
Marnix Jansen
@jansen_marnix
Followers
2,942
Following
4,129
Media
578
Statuses
7,438
Computer vision in pathology @UCLcancer and @UCLH . Cancer Research UK Clinician Scientist and Consultant Histopathologist. Londoner, father of 2
London, England
Joined May 2015
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
América
• 509284 Tweets
Sant Rampal Ji Maharaj
• 331240 Tweets
#母の日
• 210049 Tweets
#MothersDay
• 116954 Tweets
ヴィクトリアマイル
• 90728 Tweets
Newwiee Honey Teerak🩷
• 54796 Tweets
ストフェス
• 49991 Tweets
Chivas
• 41967 Tweets
Pachuca
• 37791 Tweets
カーネーション
• 37697 Tweets
Roger Corman
• 33559 Tweets
Loma
• 23886 Tweets
ナミュール
• 22437 Tweets
#AnnelerGünü
• 22193 Tweets
Toluca
• 15702 Tweets
マスクトディーヴァ
• 13404 Tweets
#मातृ_दिवस
• 10153 Tweets

















Random story
My dad passed away unexpectedly two weeks back. We had a private remembrance service last week.
This morning a card arrived in the mail for the grandkids which my father sent days before passing and had been making its way here since then.
Priceless. Thanks dad!
161
93
4K
- Yes OR 6? I'm calling in a frozen station 13.
- Okay,..[crackle] ..tell us [crackle].
- Its not malignant.
- Are you saying it's [crackle] malignant?
- It's not malignant!!
- (surgeon shouting across the floor) DID YOU SAY MALIGNANT??
- IT'S BENIGN!!! THERE AINT NO CANCER!!!

13
40
283
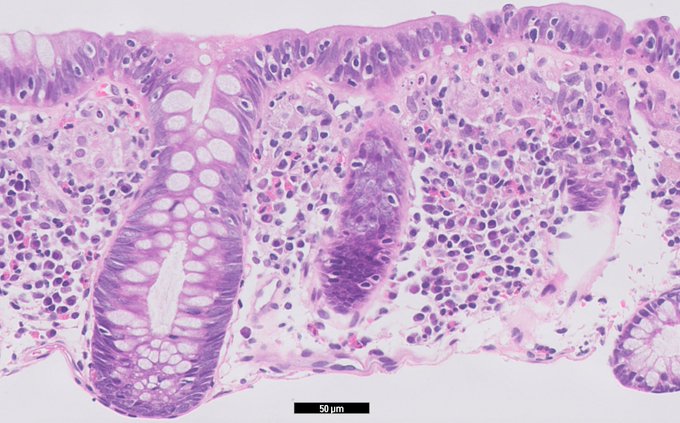
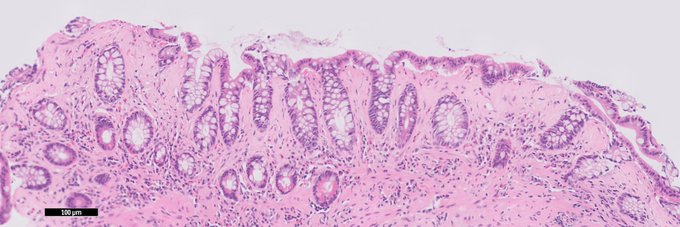
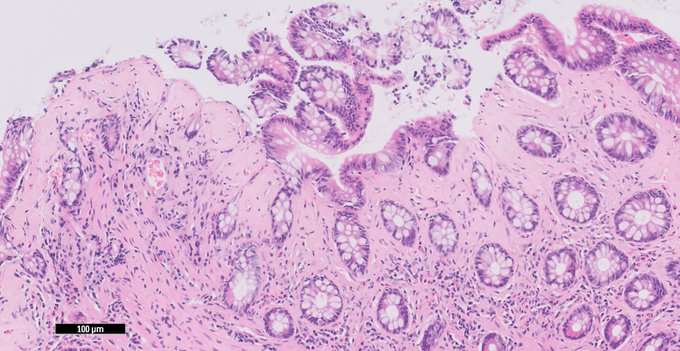
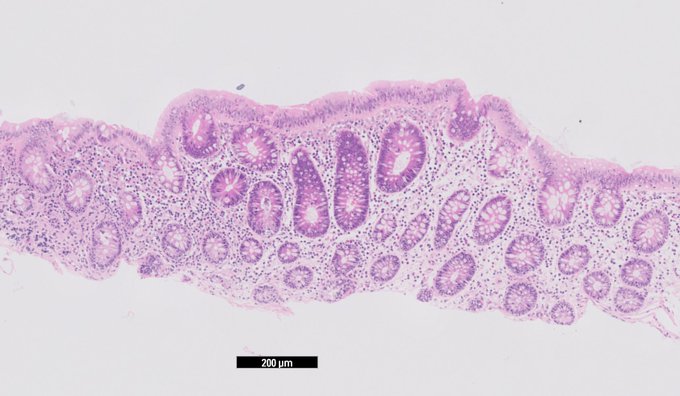
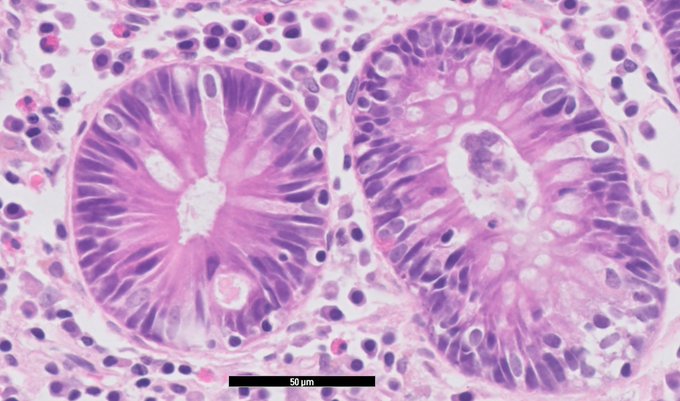
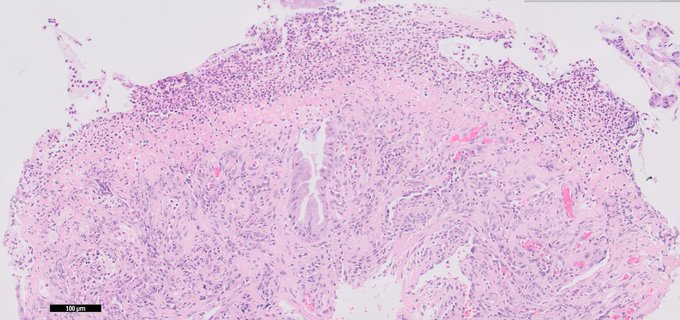
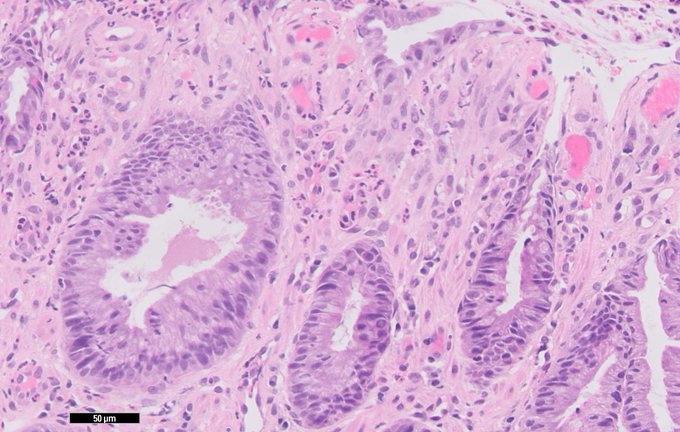
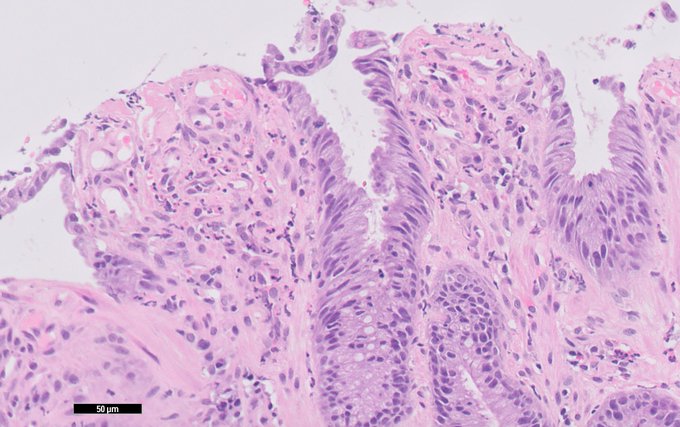
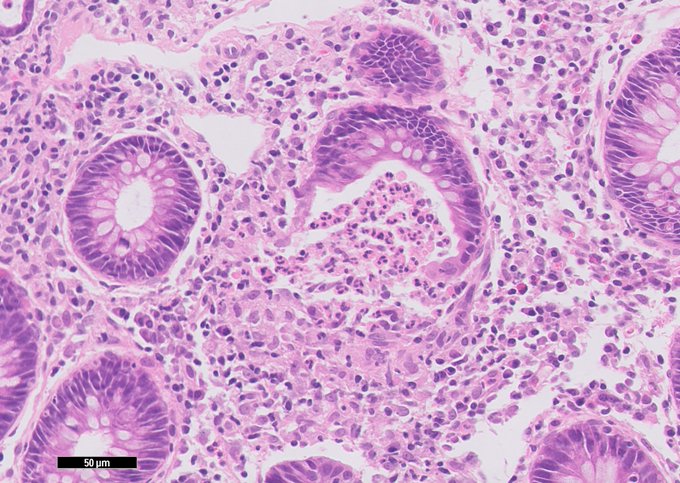
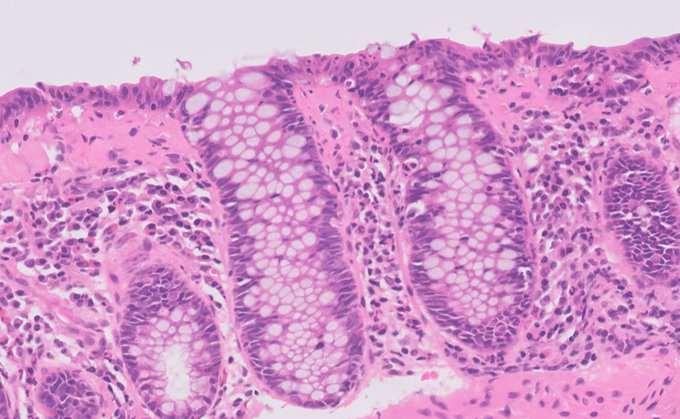
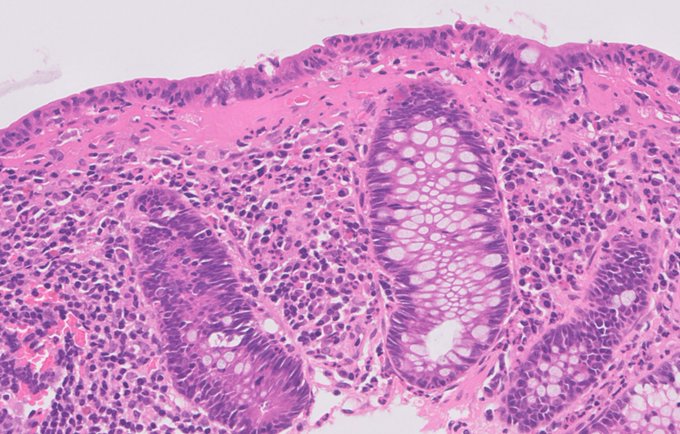
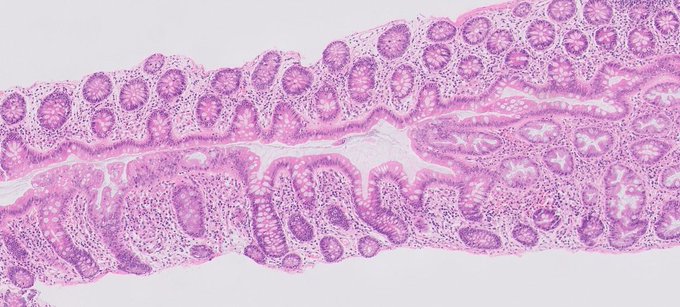
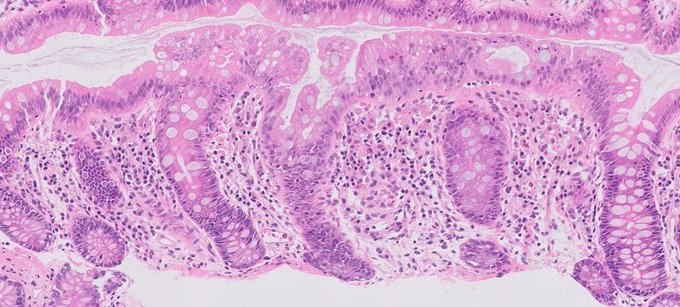
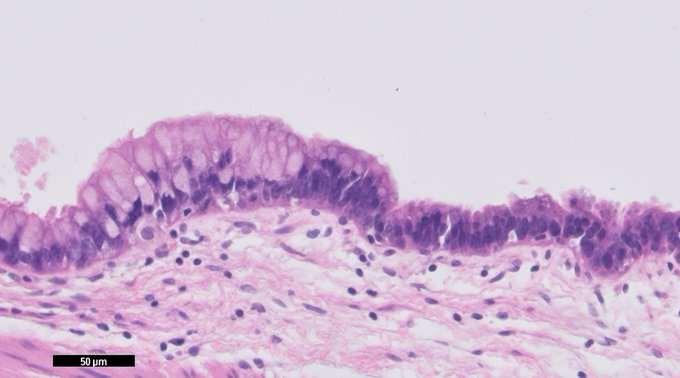
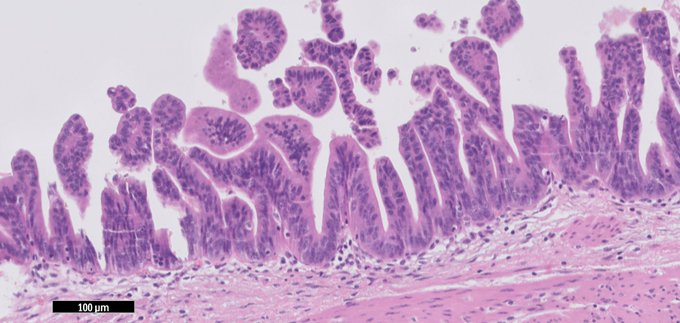
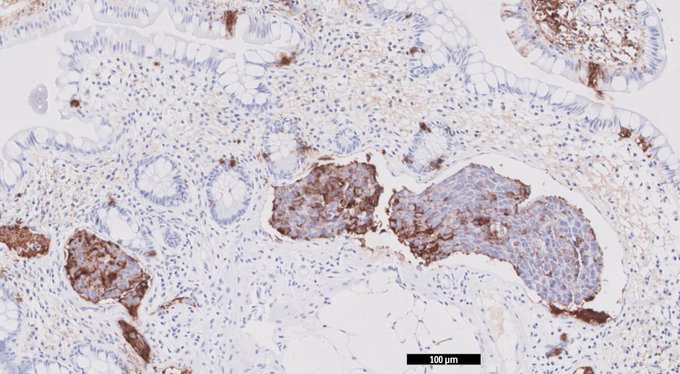
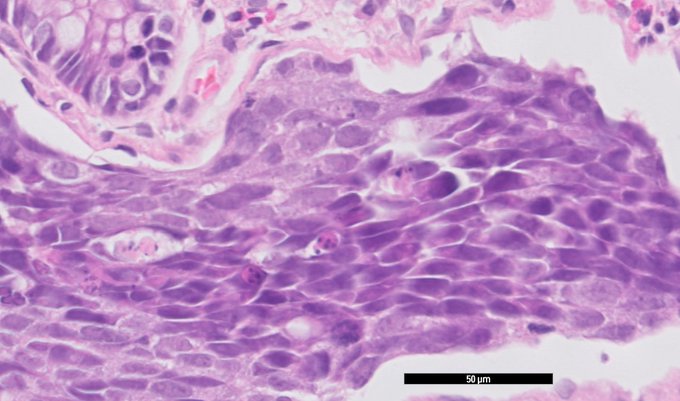
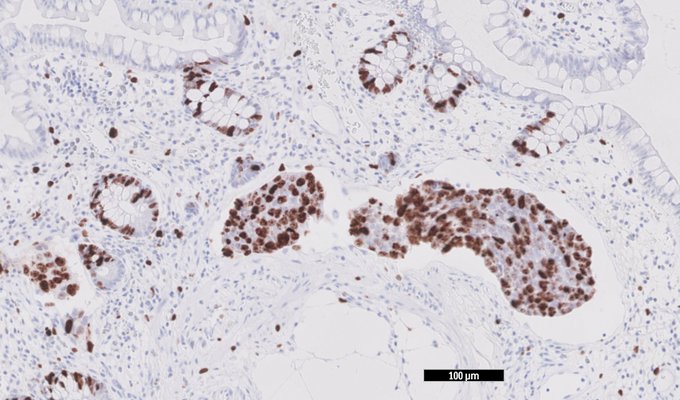
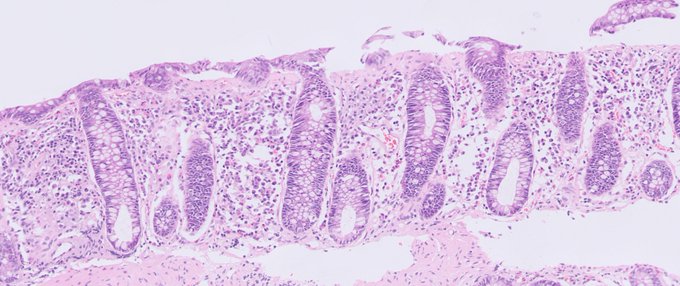
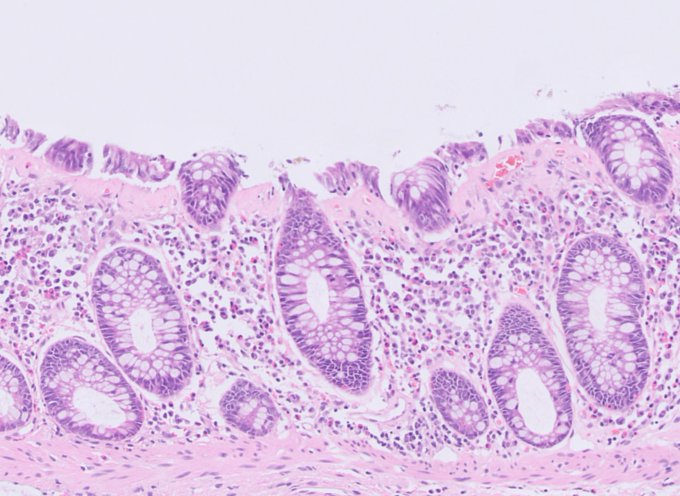
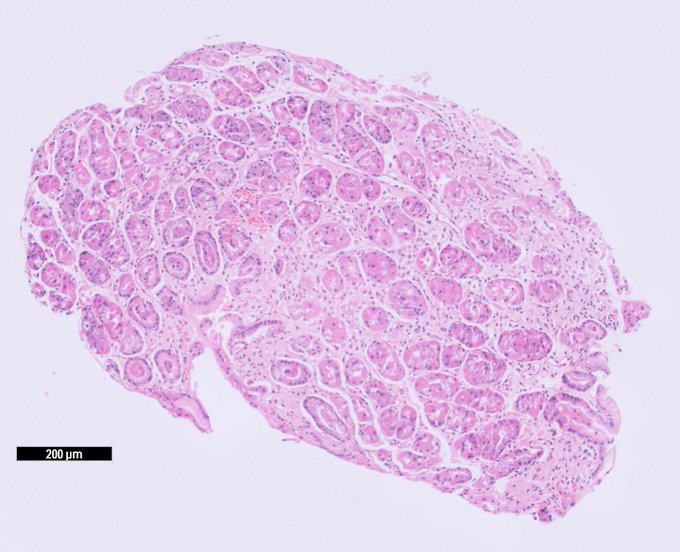
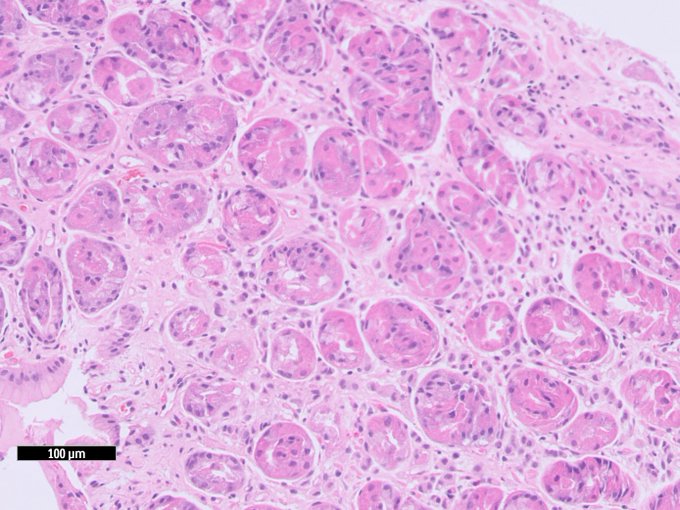
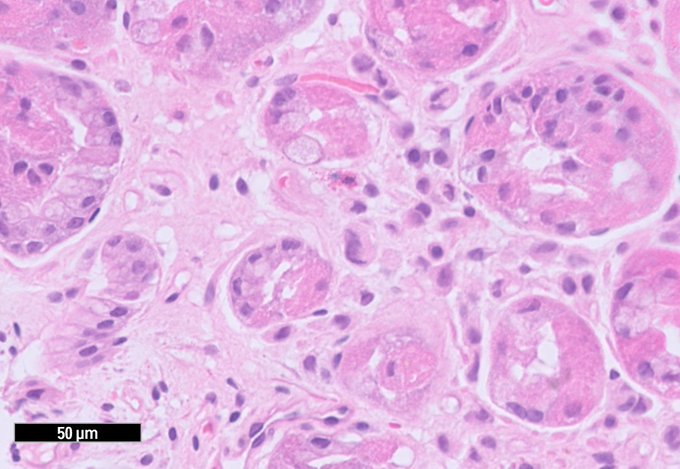
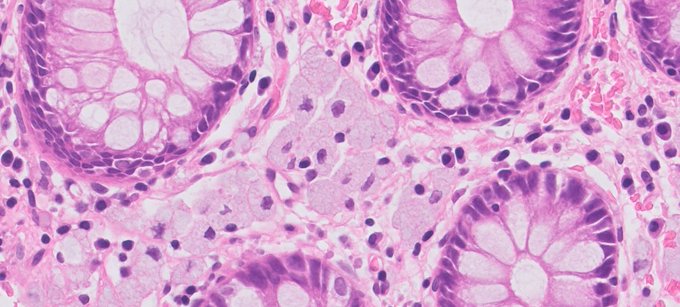
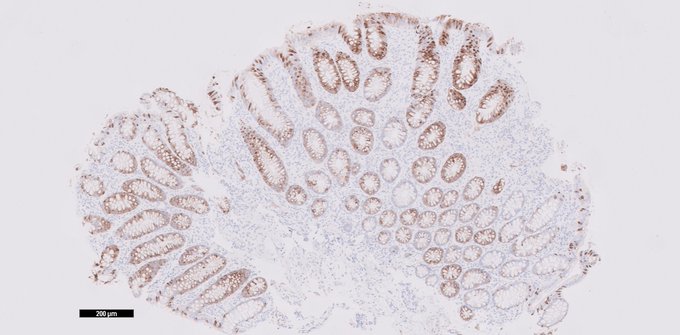
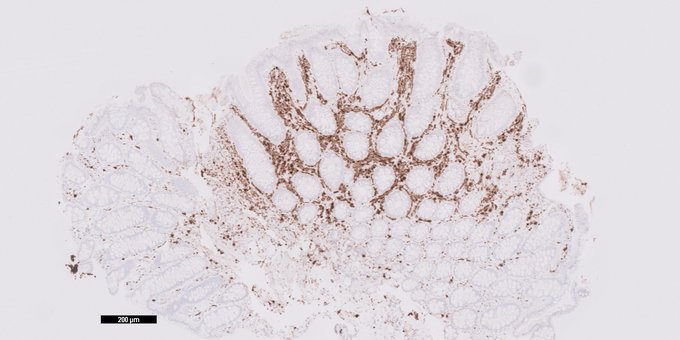
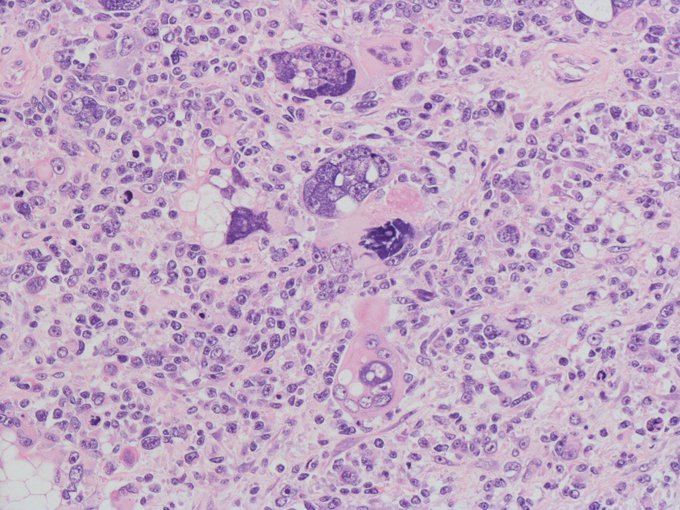
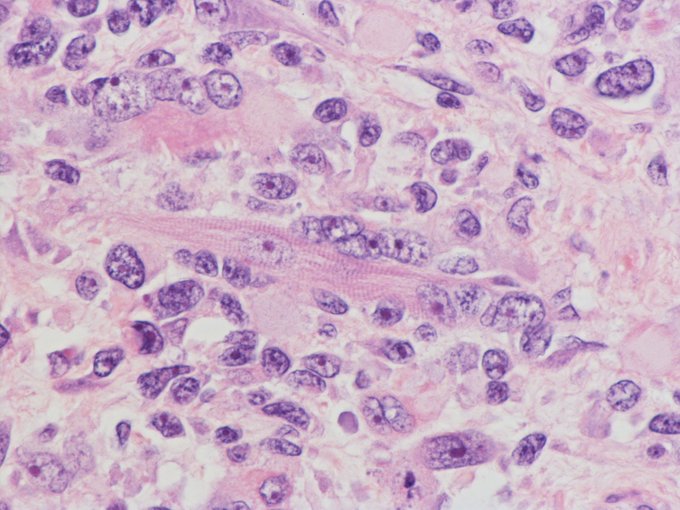
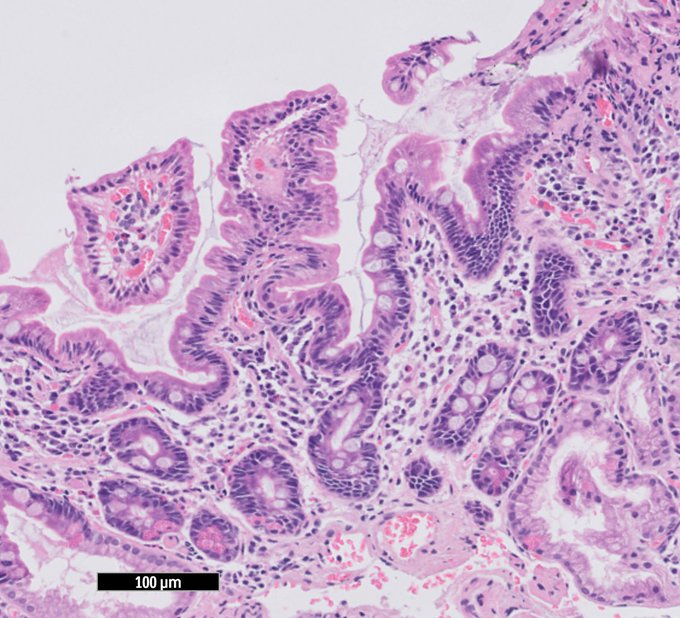
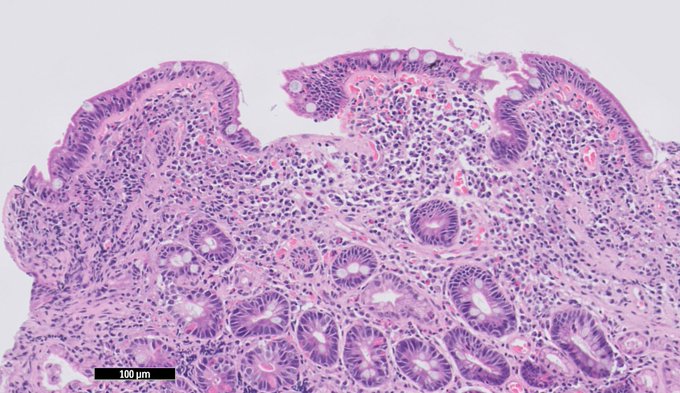
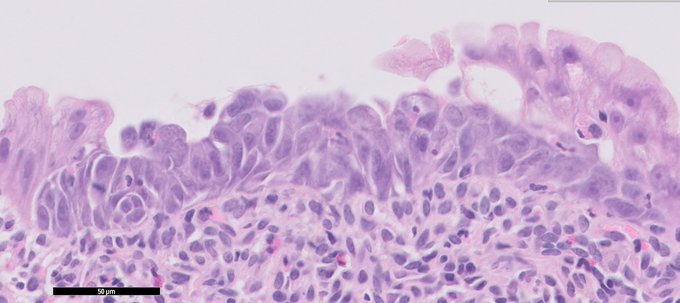
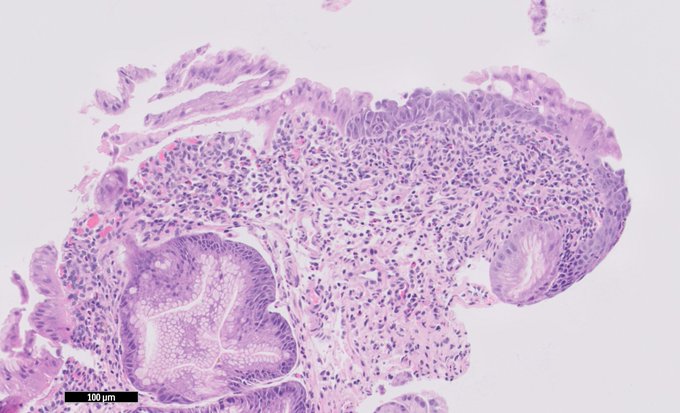
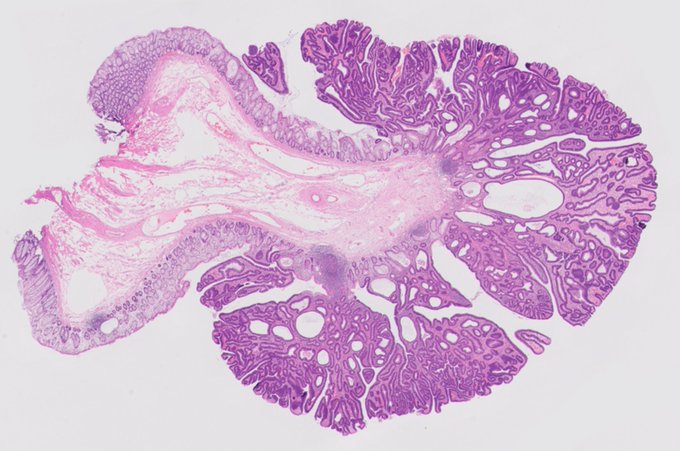
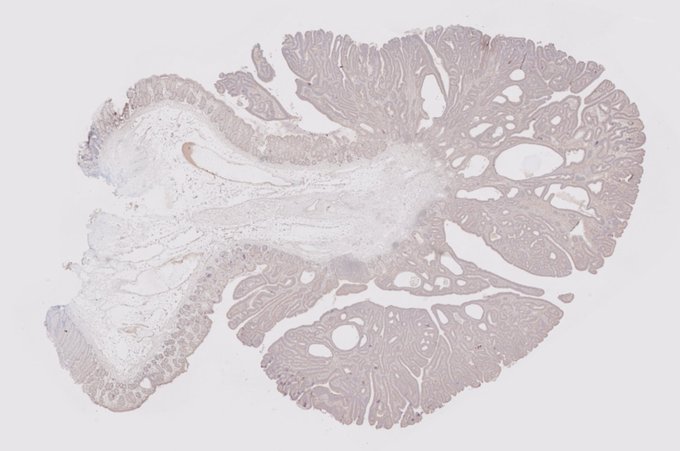
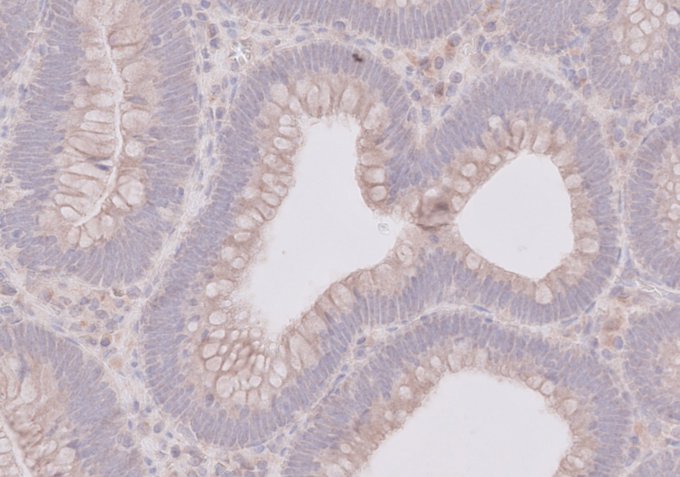
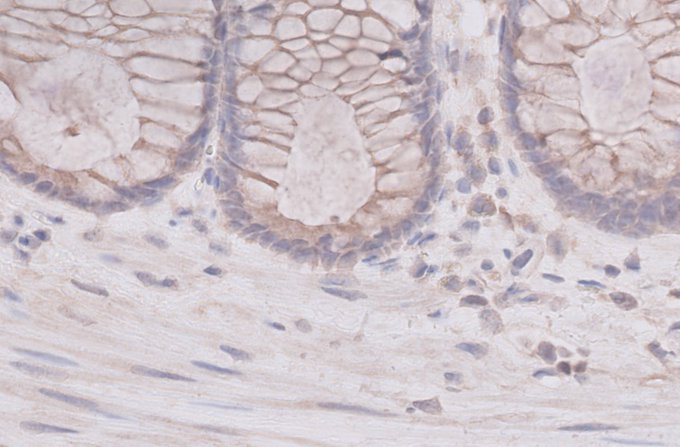
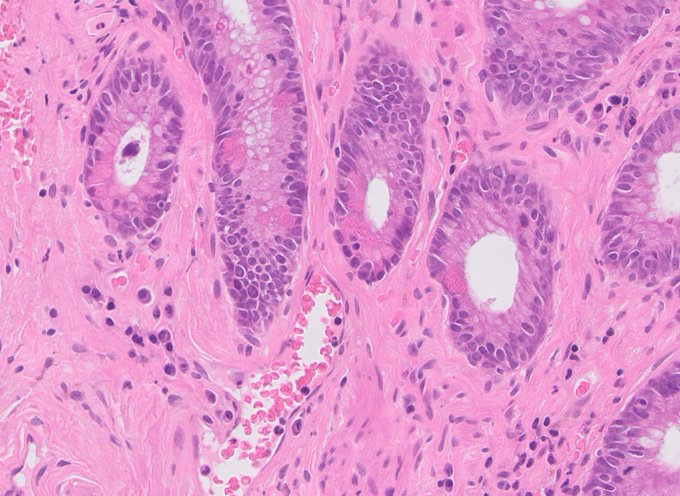
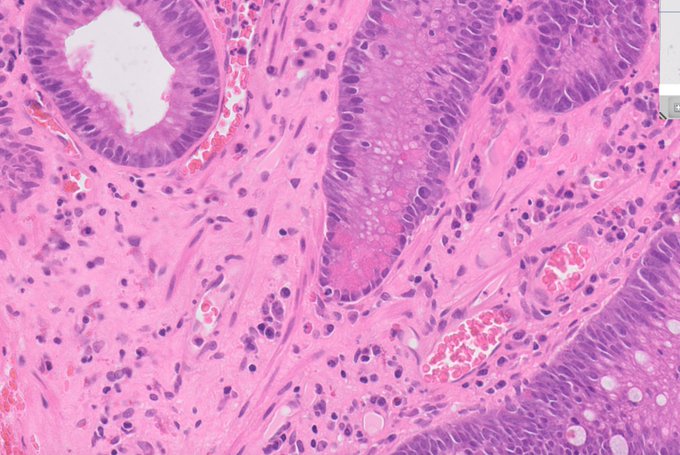
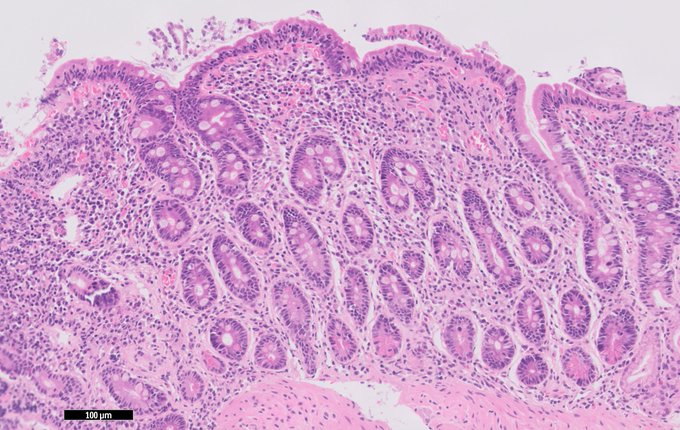
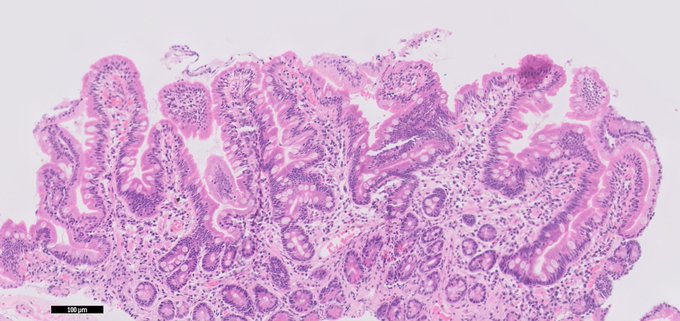
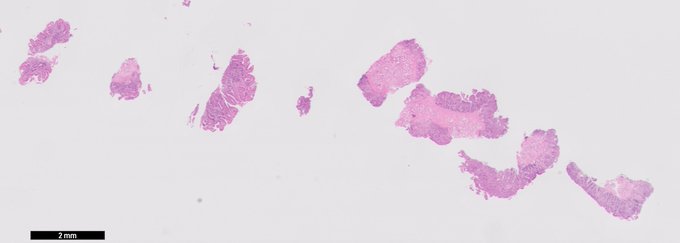
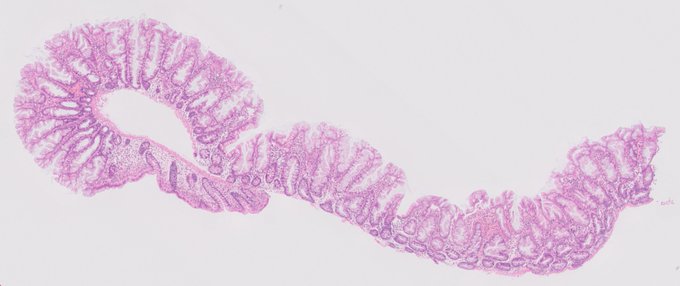
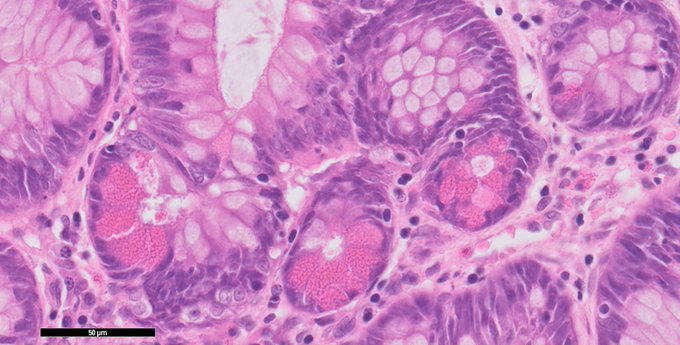
Here's an odd 🐦
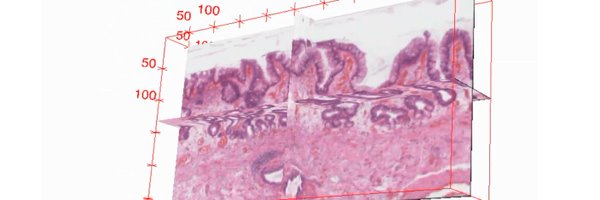
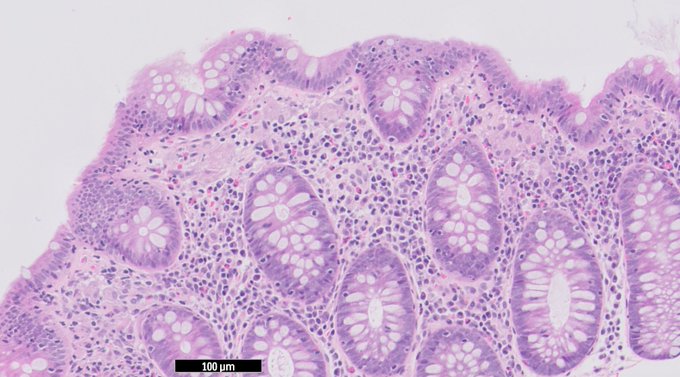
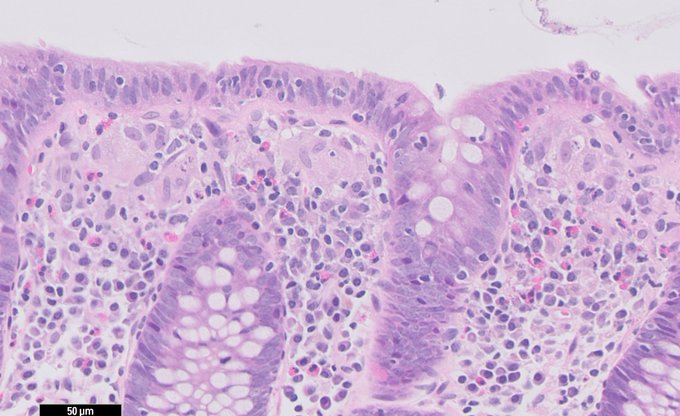
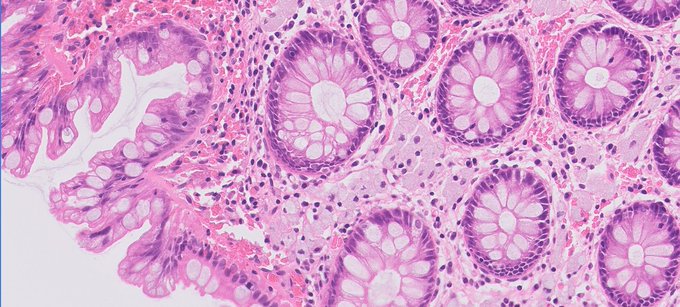
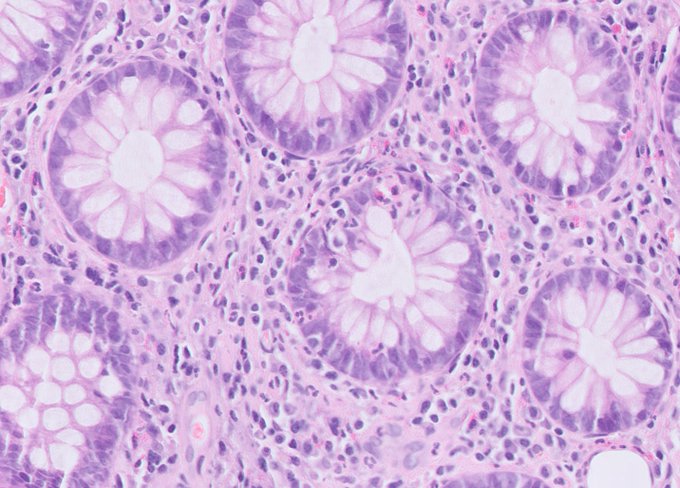
Microscopic colitis pattern, but you find rows of giant cells and macrophages have accumulated in the upper mucosal reaches.
Normal colonoscopy, no medication, usual reason to investigate.
What's going on?
#GIpath

9
53
165

Massively proud PI hugging freshly minted PhD Hamzeh Kayhanian who defended his PhD thesis today and passed with minor corrections.
@uclcancer

12
0
131
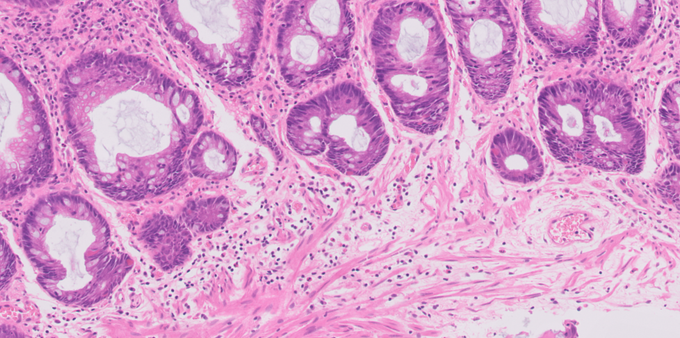
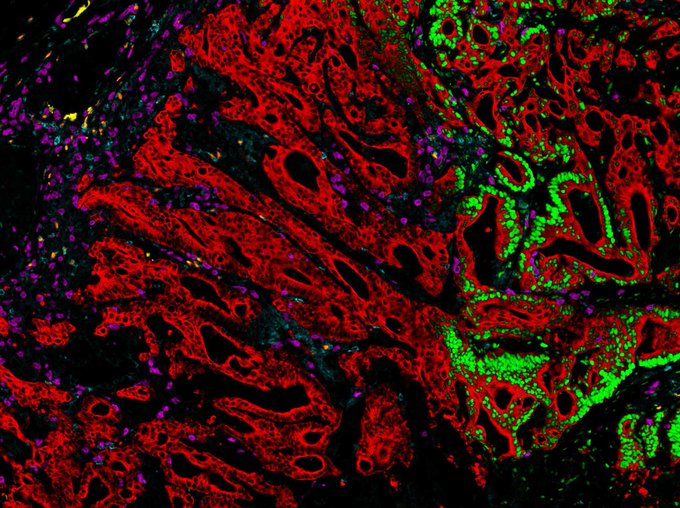
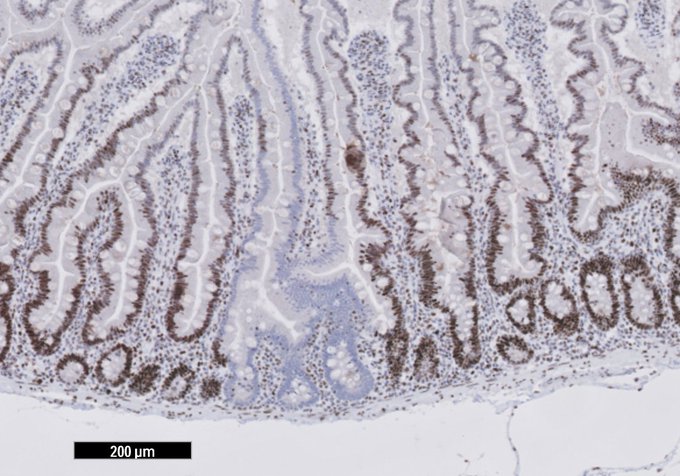
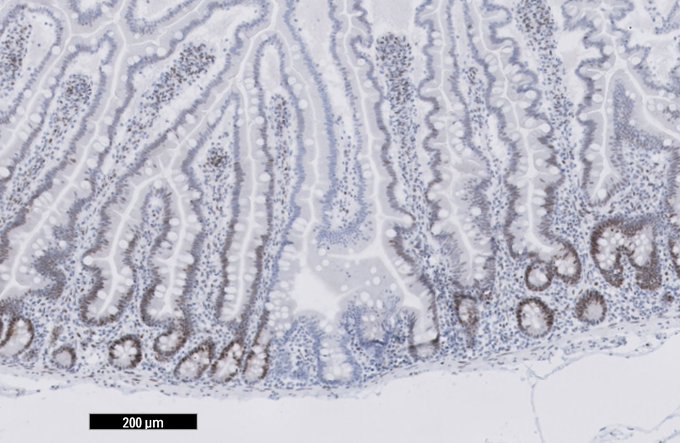
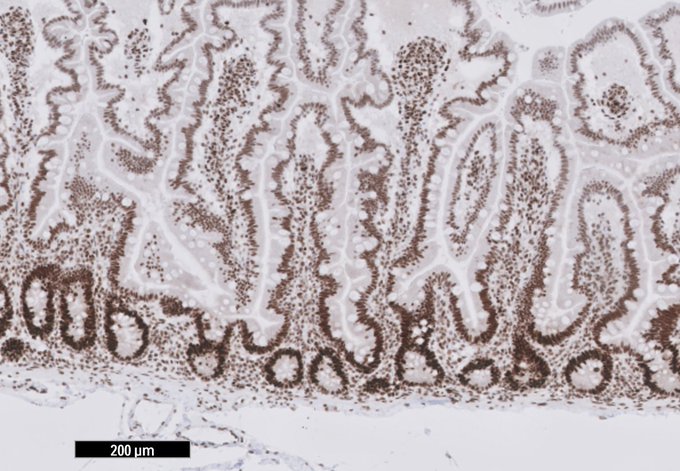
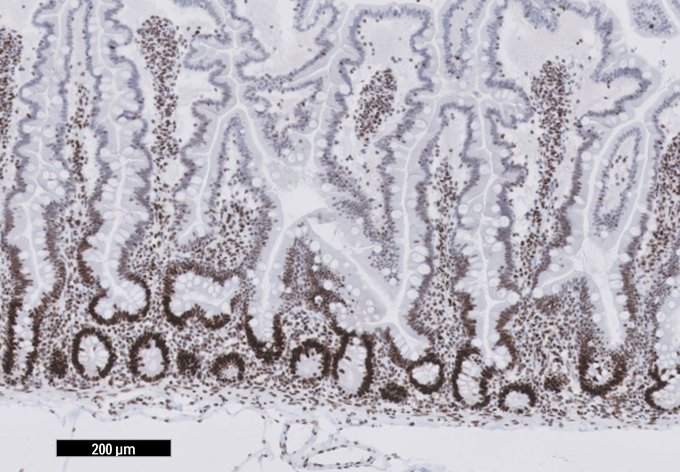
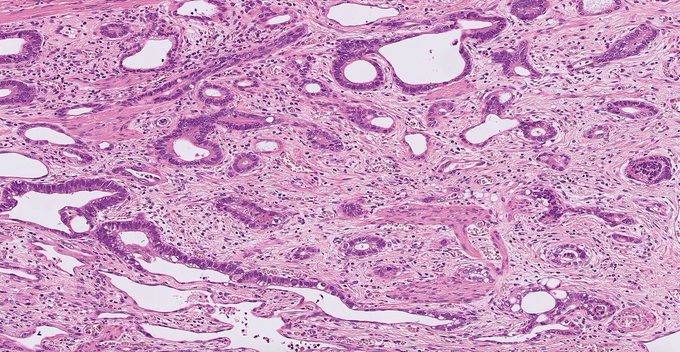
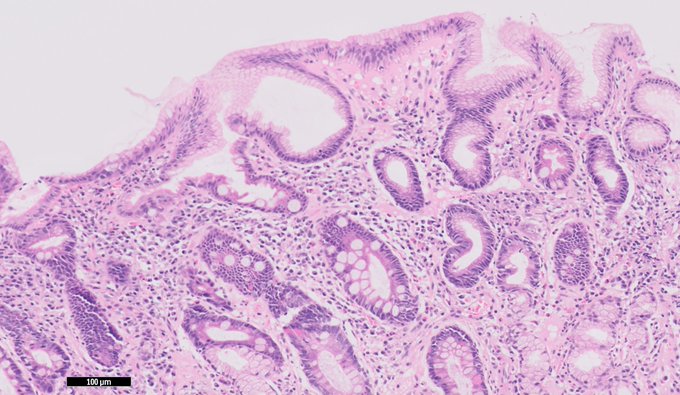
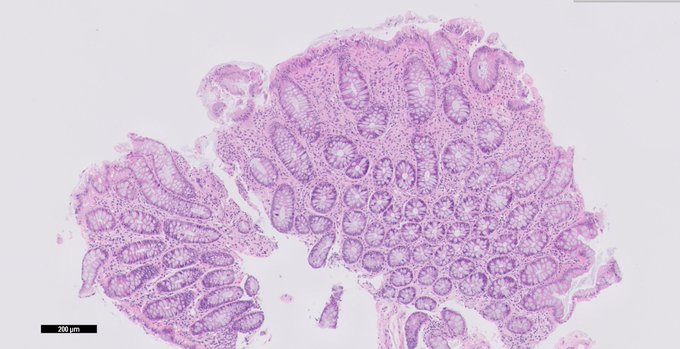
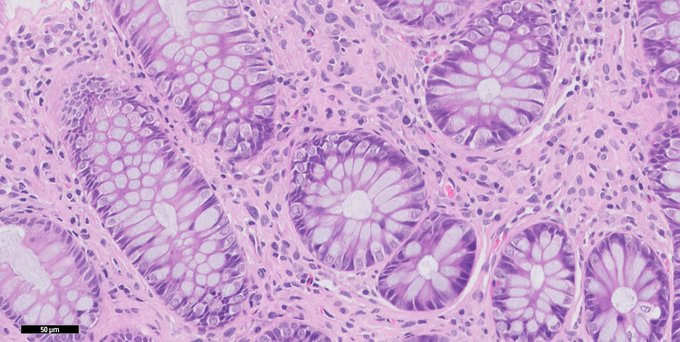
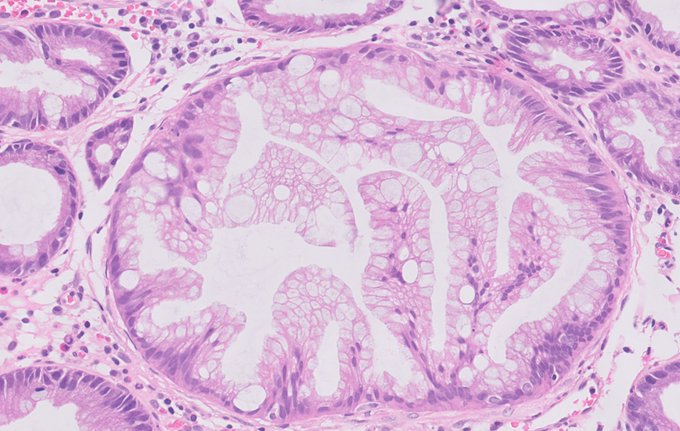
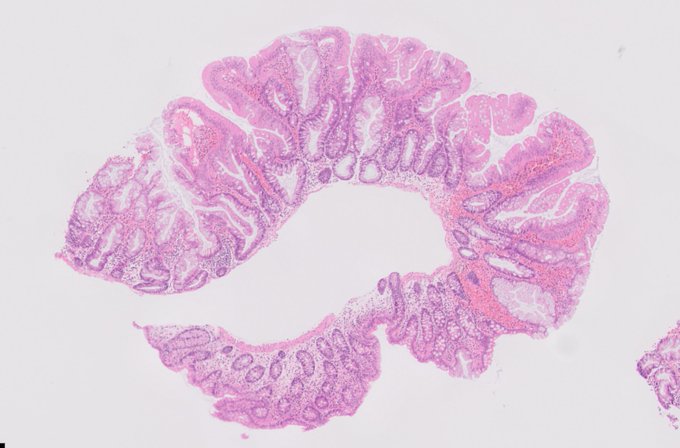
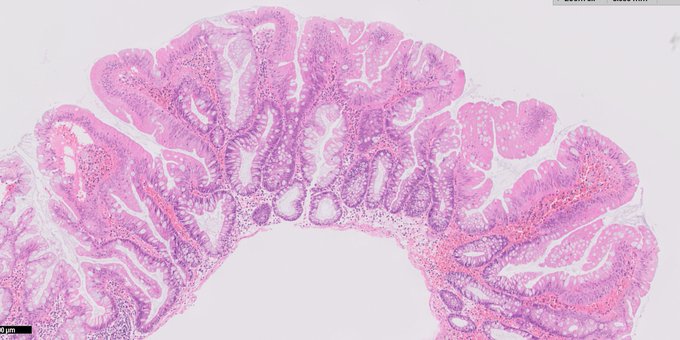
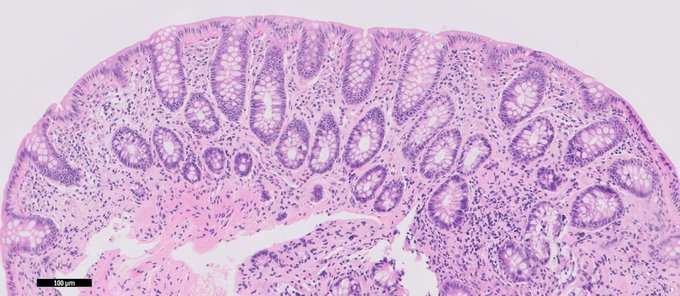
Small adenoma in a young Lynch patient. The MMR proteins involved are MSH2 and MSH6.
#GIpath
3
50
118
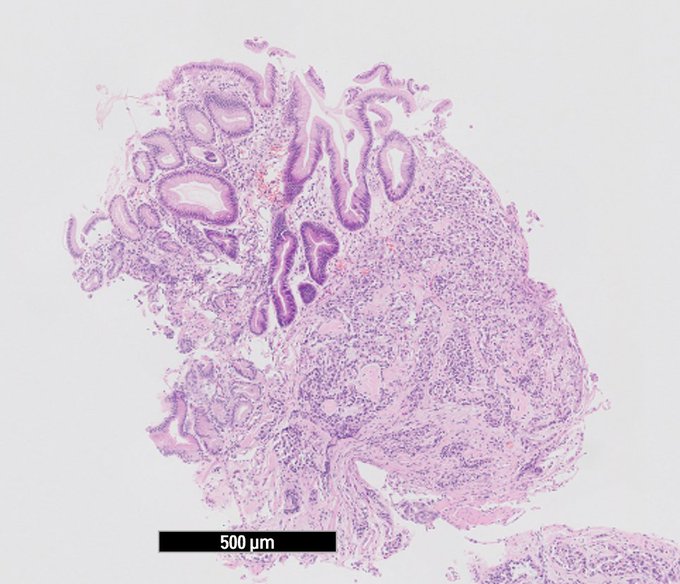
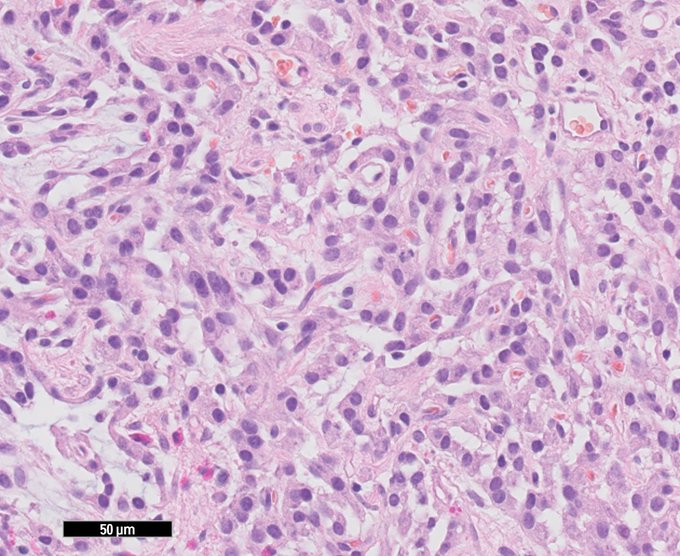
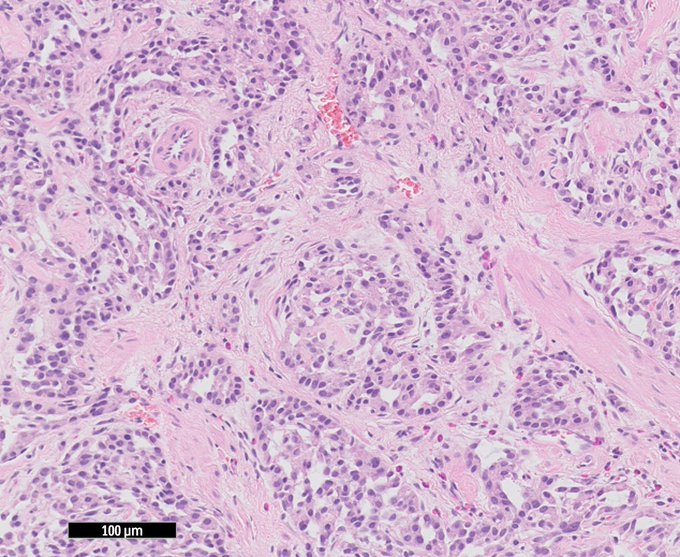
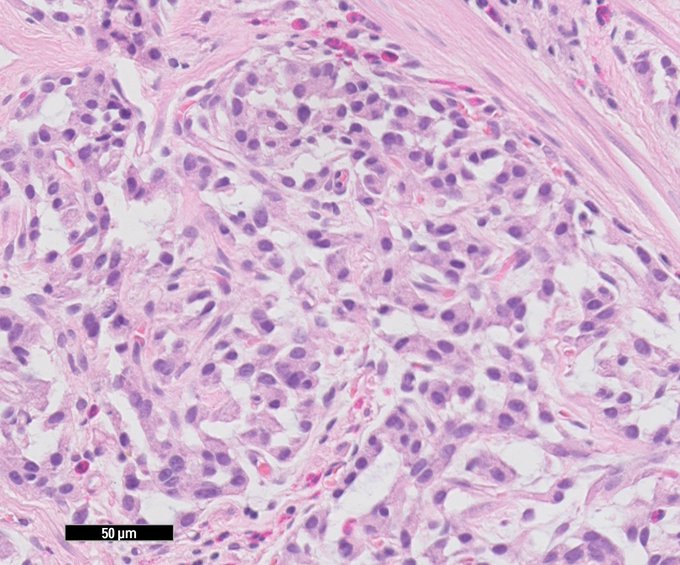
Case for trainees.
Urgent biopsies of a 3cm palpable mass on the anterior wall encroaching the dentate line. What do you tell the endoscopist?
17
45
106
EUS-FNB of a small paraduodenal lesion
Which immunos are you ordering? Likely gene mutation?
#GIpath
9
35
90
We got married 8 years back with 20 guests. Turns out we were way ahead of the game.
#ceremini

10
0
91

My dad will meet one of his grandchildren tomorrow for first time due to pandemic and I can't sleep.
4
0
76
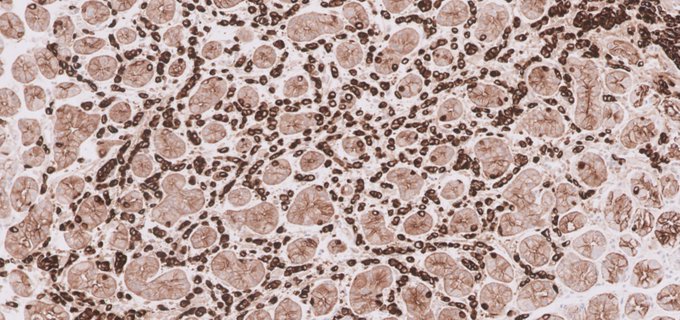
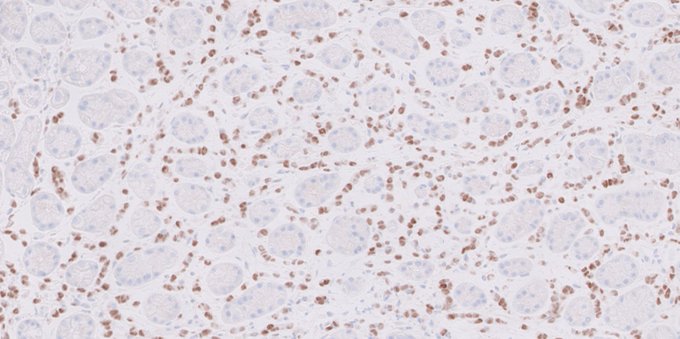
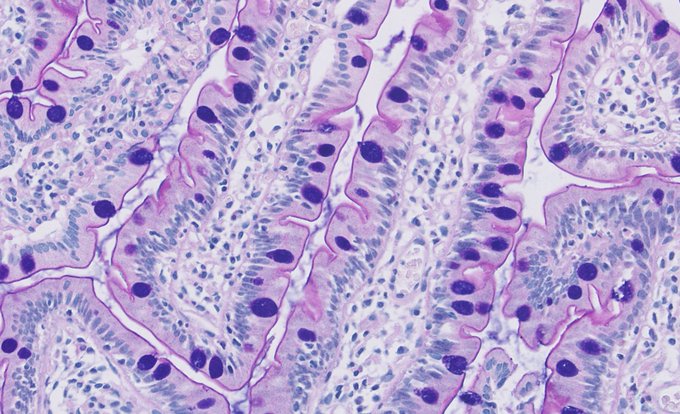
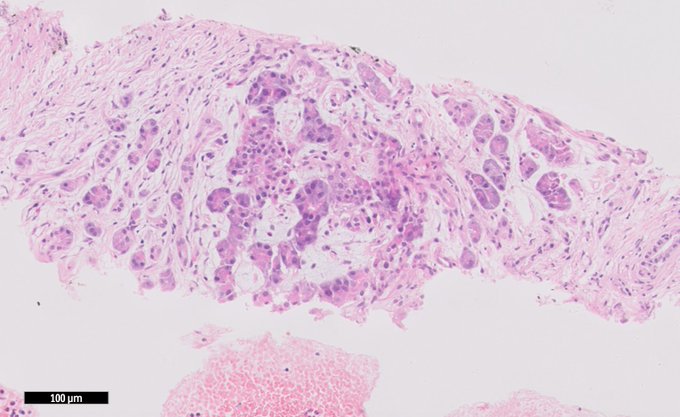
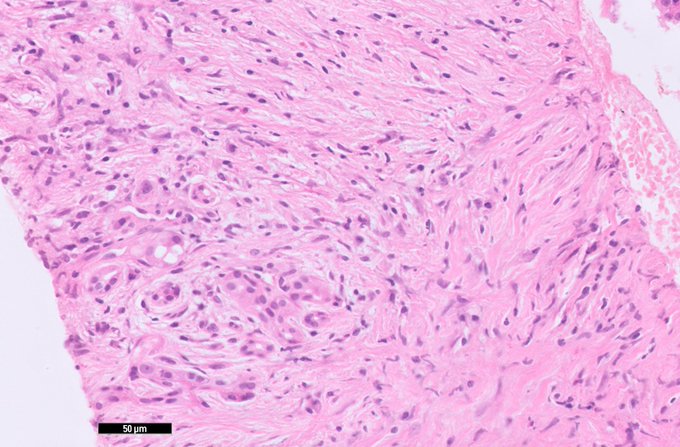
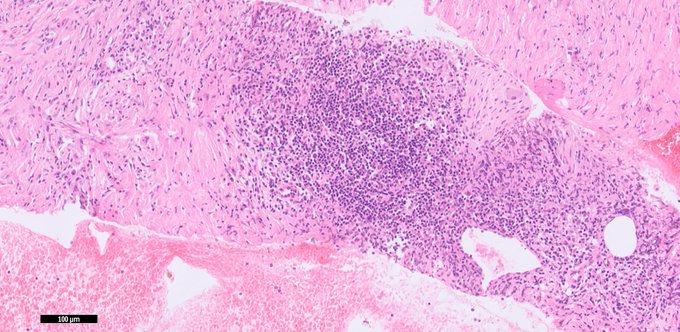
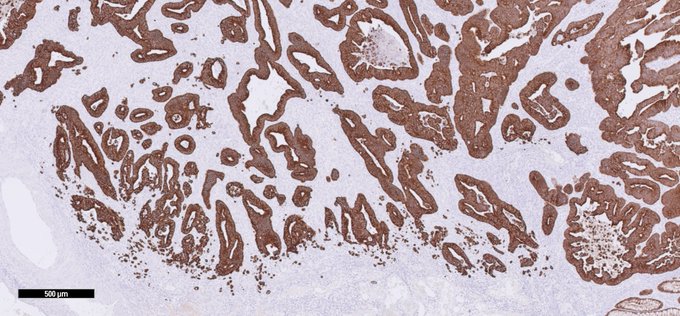
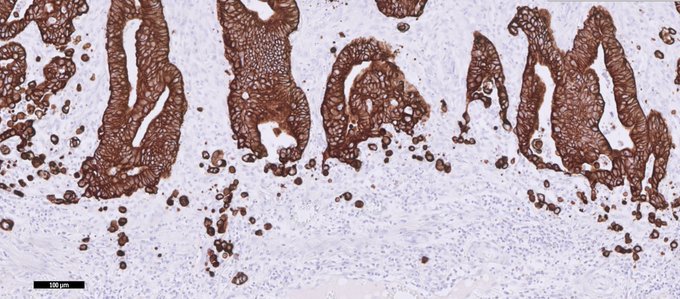
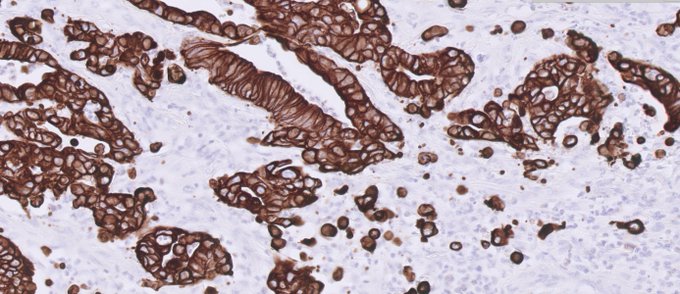
Classic stuff
Keep an open mind when the infiltrating population lacks classic signet ring morphology
H&E, pan-Keratin, and ER
#GIpath
6
21
77
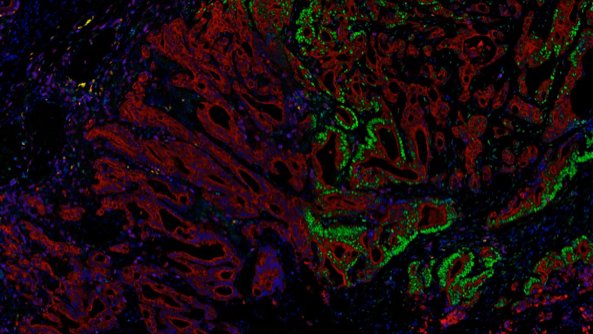
What evolutionary trajectories drive immune evasion in MMRd colorectal cancer?
We identify an unexpected new mechanism driving subclonal mutation rate and mutation bias differences in MMRd cancer. This fuels intratumour heterogeneity and immune escape.

6
20
72

10
11
74
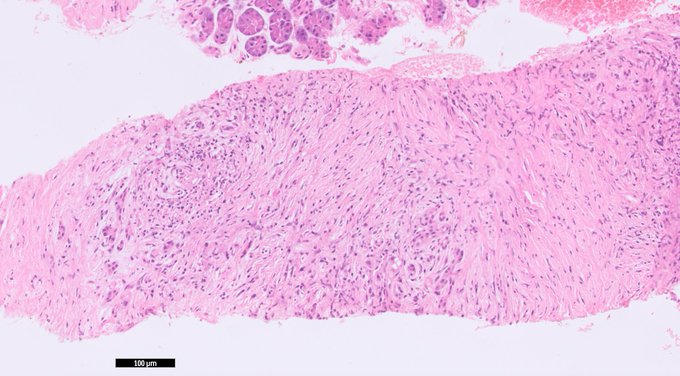
First round of immunos on that retroperitoneal spindle cell lesion
6
15
71
Diagnostic feature that I feel does not receive nearly as much airtime as it should.
SSAs often reveal normal crypts between serrated crypts, indicating they (clonally) expand and creep in between existing crypts, HPs don't do this. Bonus: can use this even in crosscut sections!
4
23
69
40M pancreatic biopsies
#GIpath
You get one last slot on the next IHC run. Which box are you ticking?
5
20
66
Incidental 3mm polyp distal rectum. Mucosal prolapse may provoke crypt changes which can begin to mimic SSA/SSL glands. Don't let prolapse fool you.
3
24
66
Hey what's this?
Oh, just classic low grade dysplasia, foveolar-type in a Barrett's EMR specimen
#GIpath
3
10
66
Our cherry tree in the garden is so beautiful this time of year.

0
4
64
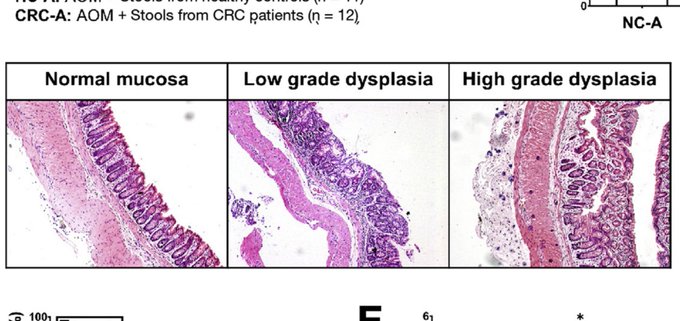
Poor pathology review by a top tier clinical gastroenterology journal, neither of these examples shows dysplasia!
12
28
59
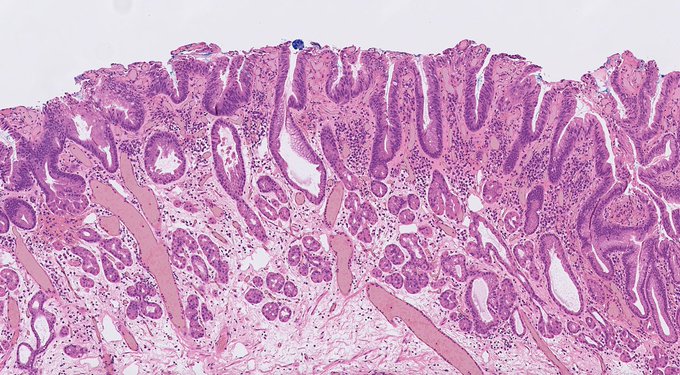
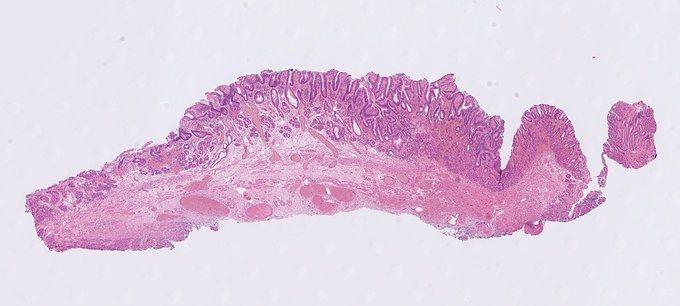
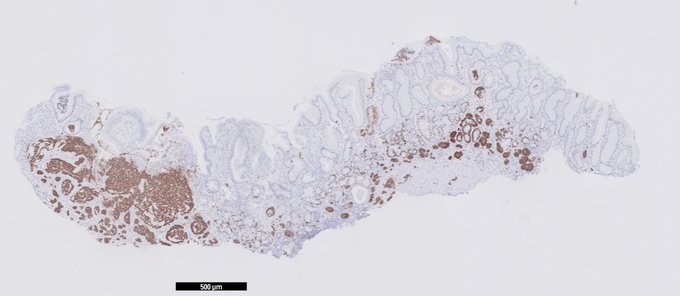
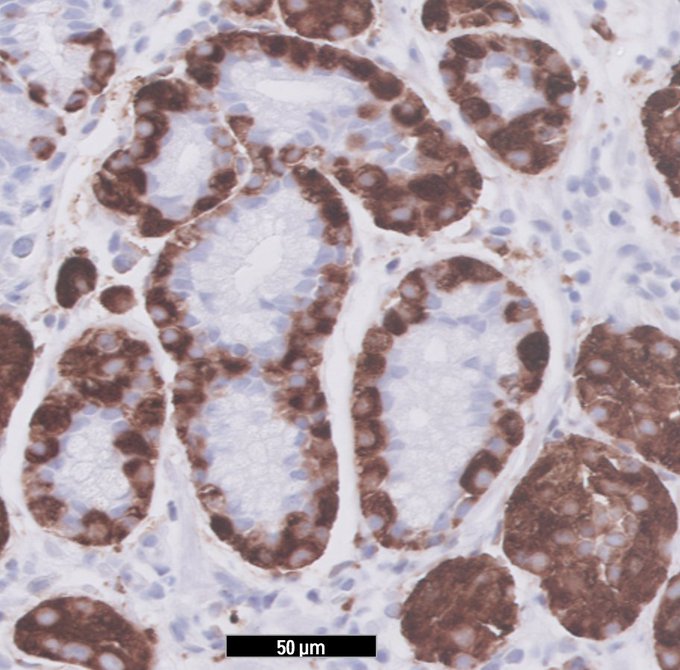
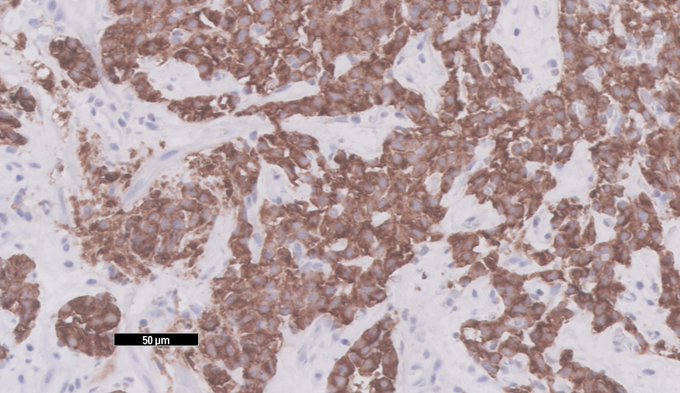
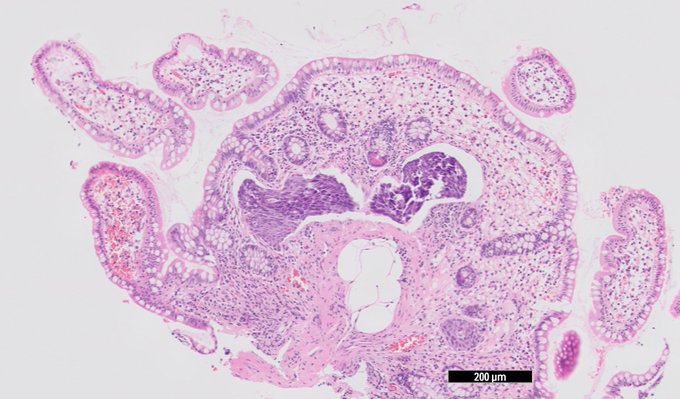
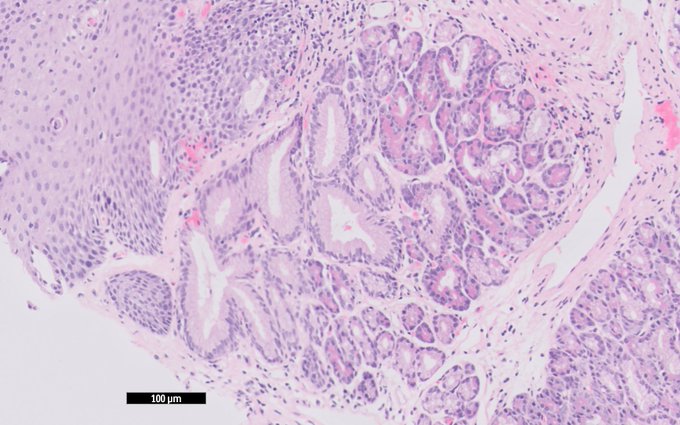
Linear ECL hyperplasia, nodular hyperplasia and invasive carcinoid, all in one view.
Autoimmune gastritis with mucosal atrophy and NE hyperplasia.
#GIpath
1
18
58
Small intestinal biopsies (historic case). What's your diagnosis?
IHC shows chromogranin and MIB1.
#GIpath
12
17
55
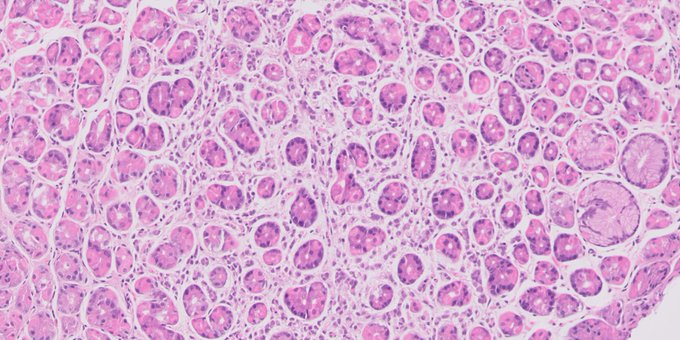
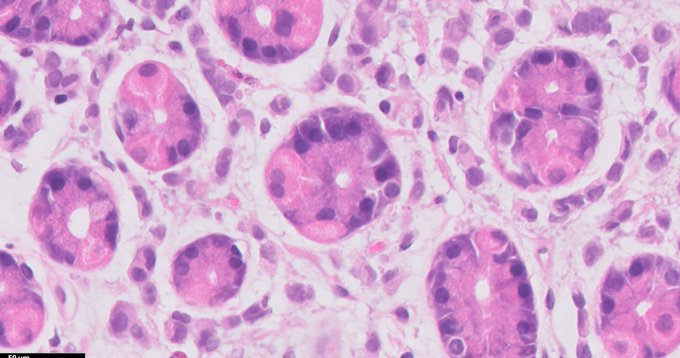
Gastric biopsies
IHC is AE1/3 (obvi)
What do you think I am NOT showing you?
6
17
56
6
22
56
Oesophageal biopsies, how would you grade this?
See our recent work on pathologist predictors of diagnostic proficiency in Gut
#GIpath
18
22
55
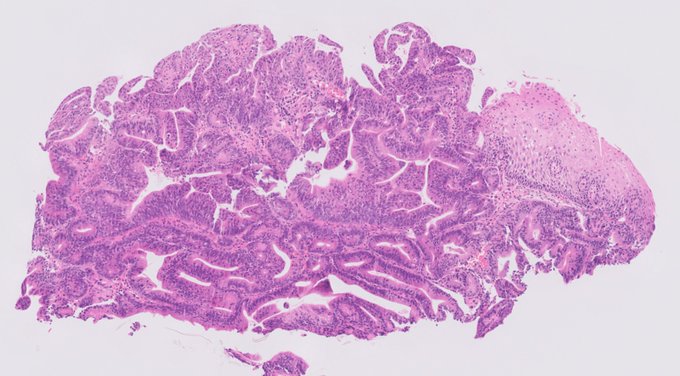
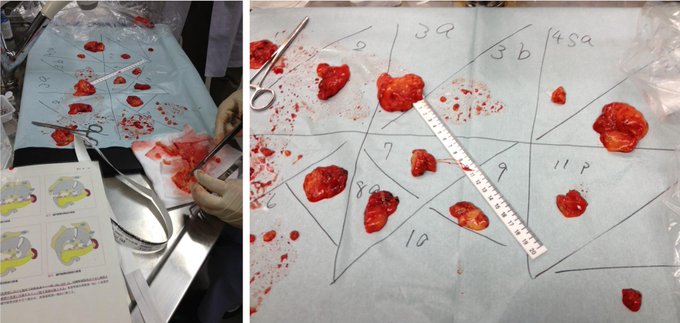
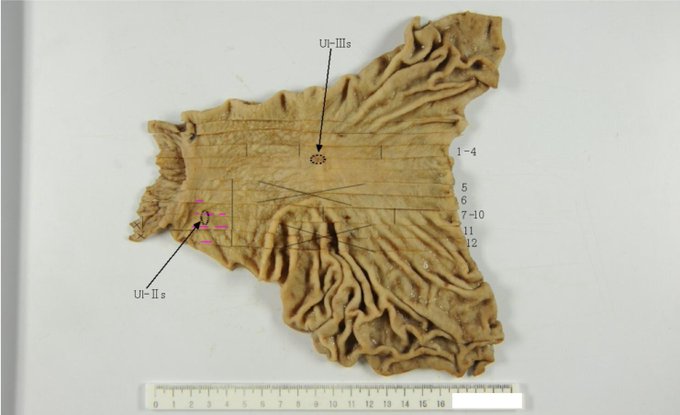
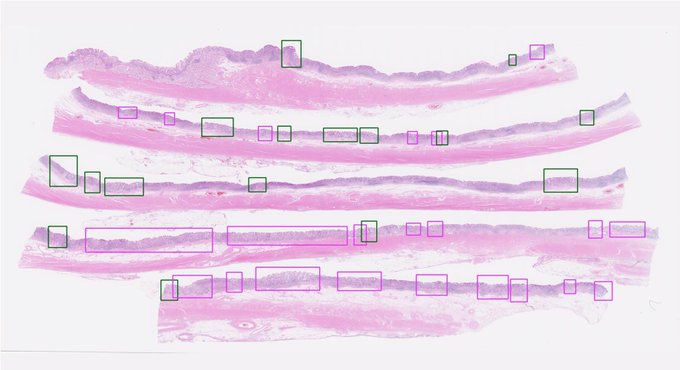
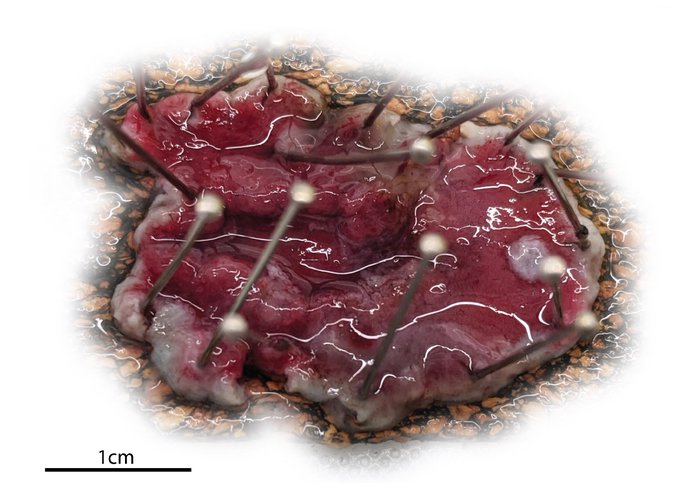
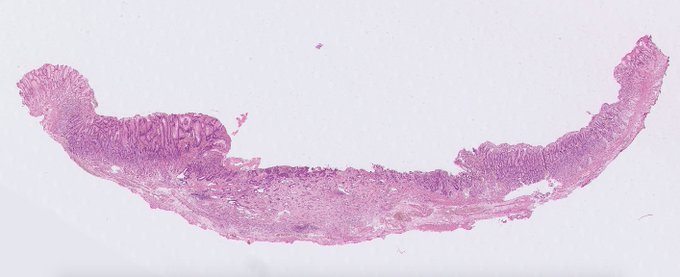
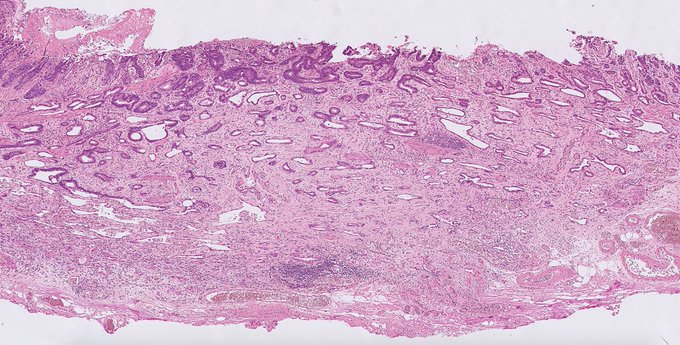
You'd think that... but LN dissection is done by a team of surgical fellows so most work is out of hand. After fixation the entire mucosa can be reliably evaluated (see picture two small cancers) and long strips are embedded in megablocks to assess proximal extent of atrophy.

8
17
54
Exciting PhD in my lab
@UCLCancer
investigating the dynamics of immune evasion in cancer.
The ideal candidate combines experience in evolutionary cancer biology and relevant laboratory techniques w exposure to computational genetics.
Thankful for RT
1
34
50
MMR negative normal intestinal crypt focus in MLH1 Lynch (clockwise: MLH1, PMS2, MSH2, MSH6).
#GIpath
4
14
51
Exciting PhD in my lab
@UCLCancer
w
@BenWerner
@QMBCI
through the
@CRUKCOLcentre
@TheCrick
investigating immune evasion in cancer.
Looking for PhD candidates w background in theoretical genetics and stochastic modelling.
Job ad here: . Thankful for RT
2
46
49
When you've just called in to say you'll be home on time.
7
5
50
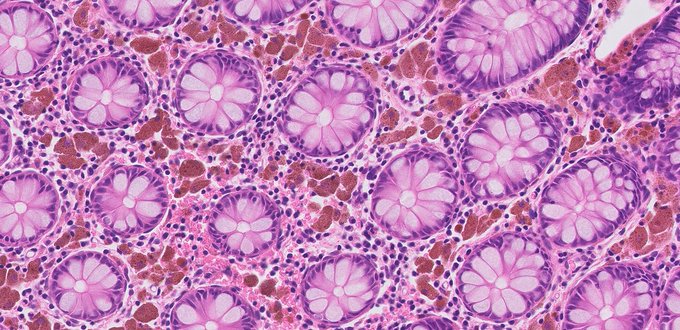
Nice example of muciphages, here in association with a hyperplastic polyp. Notice the raisinoid nuclei.
Muciphages are found in up to 40% of normal rectal biopsies, where this hyperplastic polyp was also found.
-
4
18
48
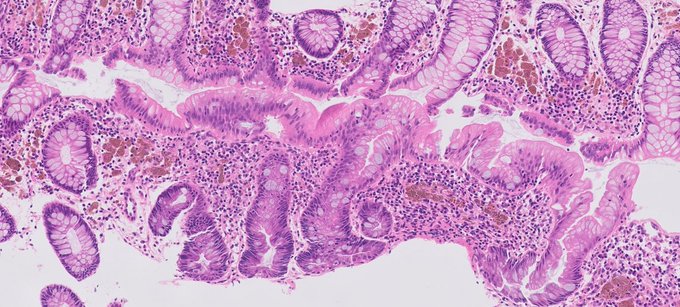
Continuing on from yesterday's theme, this is a melanosis coli with a sessile serrated adenoma/lesion.
Often in patients w melanosis coli, on endoscopy the SSA/Ls stand out from the background mucosa because of their shiny mucinous cap.
Look at all those bloated macrophages!
3
18
47
Well played all, this is solitary rectal ulcer syndrome (SRUS)
📍name is a misnomer
📍benign condition due to straining/prolapse
📍treated conservatively, surgery last resort
📍rare condition, prolapse in comb w gland misplacement can mimic invasive disease - don't be fooled!
1
2
43
Submucosal infiltration in ESD specimens often provokes extensive fraying of the muscularis mucosae.
Measure infiltration depth from deepest fibre MM, true volume of disease often larger than raw depth indicates.
Here 620 micron, T1b SM2, 15% risk LNs
2
16
44
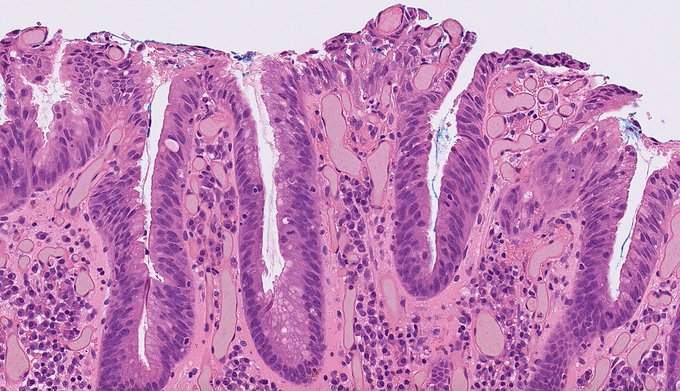
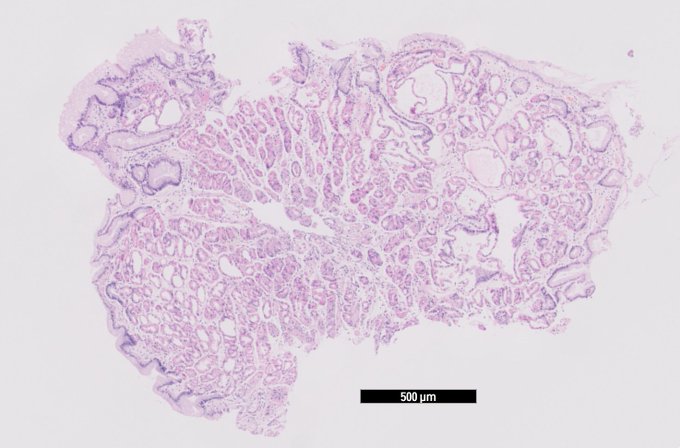
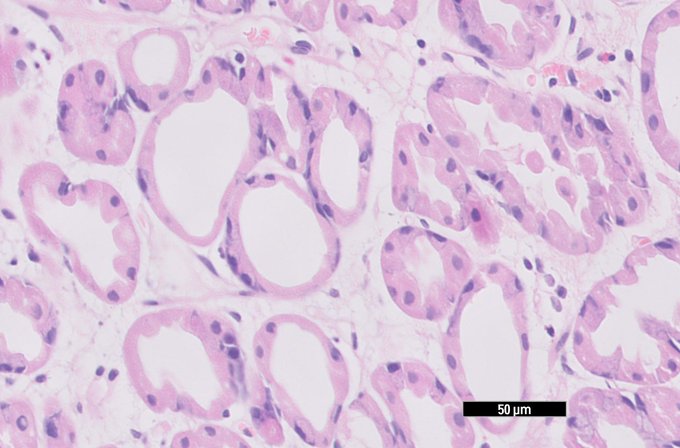
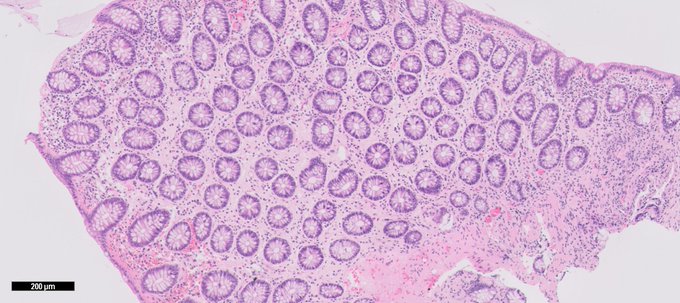
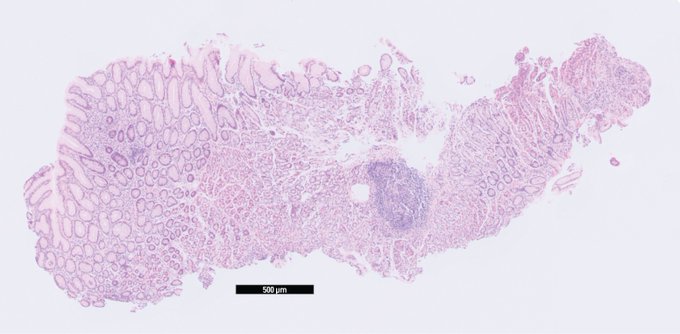
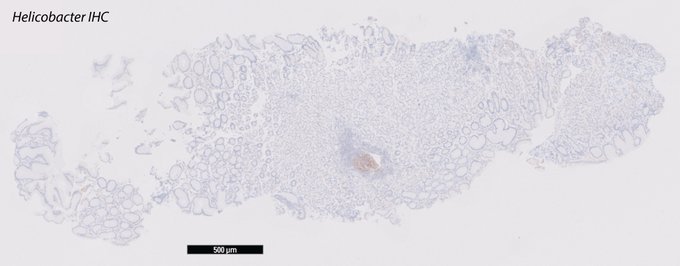
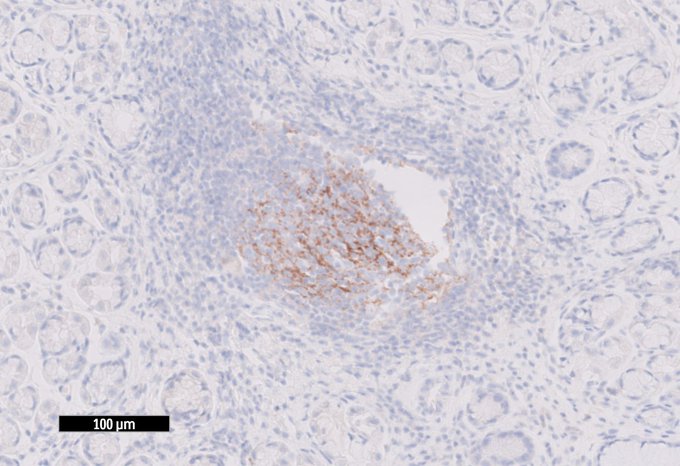
Helicobacter is a choosy organism - it will not hang out w intestinal metaplasia!
Helicobacter reveals abundant organisms on native foveolar epithelium, but none in neighbouring metaplastic glands.
This escape strategy ultimately drives progression to gastric cancer.
#GIpath

2
6
43
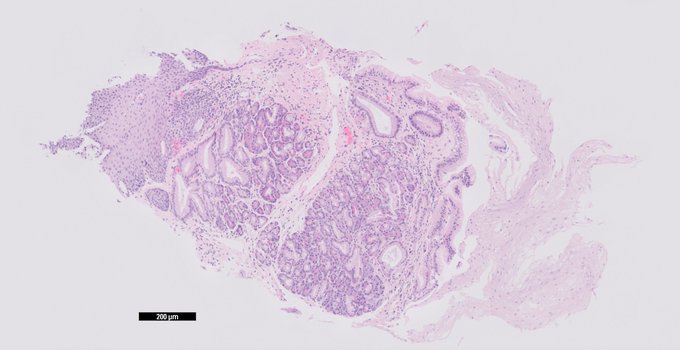
Fun Saturday evening distraction
Small mucosal lesion 3mm sigmoid incidentally detected, EMA and S100 shown
#GIpath
4
11
41
Can we agree to stop using the term Masson tumor?
It is pointlessly confusing for anyone outside of surgical pathology.
#pathology
10
5
40
Your colleagues will remember your kindness and leadership years after this horrible pandemic has passed.
#keepstrong
#oneteam
0
6
42
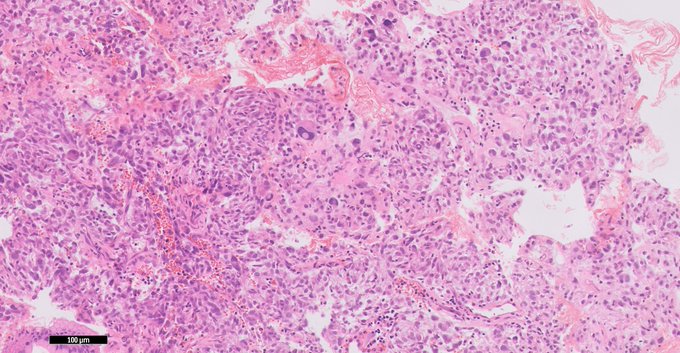
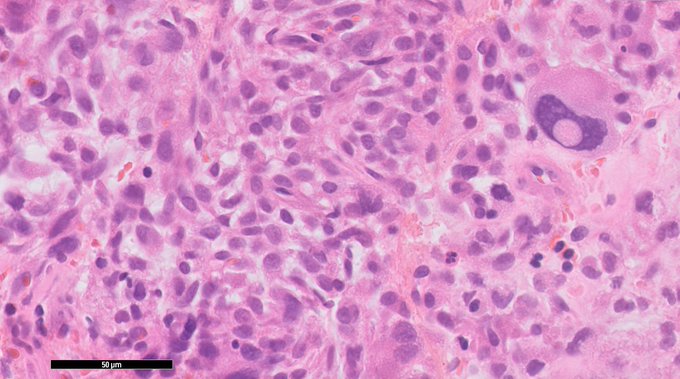
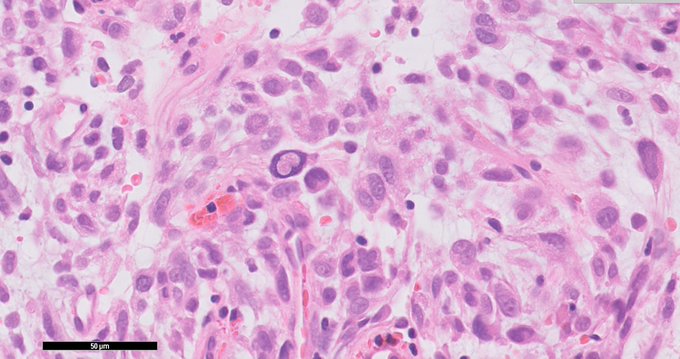
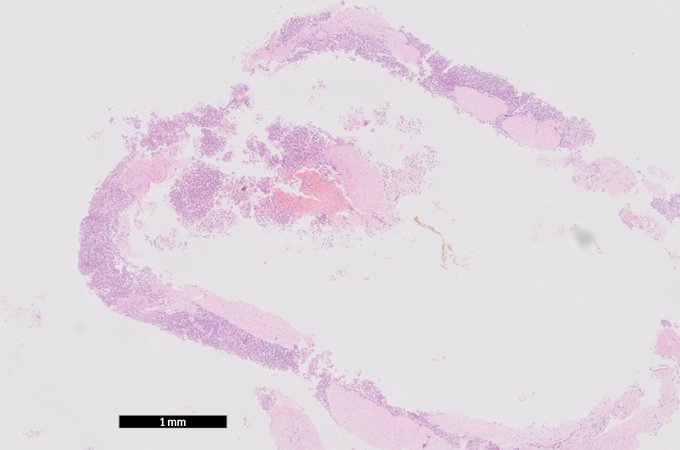
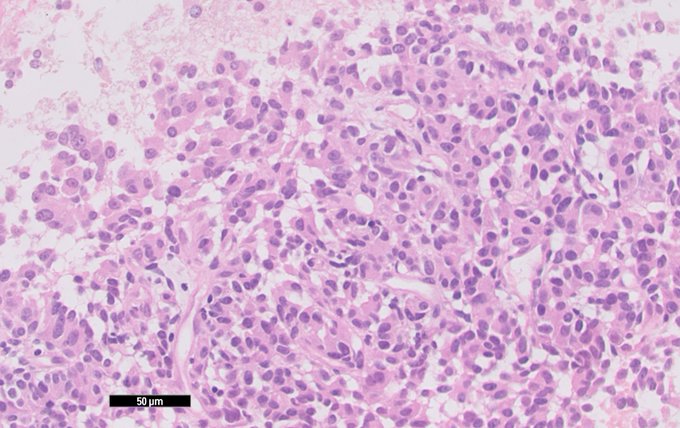
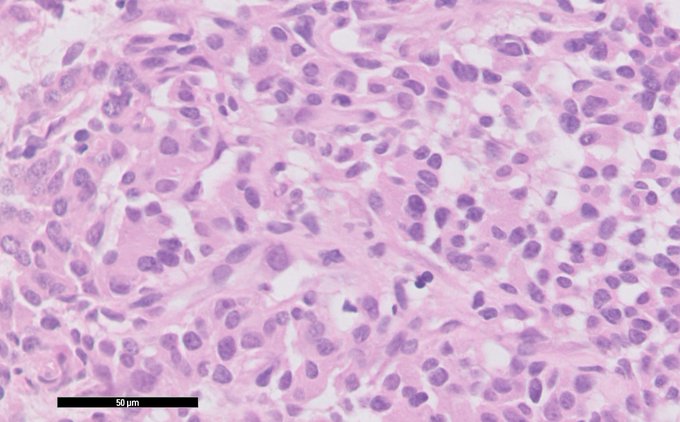
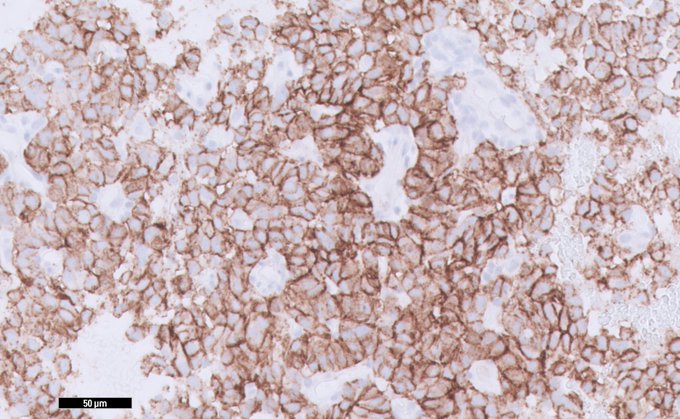
44y HIV+ M, D1 duodenal mass (5x4x4 cm), G3 lesion, lipoblasts lower grade areas, MDM2+ > dediff liposarc w focal rhabdo diff
@DraEosina
3
27
38
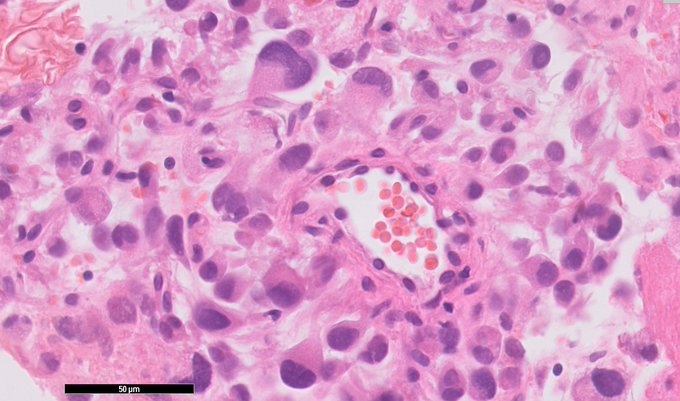
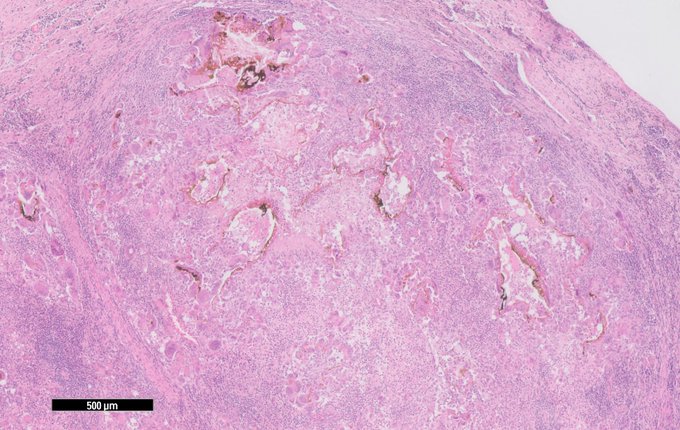
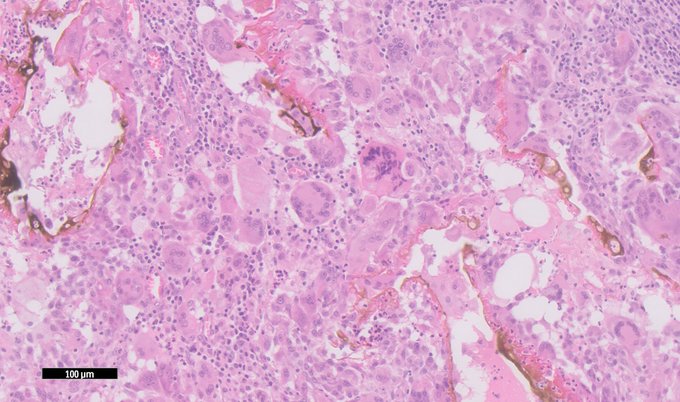
GI pathology hive mind
Looking for a name for this (benign) subcapsular liver lesion. Aggregates of giant cells, and macrophages on their way to becoming giant cells, ingesting bile. No atypia.
Is this due to trauma? Or an involuting duct hamartoma? No Tx/bx history
16
13
36

0
0
34
Many IBD biopsies tonight, which - of course - continues despite the pandemic.
This crypt is feeling the squeeze!
0
1
35
Pathologists:
Today I saw Walthard rests in a diapraghm biopsy and recently I saw them in a routine appendectomy.
Can someone explain their histogenesis to me, and how they end up in these weird locations? Do we know?
#pathology
#pathologists
3
10
34
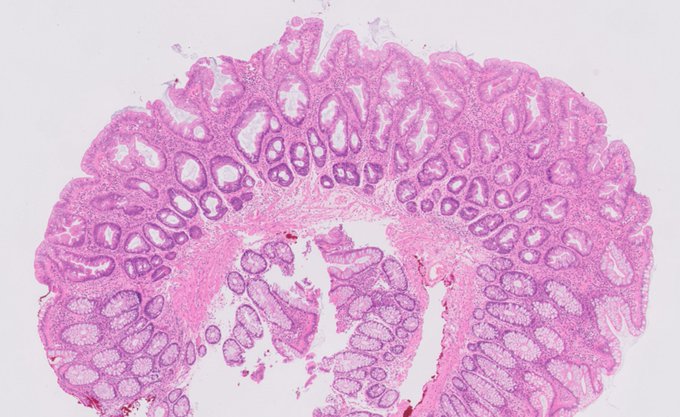
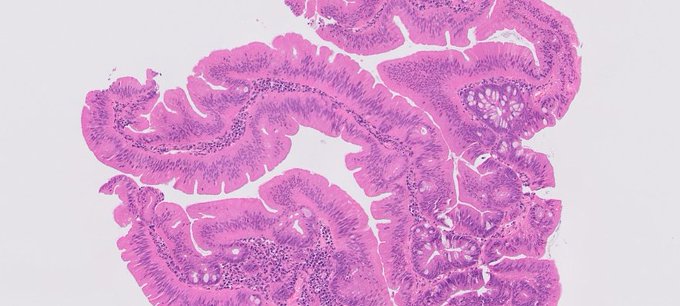
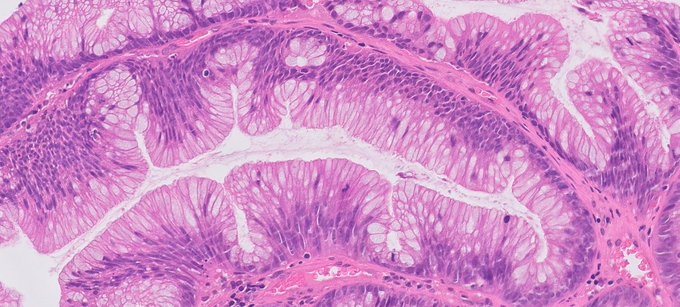
Ectopic crypts galore!!
Biopsies of an anemone-like polyp at the anorectal junction showing all the classic signs for a traditional serrated adenoma.
Every ectopic crypt focus is a cauldron of evolution!
-
-
2
12
35


We present our next paper ‘Histopathologist Features Predictive of Concordance at Expert Level Amongst a Large Sample of Pathologists Diagnosing Barrett’s Dysplasia’ with
@MedRxiv
That’s quite a mouthful so this is a short explainer
Thread 1/8

5
12
34
Khoresh-e fesenjan
Persian walnut, pomegranate and chicken stew for Sunday lunch
Been wanting to make since pre-lockdown days



7
0
33
Lots of easy going stuff tonight.
Straightforward fundic gland polyp, cystically dilated glands with PPI effect.
0
3
33

Finally back to live meetings!
Annual UCL Cancer Institute conference, so much great science.
@uclcancer

1
0
32
@frankie_shea
@Dr_Ellie
@KirstieMAllsopp
These are all outpatient clinics.
They're deserted because all elective care has been suspended and staff have been redeployed to the wards.
To care for Covid patients.
2
0
31
There is no shortcut to experience

That one senior pathologist in the department nailing it mostly by morphology
#pathology
#pathtwitter
#ihcpath
15
116
836
4
0
29
Just a nice crosscut serrated gland to go w coffee after dinner
2
5
30
Here is a small strip of reactive epithelium at a squamocolumnar junction trying really hard
2
5
28
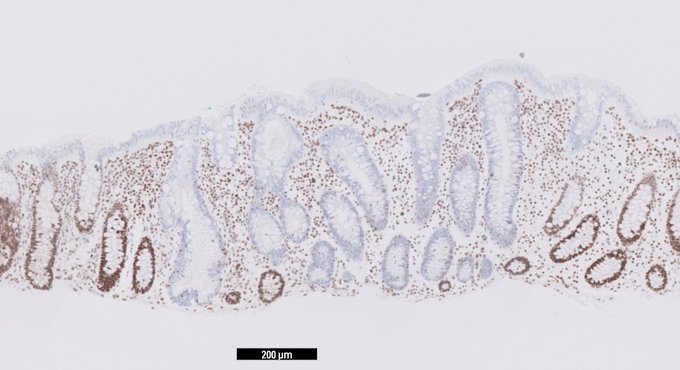
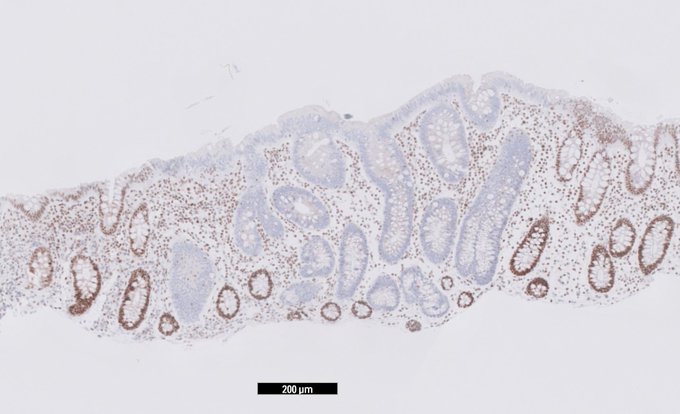
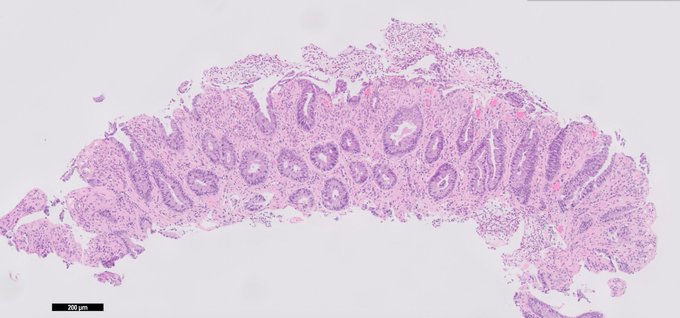
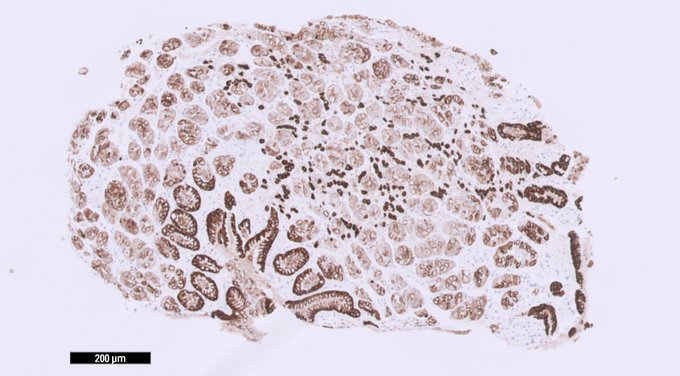
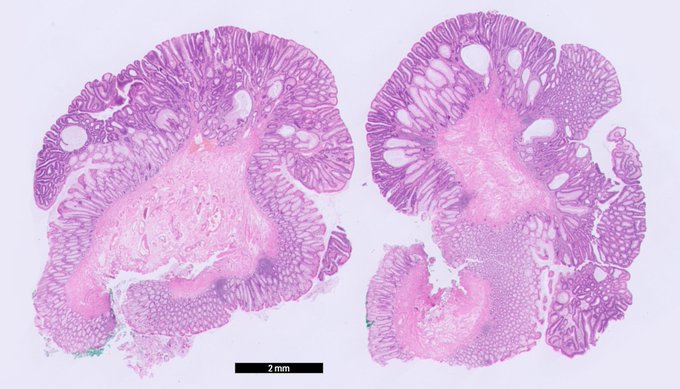
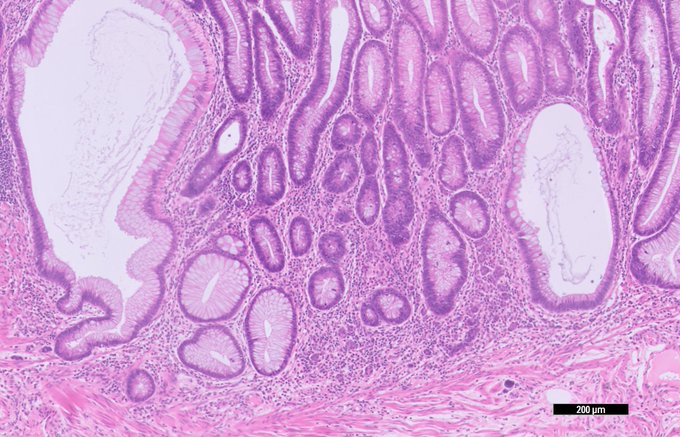
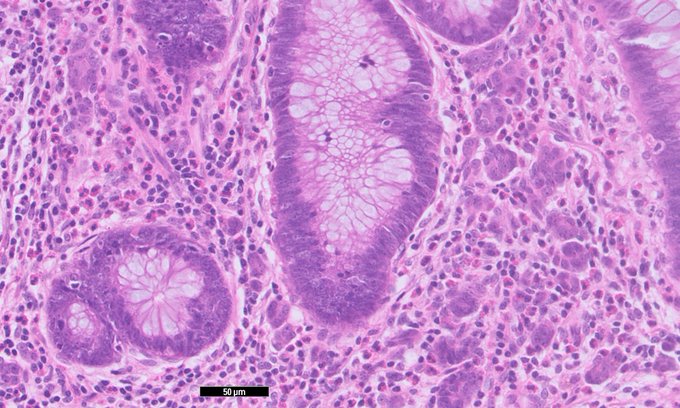
Young individual previous GBM now oligopolyposis. One of the polyps and MSH6 in overview, adenoma and normal crypts (last picture). Nb. the other MMRs are normal/retained.
What cancer-prone condition does the patient have?
#gipath
@RunjanChetty
@DraEosina
@Jmisdraji
@Aiims1742
2
16
29
@DrBMcGinn
All the time, especially cancer reports
Resection, site, approach:
- type, size, grade
- stage
- nodes
- margins
- anything else, molecular etc
TNM
I also use 'strategic bolding and underscoring' in the microscopy section. It's the way to a surgeon's heart, believe you me!
4
0
26
Paneth cell metaplasia in a cloacogenic polyp/SRUS
(crypt stem cells, like most adult stem cells, have a limited repertoire of tissue response patterns)
0
4
28
The longer I practice surgical pathology, the more I genuinely miss patient contact.
8
2
26
@hugo_uchima
@ariella8
@DraEosina
@nucleololailo
@RunjanChetty
@Teclis82
@brian_odum
@CArnold_GI
@DrMarkOng
@Mvgs1706
@ggchen_MD
@vi_monappa
@drtimbracey
@SingJamieD
@DoraGIPath
This is an example
@ariella8
of short segment/ultrashort coeliac disease limited to the duodenal bulb from today's catch. The D1 biopsies are diagnostic (right side o/t strip) whilst the D2 biopsies (left side o/t strip) are unaffected. Relatively novel entity, PMID: 26836585
1
8
27
Naughty bit in an otherwise uncomplicated SSL/SSA, MLH1 intact.
Is this what my dear friend Christophe Rosty described as 'sessile TSA arising from SSA/SSL'? (Fig 3b in )

2
5
26
Just ran into
@BBCSteveR
in Central London. Meant to congratulate on his team’s award, absolute gold standard journalism.
1
0
26
@GIJamesMD
@Vik_deshpandeMD
@ariella8
@DraEosina
@DrMarkOng
@CArnold_GI
@Mvgs1706
@drtimbracey
@SumantaDas_7
I'd sign this out as serrated epithelial change and leave a comment referring to studies below commenting on its possible association with metachronous neoplasia (which in this patient appears to have materialised).
3
5
26
I am of that age where I was too young for the first Top Gun and too old for the sequel.
7
1
26
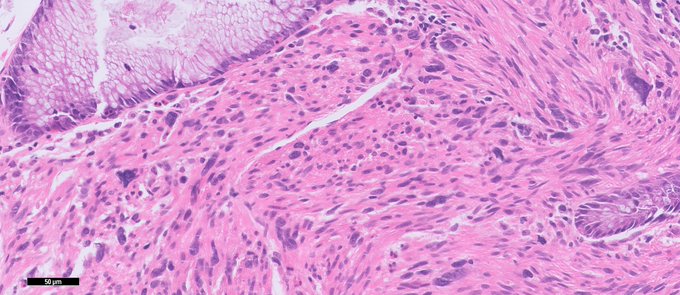
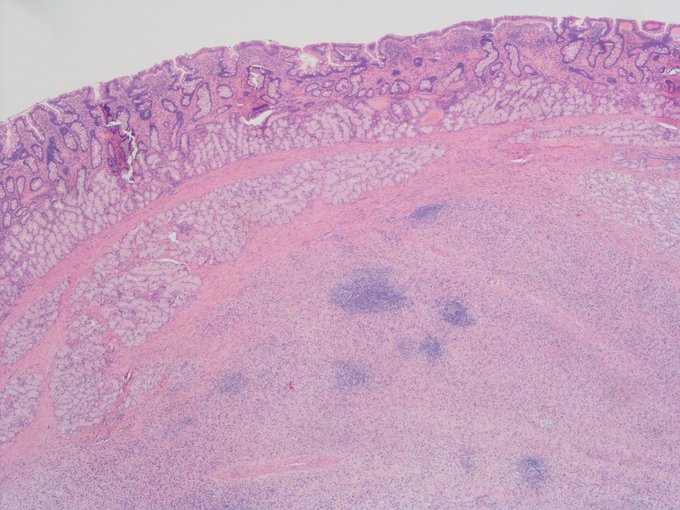
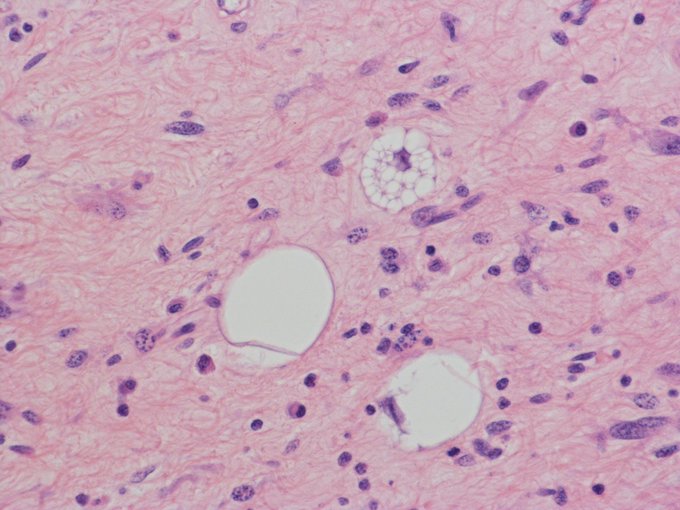
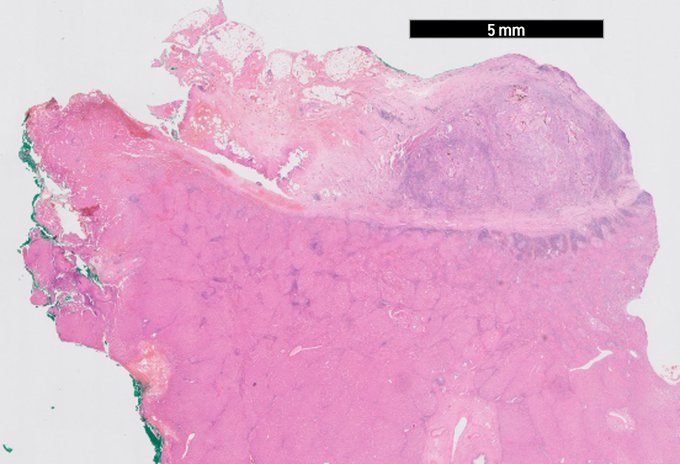
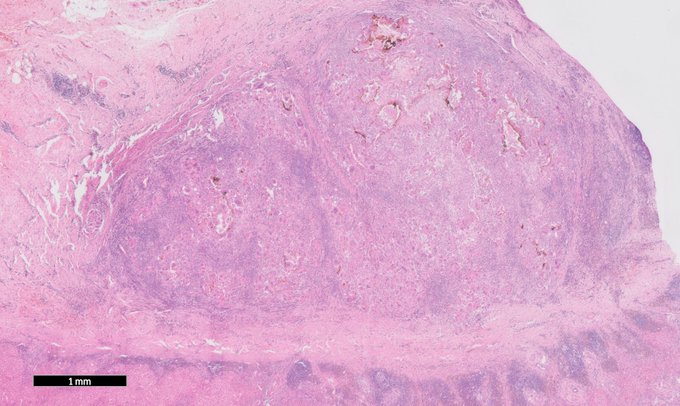
This is NOT IBD or pseudomembranous colitis
Don't believe me? Below are the biopsies of the surrounding bowel, utterly unremarkable
What is this? Remember, these are biopsies of a palpable *mass*
5
3
24
Helicobacter antigen in germinal centres, but no actual viable organisms. Patient recently treated
as reported by
@emma_furth
and others in
@amjsurgpathol
PMID: 32657781
link:
1
6
25
Londoners
I'd also really like to hang out in the local
But I was on my way back home from the hospital. Late, cuz a third of my consultant colleagues is self-isolating w Covid-19.
Which part of 'do not visit pubs, clubs, or theatres' do you not understand?
0
12
24

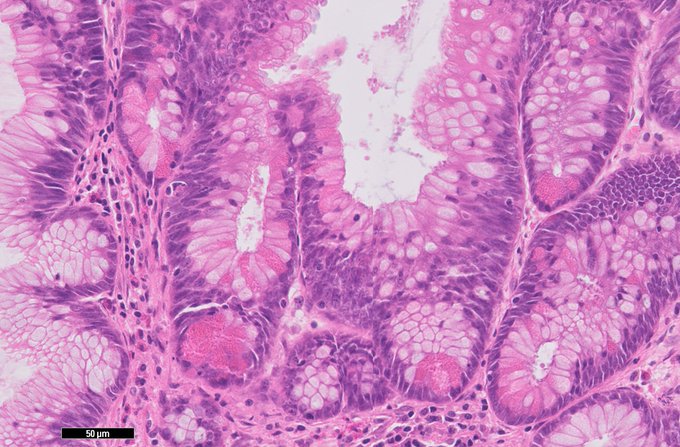
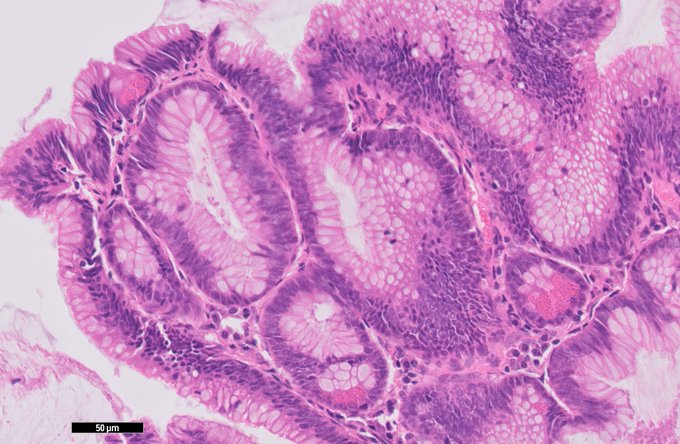
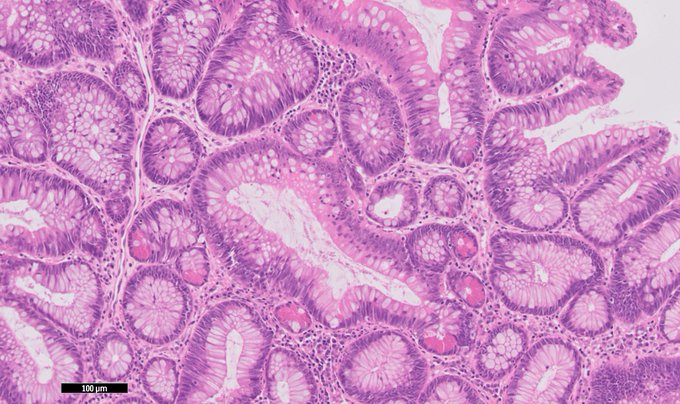
Recent work with
@NadiaNasreddin
@ViktorKoelzer
and
@leedham_simon
on diagnostic reproducibility of colitis-associated dysplasia subtypes.
@ModernPathology
1
9
21
You are looking for a PhD program in cancer immunology and DNA repair?
Apply for a
@CRUKresearch
funded PhD programme with Sarah Martin
@QMBCI
and myself
@uclcancer
. Exciting science, fun teams, impact for patients. ✍️🧬🔬

Are you interested in doing a
#PhD
in
#cancerresearch
? Do you want to develop new
#biotherapeutics
? 🧑🔬👩🔬🧪🧬
Applications for our fully funded 4-year PhD programme are open now!
0
21
25
1
10
22
Love these Paneth cell-rich adenomas clearly outlining the stem cell compartment.
Adenomas are a caricature of normal crypts ().
1
1
22
GI path hive mind
What is the rational approach to lymph node staging in pats with synchronous colon tumours? Say 6 out of 30 nodes are involved. Report one joint N status for both tumours? 3 positive nodes each?
Obvi can't tell origin...
How do you approach this situation?
11
8
21
How can completely random memories from one's childhood stand out so much? Why did exactly those memory traces stick when so many others have gone?
3
0
22
@SadiqKhan
@willnorman
@willnorman
Easy, change traffic laws to modern Dutch standard by default assuming blame lies w driver in case of collision. This will give cyclists an invisible legal safety bubble, reducing accidents and road deaths, and ultimately bringing more folks on the road.
1
2
21
In other news, our youngest took hist first steps today. Go alpha neurons!!
1
0
21
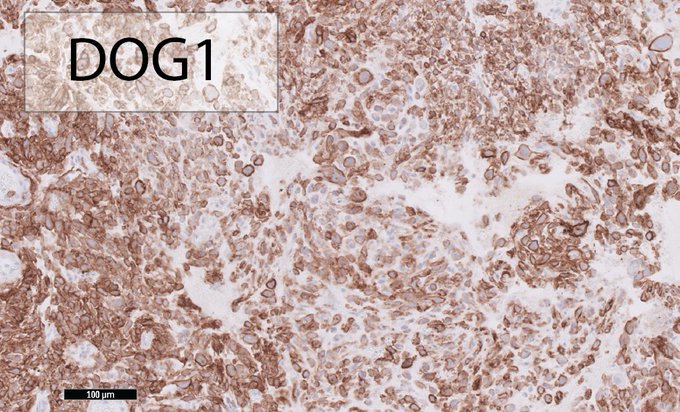
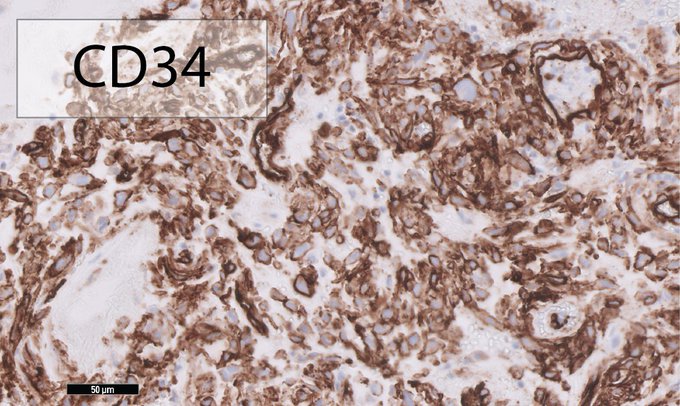
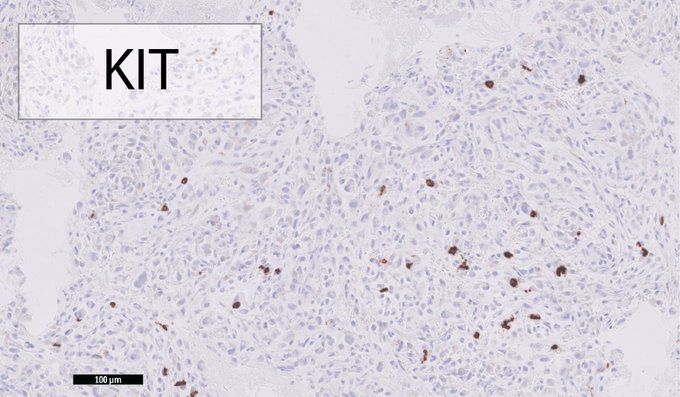
Epithelioid GIST.
This case labelled strongly for DOG1 and was negative for KIT. This occurs in a minority of GISTs (<5%), in particular PDGFRa mutated cases. This lesion tested positive for this mutation.
Keratins and melanoma markers all negative.
PMID: 19606013, 24111893

0
2
18
Congratulations to Dr Hadiza Bawa Garba on joining the GMC Specialist Register as a fully trained consultant paediatrician.
0
0
19