
New insights from the CREDENCE trial on the blood pressure lowering effects of canagliflozin in type 2 diabetes and CKD now published in
@CircAHA
4
81
255
Replies
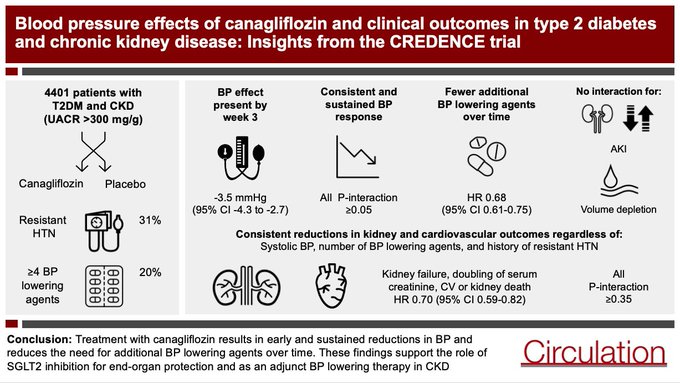
Of all the major SGLT2i trials, CREDENCE had perhaps the highest burden of hypertension, which gave us the unique opportunity to assess the BP effects of SGLT2 inhibition in CKD
Of 4401 patients:
-25% systolic BP>150 at baseline
-30% resistant HTN
-20% on 4+ BP lowering agents
1
0
4
In the overall trial population, canagliflozin lowered systolic BP by ~3.5mmHg at week 3, with a sustained treatment effect of a similar magnitude observed over the duration of the trial

1
0
2
We found that the BP lowering effect of canagliflozin at week 3 (column A) and over the duration of the trial (column B) was consistent regardless of:
- Baseline systolic BP
- Number of concomittant BP lowering agents
- History of apparent treatment resistant hypertension

2
0
2
Treatment with canagliflozin increased the probability of experiencing a >5mmHg reduction in blood pressure at week 3, with a similar likelihood of BP response regardless of number of BP lowering agents, history of resistant hypertension, baseline eGFR or UACR

1
0
2
Canagliflozin substantially reduced the need for additional BP drugs over time
Probably a reflection of both BP lowering effect of SGLT2i & benefit of preserving kidney function on BP as demonstrated by this beautiful MR paper by
@meg21212
et al

1
1
5
Canagliflozin reduced the risk of major kidney outcomes, including kidney failure alone, regardless of baseline BP, number of BP lowering agents, or history of resistant hypertension

2
2
3
We found that reductions in cardiovascular events were similarly consistent across BP defined subgroups with no interaction observed for key adverse events including AKI and volume depletion


1
0
1
To what extent do the blood pressure lowering effects of canagliflozin contribute to cardiorenal protection?
Our mediation analysis suggests that less than 10% of kidney and cardiovascular benefits are explained by blood pressure effects

1
1
3
These BP reductions, which are comparable with low dose HCT, indicate that SGLT2 inhibition can be considered as an adjunct blood pressure lowering therapy in people with diabetes & kidney disease, in addition to its kidney & cardiovascular protective effects
1
2
6
Finally what do these data tell us about mechanisms of BP lowering with SGLT2 inhibition in CKD?
For the most part, effects on BP have been attributed to natriuresis & osmotic diuresis, the premise of which is predicated on normal kidney function
1
0
1
Reductions in BP that are at least as large in people with CKD in the absence of significant glycosuria suggest that natriuresis is unlikely to be the sole mechanism for BP lowering in people with reduced GFR
1
0
3
A number of natriuretic independent mechanisms for BP lowering have been proposed, including a reduction in SNS activation -
Despite their effects on intravascular volume, SGLT2 inhibition does not alter heart rate (we looked in CREDENCE), supporting this hypothesis
1
0
2
There are some lines of experimental evidence supporting a link between reduced SNS activation and SGLT2 inhibition
1
0
0
And more recent data indicate that during standardised sodium intake SGLT2i lower BP without altering urinary sodium excretion
Again suggesting that factors other than natriuresis may contribute to BP lowering
0
0
0

@brendonneuen
@CircAHA
@georgeinstitute
@VladoPerkovic
@jardine_meg
@alta_schutte
@AgarwalRajivMD
@carinnahockham
@jlgorriz
@taraichang
@ArnottClare
@DCharytan
Nice work
1
0
3

@brendonneuen
@CircAHA
@georgeinstitute
@VladoPerkovic
@jardine_meg
@alta_schutte
@AgarwalRajivMD
@carinnahockham
@jlgorriz
@taraichang
@ArnottClare
@DCharytan
Earlier last week, I placed a patient, DM2 Insulin-Dependent w HFrEF < 45%, on Dapagliflozin. The pt subsequently developed a UTI (Proteus mirabilis) and almost Urosepsis. He was admitted to hospital for IV antibiotic therapy, and was eventually discharged. I will not place 1/
1
1
0

@brendonneuen
@CircAHA
@georgeinstitute
@VladoPerkovic
@jardine_meg
@alta_schutte
@AgarwalRajivMD
@carinnahockham
@jlgorriz
@taraichang
@ArnottClare
@DCharytan
“In people with T2DM and CKD, canagliflozin lowers systolic BP across all BP defined subgroups and reduces the need for additional BP lowering agents. These findings support use of cana for end-organ protection and as an adjunct BP lowering therapy

0
6
13