

David Sher
@DavidSherMD
Followers
2K
Following
4K
Media
67
Statuses
2K
"Ultimately, the secret of quality is love. You have to love your patient, you to have to love your profession, you have to love your G-d." Avedis Donabedian
Dallas, TX
Joined April 2019
RT @DrMLChua: This is BIG in the literal sense…. Massive effort bringing together FIFTY #HeadNeckCancer experts to debate and share their c….
0
8
0
This paper is a nice addition to the literature on the successful use of carboplatin-paclitaxel as a radiation sensitizer. The favorable results clearly motivate larger prospective trials on the use of carbo-pac as a radiation sensitizer in HNSCC. The most commonly delivered.

In patients with SCCHN receiving radiation with C/P vs cisplatin, there were no differences in locoregional recurrence-free survival, progression-free survival, distant metastasis-free survival, and overall survival. @DRNabilSaba @NikkiSchmittMD

5
5
21
Great. Medicare Will Require Prior Approval for Certain Procedures

nytimes.com
A pilot program in six states will use a tactic employed by private insurers that has been heavily criticized for delaying and denying medical care.
0
0
2
RT @hncalliance: There’s something powerful about being in a room with others who truly understand. We’d love to see you in person in LA on….
0
2
0
This guideline is an excellent document, not only with respect to the different variations of case presentations but also the thoughtful discussions. I am still perplexed by the avoidance of IMRT in this disease. It provides superior dosimetry, not just for the carotids but.
More than 12 000 new cases of laryngeal #cancer are diagnosed annually in the US. This Review summarizes the American Radium Society's guidelines on early glottic cancer management. @MCWardMD

3
8
44
RT @UTSW_RadOnc: Join us for the second PULSAR Consortium Meeting at @ASTRO_org on Monday, September 29, at 6 p.m! This special meeting wil….
0
9
0
RT @SameerKeoleMD: @DavidSherMD 💯 . The Clinical Trials Session is loaded too. @DrSpratticus will present NRG GU006 and I think it’s goin….
0
1
0
This plenary session will be AWESOME.

Plenary at the @ASTRO_org AM is stacked with 5 phase III studies. 🔹 Breast: RADCOMP (proton vs photon).🔹 H&N: TORPEdo (proton vs IMRT, Europe).🔹 Prostate: NRG GU005.🔹 Bladder: BART from @TMCIndia.🔹 Brain mets: METIS (RT +/- TTF)
1
0
16
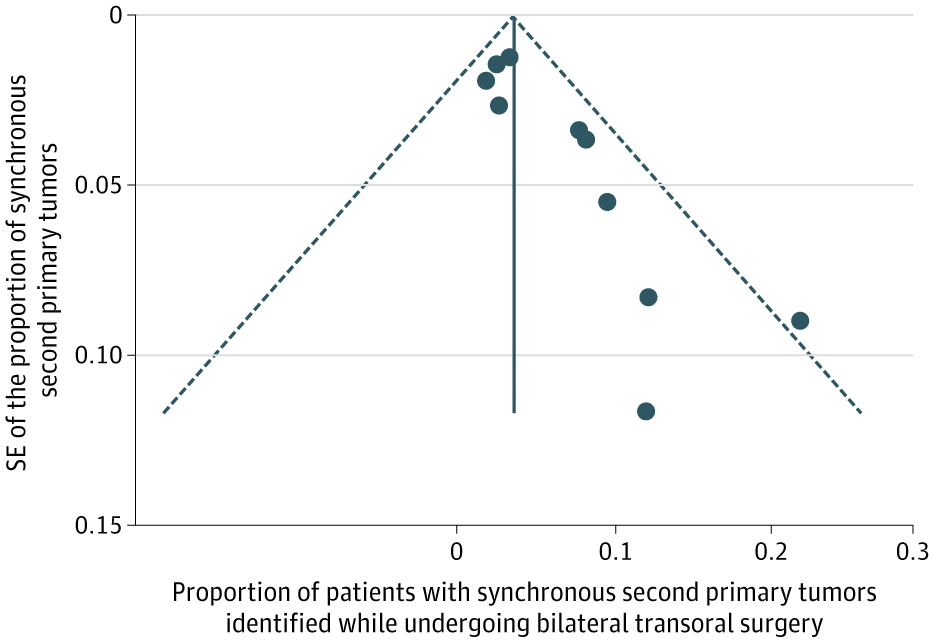
Very useful data. Now, it's time to generalize these conclusions to the unknown primary diagnostic work-up. The likelihood that a contralateral tonsil cancer generated the malignant adenopathy is too trivial to warrant bilateral tonsillectomies to find the primary, and.
Systematic review and meta-analysis: Omitting contralateral elective extracapsular tonsillectomy in tonsillar SCCa is safe, with low metachronous contralateral second primary tumor rates and no difference in survival outcomes. @andrewpete_
2
4
23
RT @jryckman3: @DavidSherMD The whole 3D vs. IMRT debate feels like a uniquely American pastime.
0
1
0
The 4-Field was a CC Wang/MGH technique to improve conformality in the 2D-3D era. It's my go-to if treating the whole larynx but IMRT is denied. Clearly better than laterals but still worse than IMRT. I can't wait for when we can talk about involved/single-cord treatment versus.

New in #practicalRO: Three-Dimensional Radiation Therapy for Early Stage Glottic Cancer Using a 4-Field Technique. #radonc

3
6
33
There are several limitations to the study. It kills me this wasn't placebo-controlled, but at least the mucositis evaluator was blinded, and there was an objective component to the grading (beyond pain). Oral cavity dosimetry is obviously very different for non-NPC patients,.
2
0
9
The median swallowing score was also superior in the mupirocin group at the end of radiation (33.3 vs. 8.3). Patients also reported less severe pain, both in terms of the score distribution as well as less severe pain (2.4% vs. 26.5%) at the conclusion of radiation:

1
0
2

The results were impressive. First, from a colonization standpoint, nasal mupirocin improved BOTH nasal AND oral colonization with S. aureus.

1
0
0
176 patients were randomized between mupirocin versus SOC (no placebo), where it was placed intranasally BID for 5 days in a row, then a week break, then 5 days in a row, etc. It started a few days before radiation, and the cycles ended when RT was over. There was one blinded.
1
0
0
Fascinating phase III trial of nasal mupirocin to reduce oral mucositis (OM) in patients receiving radiotherapy (almost all CRT) for NPC. Staph aureus growth on treatment has been implicated in oral mucositis, and we know that probiotics seem to be effective.
2
25
61
0
1
0
We are excited that our most recent amendment was approved, streamlining imaging criteria for enrollment. EA3211 is a phase III randomized trial comparing consolidative radiotherapy plus pembro with pembro alone in patients with oligometastatic head and neck cancer who have not.
#ClinicalTrial EA3211, led by @DavidSherMD of @utswcancer, aims to improve results for patients with #HeadAndNeckCancer that has spread to a limited number of places. Learn more:

0
5
14
RT @UTSW_RadOnc: Dr. @MHLinPhD presented, "Report on Common Clinical Workflows and Staffing Models for CTgART," in the session of "Staffing….
0
4
0