
Rowan Harwood
@RowanHarwood
Followers
2,394
Following
2,990
Media
72
Statuses
38,776
Consultant/ professor of geriatric medicine. Ageing idealist, viola player, Anglo-catholic, pro-EU. Editor-in-chief Age & Ageing.
Joined May 2014
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
#JO1
• 338660 Tweets
#Mステ
• 294909 Tweets
#Mステ
• 294909 Tweets
Xavi
• 117183 Tweets
Scottie
• 56295 Tweets
デザフェス
• 37584 Tweets
Valhalla
• 35246 Tweets
CHASING THE SUN
• 34295 Tweets
平野紫耀
• 34265 Tweets
紫耀くん
• 26835 Tweets
#小清水透3D
• 24242 Tweets
Louisville
• 20683 Tweets
Isco
• 14345 Tweets
トップバッター
• 13263 Tweets
しーちゃん
• 12735 Tweets
Go City Go
• 12356 Tweets
Last Seen Profiles





















@guardian
What sort of language is 'imposed'? DNACPR is a clinical decidion balancing likely effectiveness, burdens, and autonomy or best interests, not a punishment.
96
13
245
This article is complete nonsense. Half of it factually incorrect. Who does he think does all the work?. 'Costs soared under Tony Blair and Gordon Brown. Nothing seemed to improve'. The NHS ranked world leading in 2010.

30
57
223
@dsmiffy55
@RichardJMurphy
@BBCRadio4
Hospitals are open at weekends. Scans get done all weekend. Friday's go on as late as the rest of the week. When I work a weekend there are no days off in lieu, its 12 days on the bounce. The guy on
@BBCr4today
was talking rubbish
7
33
200
@NHSEngland
@NHSEmployers
@gmcuk
@RCPhysicians
Behind it all is a government hostile to the profession and the NHS.
@RCPhysicians
needs to be a thought leader and critical friend. Instead it has been played to collude with the hostile ideology. 5/n
1
25
188
@NHSEngland
@NHSEmployers
@gmcuk
@RCPhysicians
The idea that
@gmcuk
will leave scope to employers is for the fairies. They can't be trusted.
@bma
scope document is clear and precise. I fear that
@RCPhysicians
scope will be vague and general. The reason we need tight scope is that other stakeholders can't be trusted 5/n
2
27
150
'we want to represent everybody' ... But not the 48%. Bonkers. Pull yourself together
#Labour

Bad move
@tom_watson
to attack Farron when 73% in
@LabourList
poll think Labour should retain option to block Art50.
67
335
391
6
75
115
First message from
#RCPEGM
was the dire state of post-grad medical training in the UK. This has happened on our watch and needs sorting urgently. If we need a model, messages coming back from émigrés to Australia sound encouraging. Plus unjust T's&C's 3/n
2
9
110
We needs to address retention. Working conditions, work satisfaction, career progression, work life balance, salary

7
28
107
How long are Covid patients infectious? We are told 7d. 'Viral shedding' in Wuhan was max 37d. I have heard of a patient PCR+ for 54d. Italy wants - ve PCR before considering non infectious.
@trishgreenhalgh
@mancunianmedic
17
31
93
@NHSEngland
@NHSEmployers
@gmcuk
@RCPhysicians
@RCPhysicians
makes a big play of being 'inside the tent'. Big mistake. As with MTAS and Lansley 2012. The positive pickings are meagre ('more medical students ' and even that now postponed) and no progress on unblocking PG training bottlenecks.
#RCPEGM
@NHSEngland
@RCPhysicians
2
12
92
Please be aware that these drugs make some difference, but very small, at least over 2 years, with some risk, and substantial investigation and treatment burden. They are not a cure. I am not sure that NICE approval is justified, VFM is dubious

11
21
83
Second message is that so called leaders have totally lost trust.
@NHSEngland
@NHSEmployers
@gmcuk
@RCPhysicians
. The system will work better if they tried to regain it 4/n
1
9
80
In 35 years as a hospital doctor it has never struck me before to discharge patients where possible. Funny that. What do they think we do?
1
11
76
Council debates are vigorous, but secret. Messages put out in the name of Council are in the gift of the senior officers, and are not necessarily the agreed view of Council. The views of Council members are only 'advisory'. Surprised me too, that one 2/n
7
3
75
@ChrisHopsonNHS
This is incoherent spin! And hypocritical. If NHSE appreciates GP so much why the hostility and reluctance to support and pay for it? ARRS is a mess, especially putting undertrained PAs in general practice with inadequate supervision. Pharmacy first is expensive tinkering
0
11
69
Staff are still seeing covid + patients in surgical masks. Obviously inadequate from the start. On my ward most nurses and junior doctors have had covid. And half the consultants. Nosocomial spread is common. PHE and IPC credibility is gone.

"Trusts denied they had issued warnings to staff who had raised concerns about PPE supplies..." 😲
This is gaslighting on an industrial scale. It denies the experience of every frontline NHS worker. 😭
Please read & RT ⬇️
by
@mancunianmedic
6
155
243
5
23
64
What do they think we do every day of the year?

3
10
58
@UKGastroDr
Perhaps we should call them clinical associates, regulate via HCPC and then there would be less confusion. Medical professionals is nonsense and designed to obfuscate. GMC and NHSE seem intent on blurring the distinction. Meanwhile 'physicians' need to reclaim the word.
2
9
51
@Chris08505199
@juniordrblog
The NHS is under an obligation to provide translation. Mental capacity act 2005 and equality act 2010
1
6
45
The government needs to settle by making a credible offer. I have never seen junior doctors so demoralised, exploited and angry.
1
22
48
@DrAsifQasim
The recent FPA/RCP 'titles and introductions' document forbids comparison with medical grades. This practice has to stop. …
4
1
47
We must address retention. Dr's and other healthcare profs. T&Cs and especially working conditions which are very poor.

1
5
35
However. Death certification is fundamentally uncertain. The ONLY reliable measure of the impact of Covid-19 on mortality is the excess total mortality, judged against the last 5y average by month.
@mancunianmedic
#COVID19
3
12
33
Education alone is not enough. Need attitude and system change. Acute medical model is a problem.

For every additional 48 hours of active delirium mortality increases by 11%, ignorance is no longer acceptable
1
141
111
4
17
30
New developments in geriatric medicine. 'Admission as a precautionary measure'. Prolonging in patient stays for 'rest and observation'. How about hospital at home?
@darren_aw
4
4
31
The idea that
@gmcuk
will leave scope to employers is for the fairies. They can't be trusted.
@bma
scope document is clear and precise. I fear that
@RCPhysicians
scope will be vague and general. The reason we need tight scope is that other stakeholders can't be trusted 4/n
2
8
30
You won't lose weight by cycling unless you do Tour de France distances. You have to eat less. This repeats food industry inspired misinformation (thread) 1/
Doctors to prescribe bike rides to tackle UK obesity crisis

2
13
29
@spectator
If you want to keep driving you will have no choice but to get an electric car. We have to stop burning fossil fuel very soon. We are delighted with our Kia eniro
18
0
27
@mancunianmedic
The numbered list towards the end of the thread is entirely sensible. BUT:
- We were instructed to discharge to care homes ASAP, I think within 3h of a decision, by NHSE
-This was centrally funded
-we were told that if you had no cough or fever you were not infectious 1/n
3
8
28
@Age_and_Ageing
is 50. How much has changed? 1972 geriatricians were worrying about some of the same things as today. But the science and the writing has undoubtedly improved. And we now have blogs to show us the way
@CharSquires

0
12
28
The problem with workforce is not training or recruitment. It is retention. Working conditions are poor. Professional autonomy is absent. For all healthcare professions.

1
11
27
The Royal College of Physicians is holding elections for council. Canvassing is forbidden. I can say 1) there is an election 2) I am standing 3) election statements are on the website 4) FRCPs will receive an email on how to vote from 3 March
3
11
27
@mancunianmedic
-if hospitals are unpleasant and inappropriate places for frail older people that is because the NHS chooses to run them that way, using a narrow acute medical model
-there are many examples of person centred humane hospital wards, often in specialist older people's departments
2
6
27
@NHSEmployers
Increase pay, show you value staff, pay for courses and training, cut the bullying
1
3
26
Ti's is important and depressing (& scandalous). A thread /n
3
16
25
@ChrisCEOHopson
Retention retention retention. That means better working conditions, professional fulfilment, supportive management (not bullying, intimidation or 'grip'), adequate resourcing, less aggressive regulation
2
4
25
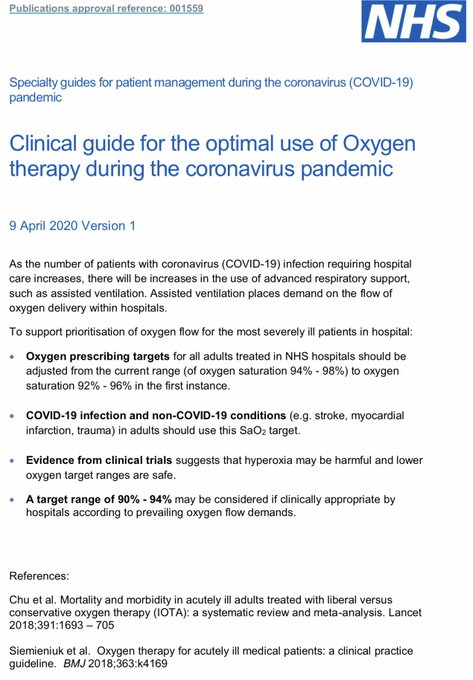
Why not adopt this always? At least for older people. So many are tied to a bed by nasal O2 cannulae for an SaO2 of 92%. It triggers NEWS2 diverting and distracting staff. Then we could get on with delivering person centred care, discussing priorities and making sensible plans

2
6
25
@RCPhysicians
makes a big play of being 'inside the tent'. Big mistake. As with MTAS and Lansley 2012. The positive pickings are meagre ('more medical students ' and even that now postponed) and no progress on unblocking PG training bottlenecks.
#RCPEGM
@NHSEngland
@RCPhysicians
1
4
25
Behind it all is a government hostile to the profession and the NHS.
@RCPhysicians
needs to be a thought leader and critical friend. Instead it has been played to be collude with the hostile ideology. 5/n
1
5
25
@guardian
If a patient has COVID-pneumonitis CPR rarely works, regardless of age or underlying conditions
39
1
23
@ChrisLeslieMP
@sarahwollaston
@Dr_PhilippaW
@joannaccherry
@thomasbrake
@coyleneil
@LSRPlaid
@Anna_Soubry
@ChukaUmunna
@heidiallen75
@MikeGapes
Too late. Time for
#RevokeA50
0
3
22
@AmandaPritchard
Please can you sort our capacity and resources. Let's start with double? Then you won't have to thank us for sorting out the mess
0
3
23
28% real terms pay reduction since 2010 for consultants is not helping. GP workloads unsustainable. Toxic over regulation problematic .
1
4
22
NHS fees to dentists don't even cover their costs. Hence it's collapse. GP gatekeeping is both good and efficient medicine. I have no idea what
@wesstreeting
is trying to achieve, but you can be sure that it won't work
0
2
23
Whether from a position of strength or weakness, geriatric medicine has work to do to drive up standards in health care for older people

0
6
23
@danielgoyal
@wesstreeting
To increase NHS staff we need to address retention. It's about pay, the dreadful working conditions and how professionals are treated
3
4
22
Blame individuals when the system is broken. I don't recognise this. I see an inadequate underresourced toxic environment. Toxic management. Fragmented discontinuous care. Consultants lacking confidence to make decisions. Toxic focus on discharge. Impersonal industrial processes

During 29y as
#NHS
Consultant I saw empathy in Doctors, Nurses, Admin staff being crushed by Target driven culture set by Governments. I saw abuse of staff eg no food during relentless 13hr night shifts. Don't mistreat staff then blame them for lack of empathy.
@jotalbotbowen

37
144
627
5
7
22
@timricketts_
@DrLindaDykes
Wear an FFP2-3 mask. On older people's wards it's an odd mix of usual business, waiting (contacts, vulnerable spouses, outbreaks in care homes) and end of life care. Families not visiting makes normal business harder and slower
0
2
21
@DuncanWeldon
@TheStephenRalph
Herd Immunity makes no sense - remember Spanish flu, aztecs and smallpox or plague. It is a vaccination concept. The UK
#COVID19
response may just have been incompetent
1
6
22
@wesstreeting
The problem for NHS staffing is retention. Poor pay and awful working conditions. First plug the hole in the bucket
2
0
21
@mancunianmedic
- we were told that you were not infectious 7d after symptom onset
- that positive PCR after 7d did not mean you were infectious 'dead virus'
-this was backed up by lectures and eebinsrs from ID and microbiol consultants
-PHE advice on PPE was late and speculative
1
2
21
@itvnews
@emilymorganitv
Our ethics of clinical practice committee has considered this. The NHS Trust discharges its duty by offering a competent practitioner. There is no right to selection by race. Patient can refuse treatment, & invited to seek it elsewhere if they want. Not covertly colluded with.
0
4
20
@edwinhayward
@pash22
Who will do the training? Will there be a structure? Who will accredit training? You can't just pick it up as you go along. Of course these doctors would not be recognised internationally, so there would option of moving abroad.
3
3
20
This is appalling lazy fear- mongering journalism.
Guidance aims to protect people from nasty medical interventions that won't help. Not ration or discriminate.
The Nice guidelines on who to keep alive aren't pragmatic, they're discriminatory

2
6
20
@mancunianmedic
@sh_abbers
@selkieO
@EmergMedDr
@ClareRayner6
@amibanerjee1
@BinitaKane
@DocStrain
@doctor_oxford
Currently a lot of inpatients are getting COVID in hospital, only picked up on pre care home discharge testing
3
6
20
@implausibleblog
Herd immunity is a vaccine concept. There was no herd immunity to measles or smallpox without vaccines
0
0
20
@PippaCrerar
We want leadership
-on climate change
-on proportional representation
-on restoring public services
-on rejoining the EU.
Not 'slightly less crap than the conservatives'.
@LabourParty
0
1
20
This is complete tosh. Complex services, health, teaching, armed forces need team work, organizations, infrastructure. Diversity in medicine is excellent. Inefficiency comes from over regulation, government policy and diktat. CQC, GMC, PFI...

1
7
20
@drkathrynmannix
@Liz_ORiordan
Much of medicine is palliative. Certainly geriatric medicine. That does not at all mean end of life. The 'curative intent' narrative comes from cancer and only partially applies elsewhere. Altho you could put restorative rehab or some psychiatry in a similar box.
3
4
19
@classicjacko
@houghhough
@nfmusic
@thetimes
@BBCRadio3
@BBC
Radio 3 presenters don't patronise. They are knowledgeable, personable, and do an excellent job in my opinion
@BBCRadio3
0
0
19
@ChrisCEOHopson
Hang on, yes we did, we were told to do so by NHS England. Additional funds were made available to do so. Some of us spun it out to 7 days at least
1
8
19
@parthaskar
@NHSE_WTE
@NHSEngland
@NHSEmployers
@doctor_oxford
@JanetEastham
@HPIAndyCowper
@trishgreenhalgh
@OrthopodReg
@RoshanaMN
@mmamas1973
@ShivaniM_KC
@DrAsifQasim
@AntonEmmanuel2
A government that doesn't believe in regulation as a matter of principle does not enforce it's own rules
0
2
12
@mancunianmedic
Sensitivity of one covid test is 70% two tests 90%. So still a lot of false negatives. On PPE take no chances
0
5
15
#ULEZExpansion
I just looked up which vehicles are affected. Petrol cars registered before 2005, diesels before 2015. So it's a few old diesels. Whose drivers impose a cost on everyone. It is not unreasonable to disincentivise wrecking air quality. Grow up
@UKLabour
4
0
16
@Trisha_the_doc
@DrAnnaDixon
Geriatricians must claim this expertise. Frailty EOLC is different from cancer eolc
1
1
16
@MattHancock
I don't understand why we all need to travel to Durham to do so though. Won't it get awfully crowded?
2
1
15
@giles_fraser
So exactly how does making things worse and tanking public services actually help? Right problem, wrong answer. EU cares more than Tories do
2
1
14
@MattHancock
But our computers take 10mins to boot up. And the WiFi doesn't work in yellow Bay. And we have unusable medical records software.
1
0
16
@HPIAndyCowper
We've had half a dozen radical shake ups in the 30 years I've worked for the NHS. None of them helped anything.
0
0
15

@bmj_latest
@mancunianmedic
Higher training in geriatric medicine has an ambitious list of end of life competencies. Please can we avoid suggesting that geriatricians do
not provide 'specialist' end of life care? We collaborate very well with palliative medicine. But please give us the time and resources
0
2
15
@Suewilson91
Clearly Starmer does not understand the needs of health and social care, universities, music and creative industries, IT, finance. And more. Or that FoM can be mutual and to our benefit. And the amazing invitation and renovation that multiculturalism brings
0
0
15
@ShaunLintern
@JohnWest_JAWS
@nottmhospitals
Don't blame the hospital, the system is under capacity, underfunded and under commissioned. Community and social care provision is also full. COVID, flu and RSV are everywhere. The population is getting older. Wards already going '3 over' their intended capacity.
3
4
15
@UKdemocrat
... or even. Double the salary and ban second jobs. It's important enough. And you need to attract the high achievers
14
1
15
@wesstreeting
Please remind us what you said about people living with dementia? In the HoC referring to the member for Islington. Think about how inappropriate it was. And then resign.
2
2
14
@dan26wales
@DacreJane
@RCPLondon
The problem is that box 2 could describe an ill, delirious older person. Yes they might die. But equally they might not. Paeds have a thing called parallel planning. Fits the problem rather better
4
1
14
@toates_19
Because specialist generalists like geriatricians are better at the totality of care. The problem is capacity, esteem and access. Acute medicine is seen as a problem not a premium service. So our work is not valued. And ward work is tough. So capacity suffers.
1
1
14
Dr Emily Oliver:the importance and reality of relationship centred care for people with dementia in acute hospitals. East Midlands Dementia Day
@emilyoliverdem
@GeriSoc
@HcopTeam
@NUHMedicine

0
2
14
@drtomround
@wesstreeting
This is utter tosh from
@wesstreeting
. He is hopeless. Let's remember how he insulted people living with dementia in the HoC. He should resign
0
1
14
@mancunianmedic
-PHE advise was probably driven by concerns about supply, and many said as much at the time
-the failure was one of infection control. Think of the scrupulous measures to control CDiff or MRSA. The COVID response was nowhere close
1
2
14
@Keir_Starmer
Increasing NHS training numbers won't help if you do nothing about retention. Of course freedom of movement might help
0
2
14
Fluid resistant surgical masks (FRSM) were never credible protection. You breath round the side of them, not through them. They may limit an infected person spreading virus around but do not protect the wearer. On acute geriatric medical wards the issue is prolonged... 2/n
1
3
14
@cpeedell
@ShaunLintern
@HSJnews
for frail and confused older people 1 nurse to 8 patients no where close to adequate
1
13
13
Just saw this La Traviata
@RoyalNottingham
. Brilliant from
@Opera_North
, who always deliver. We get 3-4 days opera 3 times a year. I grew up with
@E_N_O
. Lets try to save it. But please don't sacrifice
@Opera_North
in the process
0
0
13
@wesstreeting
@RichardJMurphy
We have been trying prevention for decades. We do it a lot and it works. To do more we would need to intervene on a lot of people who won't benefit. Look up sensitivity and specificity. And use interventions with marginal or unproven benefits. The NHS is simply underfunded.
2
2
13
@mancunianmedic
My request to put 5 motions to an indicative vote of MRCPs was denied
#egmrcp
2
3
13
@mancunianmedic
-there is no evidence on whether O2, fluids, +/-antibiotics, enhanced nutrition, protection from complications and early professional rehab improves outcomes, but I would not assume it does not
1
2
13
@AlpMehm
Being in the EU Brings many benefits, including Freedom of Movement. We will all be better off if we stay in EU.
0
0
11
@mancunianmedic
We asked families about this in a trial (BMJ 2013 347 f4132). 22% said discharged too quick, 67% about right, 11% delayed. BTW readmission does not imply error, but may do
0
4
13
A good start but some concerns
CFS is fundamentally a disability scale only indirectly related to frailty.
That said chances of CFS>=5 surviving ITU or CPR are remote not 'uncertain'
@runnermandoc
@delirious_dr
1/n
2
1
11