

Jan Hansel
@VirtueOfNothing
Followers
4,012
Following
2,813
Media
2,133
Statuses
24,826
ICM & Anaesthetics SpR North West | NIHR Academic Clinical Fellow @OfficialUoM | ‘The truth is not always beautiful, nor beautiful words the truth.' –Lao Tzu
Manchester, England
Joined November 2009
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
Kendrick
• 206146 Tweets
Drake
• 193096 Tweets
Gabigol
• 137345 Tweets
RPWP CONCEPT PHOTO 1
• 119770 Tweets
Euphoria
• 111819 Tweets
#محمد_بن_سلمان
• 68566 Tweets
#SixTONES結成9周年
• 28084 Tweets
On a Tuesday
• 27465 Tweets
音色発売
• 25051 Tweets
Senna
• 22723 Tweets
#Happy9thAnnivST
• 19330 Tweets
#いつもありがとうSixTONES
• 18647 Tweets
Thor
• 18466 Tweets
Viper
• 17657 Tweets
RIGHT NOW MV TEASER
• 16956 Tweets
ワルプルギス
• 16560 Tweets
Barron
• 16242 Tweets
大慶くん
• 15383 Tweets
サブスク解禁
• 13489 Tweets
かのんちゃん
• 11986 Tweets




















Pinned Tweet

It’s World Antimicrobial Awareness Week 🦠
Find out how research on therapeutic drug monitoring in critically ill patients with severe respiratory infections can help us understand and curb antimicrobial resistance through precision dosing
@MFT_Research
@timwfelton
@DarkNatter

For
#WorldAntimicrobialAwarenessWeek
Dr Jan Hansel discusses the importance of therapeutic drug monitoring (TDM) in limiting the development of antimicrobial (antibiotic) resistance, and the new TDM-TIME study he is leading at
@MFTnhs
🧪.
🔗 Read more 👇

0
5
12
17
3
22
‘Hiya is this gastro on-call? I’m Rob from Prestwich, 54, bit of a boozer. CGV last 24 hrs, melaena 2 days. Glasgow-Blatchford 8, but that’s without an Hb cause I’m calling from home to self-refer. Am I alright to pop in for a quick OGD +/- transfusion later today? Ta.’

"One of things we've put forward.. self referrals so individuals dont have to go to a dr in order to get referred to specialist help.. if youve got internal bleeding & you just need a test there ought to be a way that doesn't involve going to see a GP"
Keir Starmer on
#BBCLauraK
1K
176
696
43
271
2K
‘Tell me you work in the NHS without telling me you work in the NHS’

37
70
2K
Mate getting the NHS PCs to startup and let you login in less than two minutes would be a start. What are you smoking
@RishiSunak
?

87
242
2K
So we heard today at the select committee debate
@gmcuk
will be charging £221 per annum for PA/AA registration.
Why do I as a doctor have to pay £433?
I would much rather pay £221 as well, and come to think of it, I just might cancel my direct debit right now. 🙂
45
229
1K
A young woman died as a result of a barndoor pulmonary embolism presentation missed on two occasions, under the impression that she had been seen by a GP.
This is not the standard we should comfortably walk past.

88
276
918
Literally saw a porter fight off a rogue pigeon that made its way into the hospital through a window while transferring a vented patient. He grabbed it by the neck and threw it back out. 😳 Peak NHS. Highlight of my medical career thus far, hands down.
17
42
777
👀

I’d like to thank everyone that contributed to the survey. Important issues are being raised (and I don’t love that it’s the MoS trust me).
8
29
120
36
128
595
£10,000 a day for a Kwasi Kwarteng.
Versus £14.09 per hour for a fully qualified doctor.
Let that sink in.
That’s a factor of 89.
And
@SteveBarclay
is calling on
@BMA_JuniorDocs
to ‘check our conscience’.

🚨MPs FOR HIRE: a Led By Donkeys undercover investigation🚨
Watch the trailer…
4K
37K
93K
4
191
588
1/ We just published our full
@Cochrane_ACE
systematic review and meta-analysis of videolaryngoscopy versus direct laryngoscopy for adults undergoing tracheal intubation.
The full review is here, but first - some of our key takeaways 👇
25
229
551
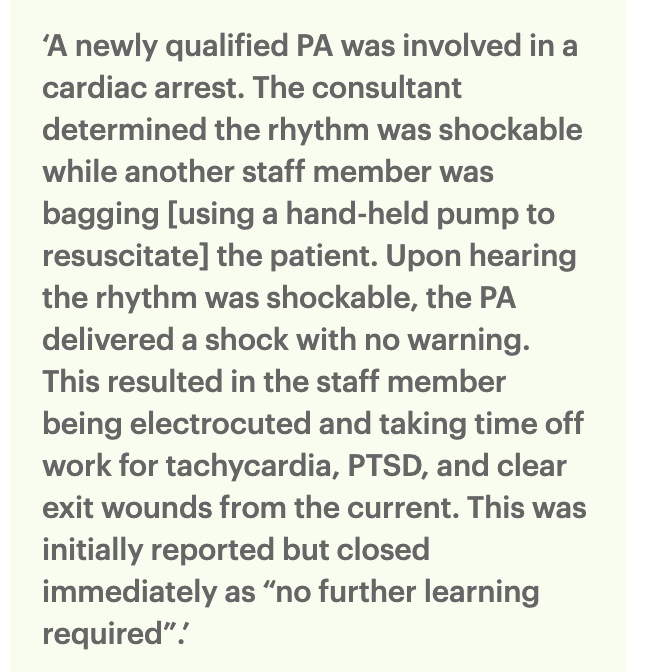
What THE HELL did I just read 😳
Was nobody in the entire chain of numbskulls able to exercise a MODICUM of common sense?
This is another example of a system broken by Kafkaesque rules and blind adherence to ‘policy’.
What a disgrace. I hope they sort it soon.

A few days ago I found out my 86yr old mum with dementia had had a fall & been admitted to hospital
I didn’t know which hospital so had to cold call the ones in the area
No luck
I thought this can’t be so called them all again
Fortunately I got a different receptionist at one….
602
1K
4K
24
45
496
#oneteam
Yet one group of NHS workers seems to be missing. Can’t quite put my finger on it.


103
39
476
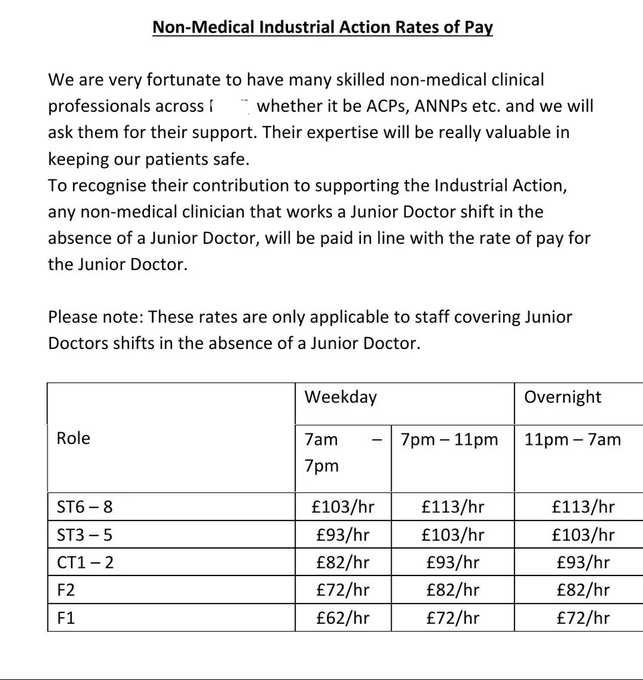
PAs have a narrower skillset than junior doctors, yet somehow get paid twice as much for the same shifts.
“But Jan it’s dehumanising to compare anything to anything.”
Make it make sense please. This is just an insulting constellation of managerial decisions.

How is this acceptable
@BucksHealthcare
?
Doctors are NOT worth half a Physician Associate.
FY1s, this is how they value you. Look how they value your replacements.
STRIKE.

63
340
1K
7
71
449
A prefrontal cortex

Dear men, what is preventing you from doing this?
40K
12K
139K
13
24
431
The BBC mislabelling AAs as anaesthetists. Thing is, ‘anaesthetist’, unlike doctor or surgeon, is not a protected title.
What’s even funnier? The GMC will make ‘Anaesthesia Associate’ a protected title.
You couldn’t make this up.

11
60
411
Nothing quite like an NHS manager gaslighting doctors and siding with the serial killer, allowing further baby deaths.
Tony Chambers was appointed interim CEO at
@qvh
earlier this year. When will he be suspended undergoing investigation on grounds of patient safety?

EXCLUSIVE: The doctor who helped catch Britain’s worst baby killer.
Dr Ravi Jayaram spent two years pleading with hospital managers to investigate Lucy Letby.
Instead, they made him apologise and attend mediation with her.
1K
11K
34K
12
91
384

I really find it quite adorable when middle management (what's an operations director?) come to speak at us on AMU to mAkE uS aWaRe that the NHS is struggling and ambulances are waiting and ED is full and we need to also discharge some patients.
Me:
'Plan: - Repeat FBC/U&E/CRP'
13
13
364
I urge all doctor colleagues to complain to the GMC regarding the 7-digit number.
The form (Word or PDF) can be found here:
We need to make our voices heard and let them know that we will not stand for this.
It also demands a top-level response
@TheBMA

How do I raise my comment or complaint?
How to raise a complaint to us about our work
www.gmc-uk.org
The entirety of the upper echelons of medical governance frameworks in the UK are currently *that* Spiderman meme…
Honestly, is this a joke?
And the 7-digit number as a cherry on top…
One word for you,
@gmcuk
: No.

8
33
128
26
129
338
As a clinician I find it extremely unrewarding working in a system that is in near-constant triage mode.
The moral injury of knowing what the standard of care looks like, and not being able to deliver it because of shockingly poor resources, is real.
7
78
339
So this is great.
Is it a doctor’s QI job though? No.
This is the sort of thing an NHS manager should be doing. Speak to clinical teams and ask what about the ergonomics (or lack thereof) is frustrating.
Then go back to the office, make it happen and measure the impact.

In F2 I needed a QIP, and instead of the usual VTE crap I decided to do something useful. The state of our doctors’ offices had always pissed me off and so I went about improving things, new chairs, more computers, more phones etc. Small things but made a big difference! 😎😎😎




41
40
655
23
35
329
Pray tell
@ELHT_NHS
what non-medical clinical professionals work at ST6-8 level to cover at BMA rates? I expect some concrete and specific examples.
@Dr_Done_
@Xeon4f145d96s1
@BMA_James_Steen
37
60
317
I will just leave this table here to do the talking. The
@RCPhysicians
leadership has attempted to mislead its Fellows at the
#RCPEGM
.
🔗

14
113
298
A bit conflicted about this. How broken is an educational system that does not simply make arrangements to defer an exam in case of illness? I appreciate there is likely nuance here. But what does this signal to other medical students ...
21
20
294
Because ARCP season is near. And we all love a good audit.


7
15
294
Not to draw comparisons, but when I moved to Iceland in 2015 the doctors had just secured a collective agreement with the government, where all grades got more than a 20% pay increase (minimum!) compared to the previous financial year.
It. Is. Doable.

@_jaytalbott_
@Dr_XYZ
@VirtueOfNothing
@Ssj3Sa
@_VivekTrivedi
Politically impossible. Imagine effect on other workers seeing what they perceive as (and in reality is) a high earning group getting 35% rise.
13
0
1
6
30
266

I really hope this was a misprint or some other error, but ‘management of AAAs’ axed via the NHS?
‘Hey John, so you have this 3 inch ticking timebomb in your belly that we could operate on and save your life, but now you will die within the year. Good luck.’
What am I missing?

30
18
238
And another one. The embodiment of 'junior doctor' infantilisation in the UK. It is rampant and quite frankly toxic. I for one am happy to call it out.
Out of interest, what do you ignorami define as 'the junior doctor'? The ST8 with a combined 14 years experience?

@DrHuw
@VirtueOfNothing
@telswood
@Matt_L_Nash
Why wouldn’t an experienced ANP be able to be above the skill of the junior doctor, maybe the consultant is busy.
8
0
1
8
34
227
Behold… The ‘I could teach my mum how to intubate a neonate’ argument in favour of taskification. 👏 Right after equating it to putting a cannula in. Couldn’t make this up. 🤌
14
23
227

Get in the bin. ‘Anaesthetist associates’
First you need to learn to get their titles right. Amateur hour.
And to think the public or the profession should trust you lot to ensure patient safety?
Get serious.
Sincerely,
An actual anaesthetist (in training)

On behalf of Professor Sir Sam Everington, we share his thoughts on the process towards the regulation of physician and anaesthetist associates
49
8
37
4
27
220
Having just moved prior to changeover, wanted to explore the area a bit and somehow made this happen accidentally 😳 what are the odds…

7
2
219
A very positive dichotomous outcome 🤓





63
0
215
This ICU nurse chose ‘violence’ as her mode of postop PEEP weaning.

31
15
213
This needs to be vetoed by the profession. Hard.
Out now: our self-assessment tool supporting the career progression from Advanced Clinical Practice to Consultant Practice! Track your development as an aspiring or consultant practitioner 👉

88
117
276
9
16
200
Not to be a snob, but does BMJ Open even proof read submissions anymore? This is barely English. The peer review process was clearly sloppy as well. As for the ‘science’ … well. Some wild conclusions here.



25
28
190
This ... is insane. That nurse needs to be fired.
Actually, I would argue that this needs naming and shaming. Such behaviour should not be tolerated from anyone.
Fucking power trips these people are sometimes on ...

Holy fuck. The NHS keeps sinking to a new low day by day.


135
209
927
16
18
178
For anyone following the discussion, a few wise insights from Prof Cook.
We seem to have reached a farsical point in the conversation where it is impossible for a group to acknowledge that a high-risk & high-complexity procedure is best performed by experienced medics.

@thatsnotmine125
@VirtueOfNothing
@telswood
@Matt_L_Nash
This does seem a bizarre conversation
Intubation of the critically ill adult is rife with risk & complications. Harm is common.
Intubation of the neonate (especially when critically ill) is a league up in failure, delay & complications. Harm is intrinsically less easy to…
11
52
316
9
32
176
This to me reads like the straw that should break the camels back, once and for all.
I note the hearings (listed on the doctor's registration) are no longer available on
@gmcuk
website. These should be made openly available again, immediately.



⚠️ For those working with PAs
MPTS case published 2017 where a ST3 Junior Doctor was suspended for failure to adequately supervise a physician assistant’.
The PA was known as ‘Dr G’.
There may have been other issues too - irrelevant. Read the following:

90
282
752
8
51
174
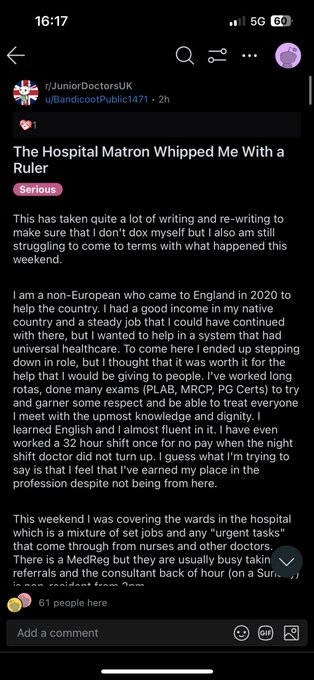
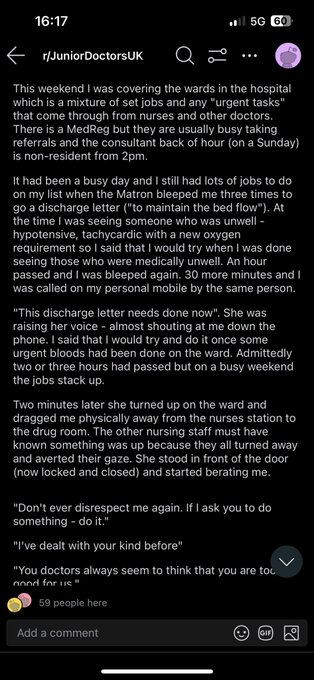
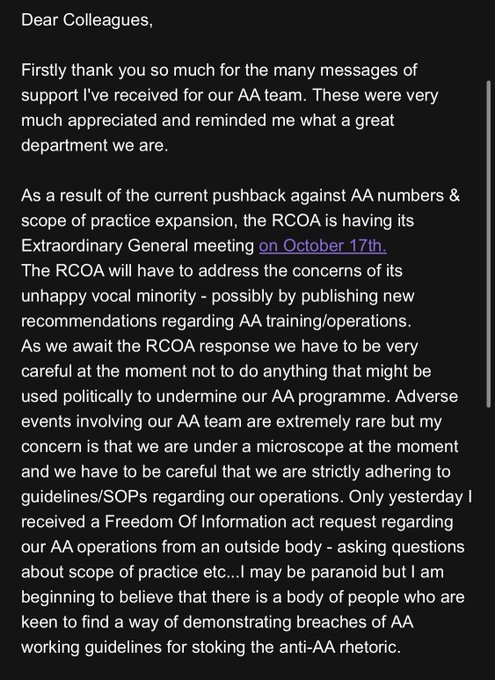
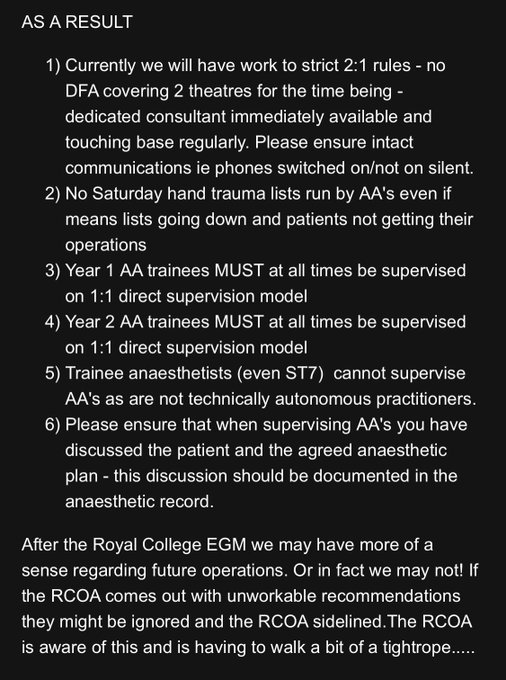
Surprised? Hardly.
This is the equivalent of “fire up the paper shredder” if I’ve ever seen one. Astonishing that an e-mail like this would be openly circulated among a group of consultants.
This is worthy of national news. The public need to know what is happening.
Now, I get lots of DMs
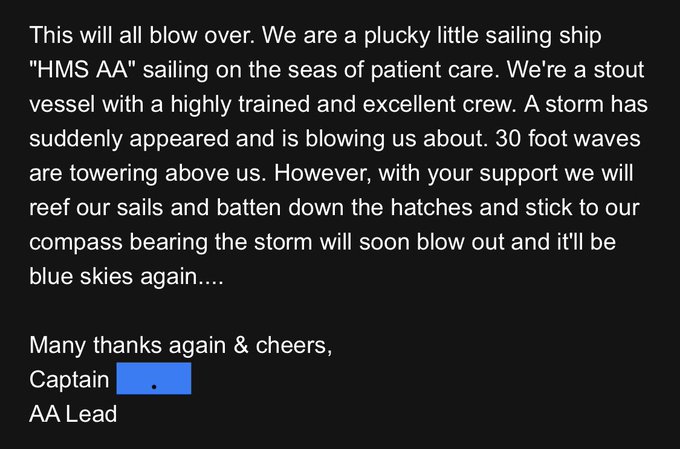
But this has to be in the TOP 5 WORST❗️
‘Unhappy vocal minority’ - how dare you raise concerns?
‘We need to be careful, but only while we’re under the microscope’
Storm analogy again when in fact a tsunami is coming 🫠
@SheffieldHosp
@MajorKirsten1
?
153
187
629
8
36
172
With 3250 PAs currently working in the UK, these data by
@Telegraph
suggest that at least 15% (likely more) have no relevant background qualification.
Degrees such as homeopathy, management and English literature have been accepted.

6
80
172
Hive mind, can you please help? Delivering a tutorial on approaching the deteriorating inpatient out of hours as a junior on-call.
This is what I’ve got so far. 🤔 Further thoughts? NB small group, discussion-based.
47
5
171
AV fistulas should be done by vascular surgeons. Or vascular surgeons in training.
This shouldn’t be a controversial take. Yet…

@scrivvyfloor
@pcricoarytenoid
@ABarotchi1
Afraid an AV fistula is are far too important such that you have to get them right. Dialysis patient's life depends on them working and cannot waste access.
6
0
9
5
21
165
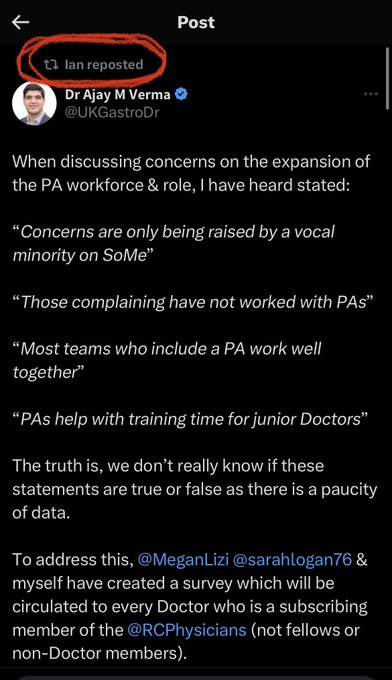
Interesting to note that the CEO of the Royal College of Physicians is a nurse.
Only one month ago, Dr Ian Bullock (RCP CEO) (Nurse)
@Bullock1Ian
retweeted this
A call for responses to assess concerns of doctors about physician assistants
To ‘be better informed prior to voting on proposed motions.’
@RCPhysicians
then obscures the data at
#RCPEGM

11
31
121
14
27
168

Good to know that my practice can stay the same.
One of my favourites on ALS special circs stations is appending the phrase “… will do f*** all.” to the often recited “10 ml of 10% calcium gluconate…”

13
26
166
Look at this badboy just casually chilling next to some bins unattended. Rare to see one in the wild like that 👀

20
6
165
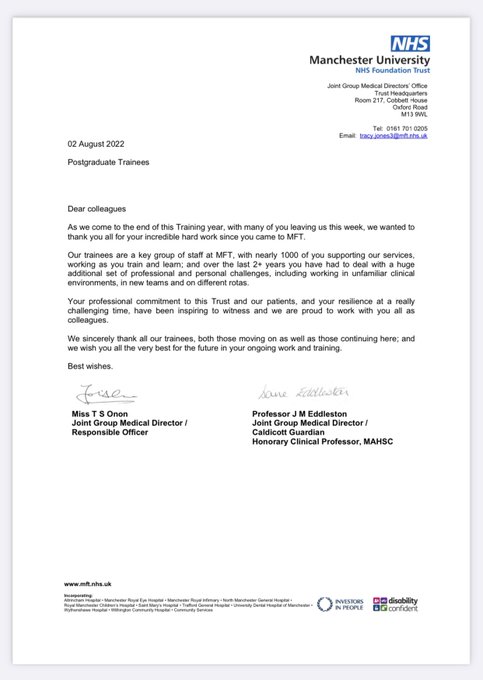
Amidst a lot of negativity on Twitter—and
#MedTwitter
in particular—this sendoff by
@MFTnhs
prior to changeover was a lovely little gem. Thank you.
10
22
164
Funny how in cardiac theatres every single dorsum of the left hand seems to magically take a 14G cannula without issue all of a sudden

15
9
162
That pesky critical desaturation won’t stop this task fixated anaesthetic team from putting a 17G venflon in the wrist!

13
23
162
@Dr_Done_
This will all very soon be landing on the GMC's doorstep.
Just imagine, scaled up nationwide, the additional staffing requirements for the rigorous FTP procedures ...
6
12
160
There we go, an unregistered anon ?PA is weaponising GMC guidance against me. You couldn’t make this up. 🥲

@VirtueOfNothing
@iDrSunny
I don't take kindly to threats Jan Hansel and please read your own GMC guidelines in relation to social media. Thank you
2
0
3
8
11
159
Just published: The impact of PAs on surgical training
Four domains of key recommendations from
@ASiTofficial





📢 New
#ASiT
Report on Physician Associate Impact on Surgical Training and Patient Care 🏥👩⚕️
🔍 Largest ever ASiT survey: 1,978 doctors across all surgical specialties in the UK.
🤝 Focus: Physician Associates (PAs) impact on surgical training and patient care
📈 73.8% worked…
21
239
435
3
36
153
'The judge ruled that Dr C was in breach of her “duty of care” towards the child and was 60% liable for the incident. The child had stepped on to a pedestrian crossing when the light was green for traffic and was 40% liable.'
What did I just read?! 😳

46
22
147
Anaesthetics ST4 job offers due today ...
2pm: ANRO sends this e-mail to candidates.
Colleague: "My BP has been through the roof since 9am waiting for the result."
Thanks ANRO ...
This does NOTHING to restore any faith in your utter lack of competence.
@RCoANews
, comment?

19
16
150
Gosh, GSTT critical care sounds like a right mess…




5
10
146
I would be keen to hear how patients/NHS service users have been involved in the decision to introduce PAs/AAs.
While the DHSC would love you to believe the horse has bolted, it is not too late to turn this around and set things straight.
Read this article. Write to your MP.

4
72
148
A business case from UCH published March this year on the RCoA website:
Back-of-the-envelope calculation...
2x Consultant Anaesthetist = £277,240
2x AA + 1x Consultant Anaesthetist (2:1) = £287,546
Make it make sense 🙏

24
35
145
An appropriate scope of practice for AAs?
Some hard-hitting statements about the role from senior AAs introducing it to prospective students.
DNACPR conversations, very liberal solo regional lists, misleading introductions, and more.
My view: This needs addressing at the EGM.

'An introduction to the AA role' from Lancaster University.
We have compiled excerpts from three talks by senior AAs. Names and other sources of identifiable information have been removed.
49
94
255
4
20
140
Should the BMA start cracking down on such highly imaginative use of public-facing language?
13
12
143
Entirely irrelevant whether doctors’ fees are used for the AA/PA register or not.
We expect to see an exact breakdown of costs to justify a twofold (or more) difference in fees.
We definitely pay you enough to be transparent.

2/2 While we’ve said we plan to set initial fees for PAs and AAs close to the current fee for the FPA voluntary register, this is subject to change.
PA/AA & doctor fees will differ as we take a range of factors into account when setting fees and align them with the cost of…
34
2
11
2
20
142
And this is the crux of it. In the UK, yes, everyone is deskilling left right and centre.
I’ve been fortunate enough to do a proportion of my early EM training in Iceland, where exposure to these basic procedures (chest drains, paracentesis, LPs, CVCs) was plentiful.
@scrivvyfloor
@dr_lungs
@sh_abbers
@dannyjnwong
@pcricoarytenoid
@ABarotchi1
I'm amazed placing a chest drain isn't within the compass of any medical SHO. What are doctors doing now? Is everyone totally deskilled?
10
0
17
8
23
139
And here it is. The pernicious argument that always seeks to lure doctors into self-defeating submission.
Because we need to pretend that everybody is the most skilled at everything and anyone can do our job, right?
This doctor is tired of the constant lane-jumping.
@VirtueOfNothing
@telswood
@Matt_L_Nash
The assumption that it’s the medics who’d always do the bailing is an interesting one.
5
0
0
3
13
141
Are these just random musings? We cannot have PA/AAs be medical practitioners for the purposes of this joke of a guidance, but not when it comes to the Medical Act (1983).
Or… are you suggesting they are in fact medical practitioners according to the Medical Act (1983)?

Interesting debate on titles-
The Medical Act (1983) almost always refers to ‘medical practitioners’ not doctors (or medical professionals).
#GoodMedicalPractice2024
means AAs and PAs once in UK regulation will have to follow the same high professional standards as doctors.
174
15
44
6
23
142
And a massive thank you to
@ProfRWinston
, also from
@UKLabour
, for standing up for the profession.
6
14
141
📌 Important for all doctors working in the NHS
NHSE are welcoming comments on a framework for MAPs
Link here:
Have your say to avoid another regulator snafu. It is designed to comment on ‘clarity of language’ but should be fundamentally rethought.
7
82
136
At a doctor in training in the North West, I am having to pay £240 for the duration of my rotation at
@WythenshaweHosp
@MFTnhs
. For this.
On a side note, why can
@SalfordCO_NHS
provide (much better) parking facilities to trainees free of charge?
Can we do better
@MCubbonNHS
?

28
11
137
Has the
@gmcuk
completely lost the plot? You must be literally insane. How is it in the public’s interest to lose a doctor for half a year over this? You lot are denser than fog.

This is an absolute travesty. I cannot put into words the amount of contempt I have for this.
@drcolinm
, I know you're not involved directly but as an Executive Officer - would feel comfortable defending this decision to
@bbcnickrobinson
on
@BBCr4today
?
23
40
267
7
5
135
😂 Subtweeting against IA from the French Alps is just pure gold. Never fails to deliver.
Massive queues as French are on strike AGAIN. God I detest strikes. If you don’t like your job go get a better one. That’ll do more to improve conditions than striking

15
0
2
6
5
132
The entirety of the upper echelons of medical governance frameworks in the UK are currently *that* Spiderman meme…
Honestly, is this a joke?
And the 7-digit number as a cherry on top…
One word for you,
@gmcuk
: No.

“PAs and AAs who register with us will receive a seven-digit number in the same format as a doctor.” - a deliberate attempt by the regulatory authorities to further obscure the differences between PAs and doctors.
11
39
124
8
33
128

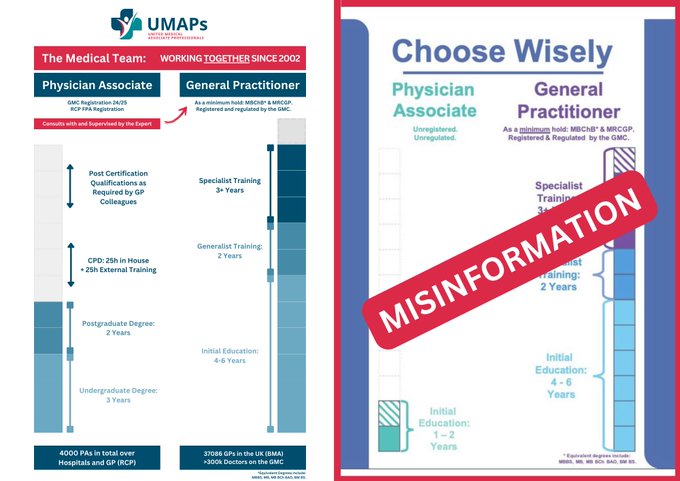
A masterclass in false equivocation

⛔️ Rebuttal
An infographic with misinformation is currently being shared on social media.
We corrected it for you 😉
🚨 MAPs, share away!
#PhysicianAssociate
#AnaesthesiaAssociate
#MAPs
#UMAPs
#MedicalAssociateProfessionals
#🐙
241
24
123
7
14
130
@NHSE_WTE
You should genuinely be ashamed of yourselves and start taking a modicum of pride in your work.
Not only are you sacrificing the quality of training standards.
Mark my words: You have blood on your hands.
2
12
130
I'd support this.
A clear line in the sand is necessary to (a) avoid scope creep and (b) ensure training of future consultant anaesthetists is prioritised.
🚨The uprising is real…
@RCoANews
AND
@NHSEngland
- pay attention
& it wasn’t even me this time! I’ve had countless DMs from fed up AiT who are taking action
See below - each with more likes than the votes needed to pass
1.
2.


10
43
249
3
15
125
Dave Kelly: “Your helicopter pilot should not look like this. He should be old, grey and wrinkled, with a look of slight disappointment when he meets you.”
@BigSick18
#TBS18

6
38
123
Imagine the concept of physician associates was an investigational medicinal product (IMP).
What would the process be to implement it into usual care?
Medicine is a safety-driven profession. For good reason. We take it seriously.
Why is this being undermined at every step?
"If we want to tackle the crisis in GP numbers, we should establish a pathway for physician associates to go on to train as doctors and for newly qualified doctors to go straight into five years’ training as GPs."
241
15
47
7
21
122
Does anyone else subconsciously hum or whistle a brief tune when in a stressful rapidly developing situation? 🤔
30
2
122
Surely the award for best title goes to
#47
:
"The lemon: an ‘apeeling’ teaching tool for epidural anaesthesia"
👏👏👏


All the abstracts from Annual Congress 2023 have been published now in a special issue of
@Anaes_Journal
Free to access here
#AC2023

2
6
24
15
26
119
Can the
@gmcuk
please clarify whether this is correct.
Reading the proposed order, it seems that there is in fact a proposal for an amendment of the Medical Act 1983 to include them.
Can we *actually* clarify?
If this is the case, I have questions ...
@drdernial
@wendyburn
Daniel. Just to clarify. They won’t be included in the Medical Act. There is separate legislation being laid - the AAPA Order - to regulate them albeit by the GMC
7
0
6
6
26
118
I like how Freedom To Speak Up is an anagram of its own antithetic acronym
7
16
117
The stills from Breathtaking look incredibly close to home for those of us that worked in the NHS through the pandemic.

16
24
117
Did anybody consider that Italian intensivists are the masters of ARDS and ventilation ... and are struggling with this? Will be interesting to see how this hits other territories. 😶
7
25
113
Not to mention that up until two months ago one of the biggest trusts in the country was still on ubiquitous paper notes. Yes, paper notes and Kardexes. In 2022. Have to walk before you can run.
Let’s rather focus on investing into important infrastructure, shall we? Robots… 🙄
5
9
113
Based on Twitter discourse, it seems that 13th March 2024 was a monumental day for the
@RCPhysicians
.
Let us see how they handle the results of the vote for Motion 5.
“More than 30% were against the motion and fewer than 100% were for it, so it fails, right?”
7
17
114
What fresh hell in what can only be described as 'professional appropriation' is this?!


17
15
112
Why is this midwife not hauled in front of her regulator right now? Sorry but this sort of arrogant dismissive attitude is beyond the pale. To have it broadcast as well?!

9
9
110
The statement from the Association of AAs makes for interesting reading. They openly oppose the AoA’s recent position statement. Some shared language in the document with recent RCoA comms.
The
@RCoANews
needs to very carefully consider its next steps.

21
24
111
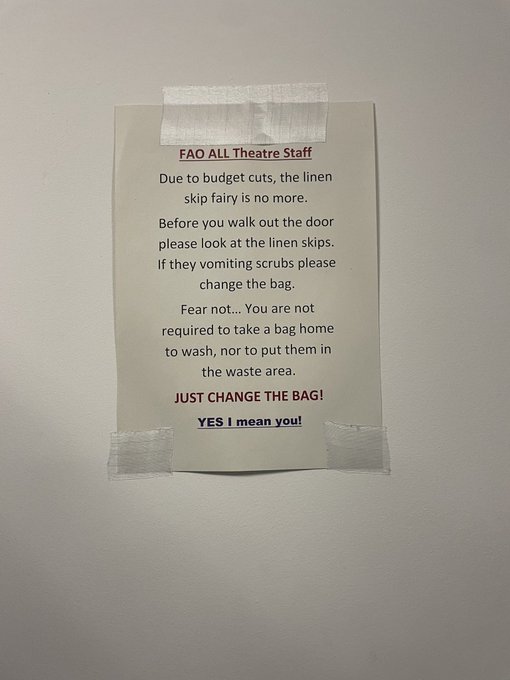
Stiff upper lip eh…
In late 2021 on an AMU placement at an unnamed trust as an ST4, I remember being asked to take bags of used scrubs from the changing rooms to the dept sluice. So that the consultant wouldn’t have to do it - she was about to.
What is wrong with the NHS?

We don’t have the money to do routine tasks so we’ll patronise people into doing it instead. Do these signs exist outside the NHS?
106
46
589
13
11
109
The FRCA Primary, in pen form


1
5
111
I would like to read, specifically, how scope will be defined. Because if it’s left to individual employers, this is insufficient and frankly dangerous.
The Royal Colleges need to be able to exercise their power here and define the scope in no unclear terms.
Scope of practice: We'll work with health services, royal colleges & stakeholders to help them define this, as they do for doctors. The professional standards that will apply to PAs/AAs are clear that registrants must recognise & work within the limits of their competence (6/8).
12
3
17
11
21
108
The higher-ups keep waxing lyrical about wellbeing.
THIS is where wellbeing starts.
And THIS is how wellbeing is denied to hardworking hoop-jumping doctors.
By absolute jobsworths. You’re done ANRO.
I think it’s safe to say that the membership EXPECTS the
@RCoANews
to ACT.
6
11
109
@drcolinm
They are healthcare professionals, yes. And we are medical practitioners. Would it have been too difficult to leave it at that?
‘Medical professionals’ just blurs the line, intentionally or not.
5
11
109
@Matt_L_Nash
@DrHuw
@Matt_ParaACP
@Dr_Done_
@FICMNews
An interesting level of hubris regarding neonatal airway management on display here. (Yes I have looked at your bio)
It always goes according to plan right?
4
0
107

Big headline: 252 RCTs looking at more than 30,000 patients show propofol increases mortality compared to ‘other’ (RR 1.10, 95% CI 1.01-1.20, p = 0.03). This translates to an NNH of 235.
Interesting one. Where does the effect stem from? 1/8

9
43
109
To say this is incriminating for the
@RCPhysicians
is an understatement. They appear to have misread the room back in 2015, and most importantly, not listened to expressed concerns from key stakeholders. They have been warned.

Way back in 2015 when Twitter/X and social media was not as big a thing as it is now, back in 2015, there were lots of concerns how
#PAs
where being pushed forward by
@RCPhysicians
whilst junior doctor strikes were on the horizon 1/x
44
347
683
2
26
109
I find it quite telling that the 30-page guidance by the
@gmcuk
makes reference to the word 'doctor' five times. As a footnote. Let that sink in.
🧵The updated standards for all UK doctors are now in effect
#GoodMedicalPractice2024
You can access a new digital version of the standards on our website.
We've improved how these are presented and structured, so you can quickly find the information you're looking for 🔎…

16
3
27
1
32
107
Remember to cast your votes before 16 February. I am voting YES for Full Pay Restoration.
#BMABallotReady
#PayRestoration
@BMA_JuniorDocs
4
12
103
I will shortly be presenting the preliminary findings of our Cochrane Systematic Review update comparing VL and DL in adults undergoing tracheal intubation at
#vDAS2021
as part of the Oral Presentation Session (Stream B). Remember to tune in!
@DAS_2021
@ProfAndyS
@doctimcook




4
28
101
Many thanks to
@ICS_updates
for the New Investigator Award and to the
@ManchesterBRC
for supporting the study.
As we move towards precision dosing of antibiotics in intensive care many important research questions remain.
Let’s see if we can answer a few.

Congratulations to Dr Jan Hansel on winning the
@ICS_updates
New Investigator Award 🏆.
The BRC-funded therapeutic drug monitoring study asks if a 'one size fits all' approach to antibiotic dosing in ICU can be improved.
Read Jan's blog on this study 👇

5
3
23
24
11
101