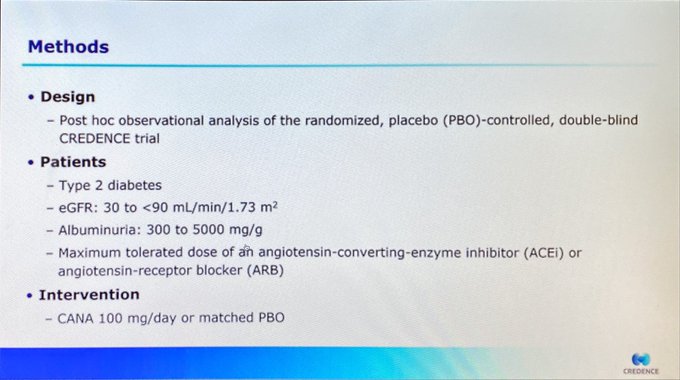
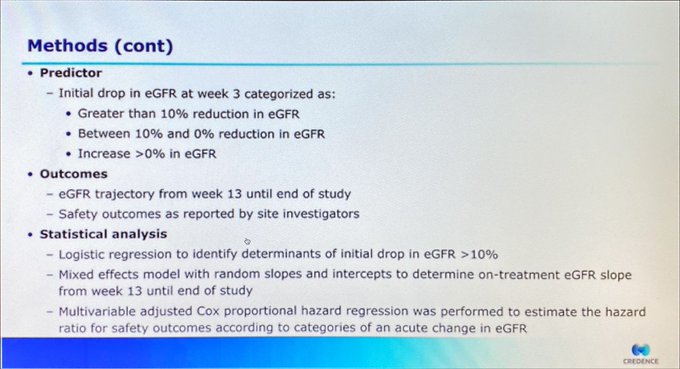
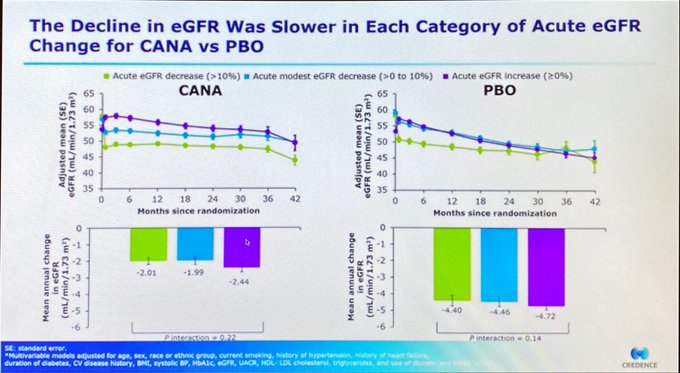
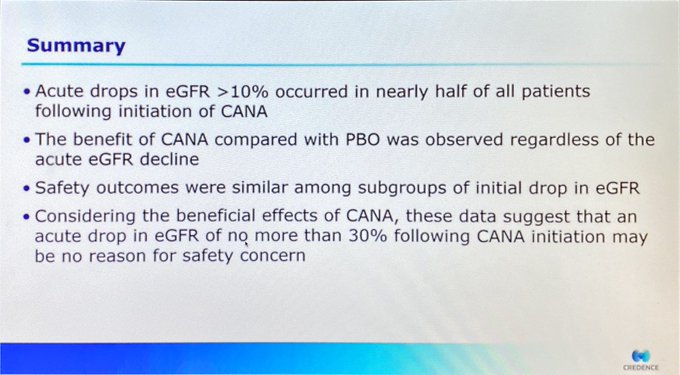
This is really important data from CREDENCE, similar to that presented by Bettina Kraus &
@ChristophWanne4
at
#eraedta20
Key message: do not stop SGLT2i due to an acute dip in eGFR at initiation. Kidney benefits are likely similar regardless of initial eGFR decline
#ADA2020

Reassuring data from the real outcome trial CREDENCE presented
#ADA2020
. Drop in eGFR of >10% not relegated to increase in adverse events (including renal events), unless the eGFR ⤵️ was >30%.
@kamleshkhunti
@drkevinfernando
@AmarPut
@AbdTahrani
1
29
60
0
20
50