
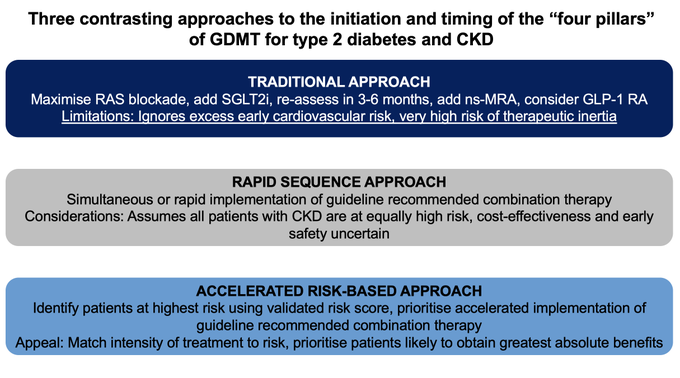
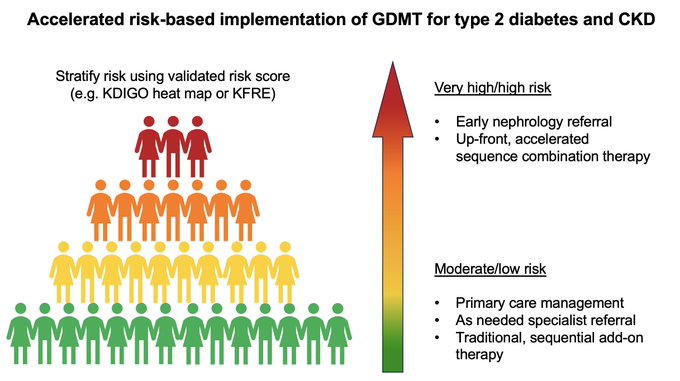
How can we prioritise accelerated therapeutic implementation of the "four pillars" of GDMT for diabetes & CKD?
-RASi
-SGLT2i
-ns-MRA
-GLP-1RA
@mvaduganathan
@KatherineTuttl8
& I outline what an "accelerated, risk-based approach" might look like
@CircAHA
2
35
101
Replies

@brendonneuen
@mvaduganathan
@KatherineTuttl8
@CircAHA
@georgeinstitute
@BrighamFellows
@george_clinical
Why would one need 3 to 6 months to fully onboard SGLT2I? 3-4 wks are needed to get a new baseline of egfr, then one moves to the nsMRA, which can be prescribed based in CV risk alone. If gfr >45 can start both at the same time. Glp1 can be dropped any time.
#pharmanuke

2
0
7
@ChristosArgyrop
@mvaduganathan
@KatherineTuttl8
@CircAHA
@georgeinstitute
@BrighamFellows
@george_clinical
Completely agree with you - but guidelines & consensus recommendations don't currently advocate such an approach. Instead they suggest monitoring UACR every 3-6 months! Which is not even happening. We need a new framework that prioritises accelerated GDMT uptake for high-risk pts
1
0
5

@brendonneuen
@mvaduganathan
@KatherineTuttl8
@CircAHA
@georgeinstitute
@BrighamFellows
@george_clinical
Could you please share the full text article?
0
0
0