
Dr. Nina Niu Sanford
@NiuSanford
Followers
6,460
Following
1,939
Media
373
Statuses
3,511
GI Radiation Oncologist | Boston, @Princeton , @harvardmed , now @UTSWNews in Dallas | buying in bulk | @AAAS IF/THEN | Tweets=own | FCOI:
Dallas, TX
Joined November 2018
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
Usyk
• 440446 Tweets
WALK IN SKECHERS WITH APO
• 294142 Tweets
Campana
• 139379 Tweets
オークス
• 104518 Tweets
#GrandConcertENGLOTinMiami
• 77955 Tweets
#precure
• 69525 Tweets
#RingOfFire
• 68870 Tweets
プリキュア
• 52300 Tweets
#ブンブンジャー
• 50374 Tweets
上川外相
• 45026 Tweets
ゴーオンジャー
• 31550 Tweets
しんちゃん
• 25056 Tweets
切り取り
• 18778 Tweets
ステレンボッシュ
• 15372 Tweets
予定枚数終了
• 13582 Tweets
FIESTA FURIOSA
• 12167 Tweets
コラボ回
• 11929 Tweets
スピードル
• 11491 Tweets
Last Seen Profiles


















Pinned Tweet

In this week's
@JAMA_current
, my husband
@EthanLSanford
writes about the deaths of our daughter Ceci and his patient Terry.
About how grief has informed his practicing of medicine and living a fuller life.
Please read about our girl and share.

114
371
1K
Ceci died unexpectedly on Dec 5, 2022 at 14 months old. She was our daughter & we are devastated. She was so smart, smiley, stubborn & squishy. She adored the rabbits in our yard & playing with her nanny “Shang NaiNai” & sisters. She is loved & missed beyond comprehension (1/5).

5K
2K
58K
Without Ceci, the world is darker. To bring light, we will strive to be better parents, physicians, & citizens (4/5).

176
230
12K
We created a donation site in honor of Ceci. Funds will support research at Children’s Medical Center Dallas, where Ceci received outstanding care. Please RT & share.
@childrens
@UTSWNews
(5/5)

393
2K
10K
Ceci had limited mobility of her right leg, but despite whatever pain or discomfort she experienced, she eagerly fought to stand and keep up with her sisters. All she wanted was to share laughs with those around her. Ceci was so spoiled and so happy (3/5).
28
114
6K
Ceci had gross motor delay and right lower extremity weakness. After extensive work-up, including an open neurosurgical biopsy, she was found to have a tumor in the lumbar and sacral nerve roots. The exact tumor origin or type is still unknown (2/5).

33
132
6K
Happy to share that I have been promoted to Associate Professor! 😀
Getting to practice academic medicine is a privilege in many ways.
I am grateful to my colleagues, mentors, patients, & family.
58
12
483
Wow. Ethan’s piece on Ceci has received more than 30,000 views.
Thanks to all who read, shared, reached out ❤️.
The end of 2022 was tough, but we had so many happy moments with Ceci.
Sharing a few here - her birth day, etc.



16
31
447
Am I still an oncology researcher if I don’t publish a “COVID and Cancer paper”?
Asking for a friend...who is stretched pretty thin keeping up w patient care, homeschooling, and meeting pre-existing deadlines...🤷🏻♀️
19
25
391
Last night with my fellow Bostonian.
THANK YOU, Mark Wahlberg
@markwahlberg
for promoting awareness about COLORECTAL CANCER!

8
19
369
Little personal update:
On 9/23, we welcomed our pandemic DIY, baby girl
#3
, into our family.
Grateful & sleepy-eyed to be a party of 5.

35
1
337
“Mama, that’s you!”
Everything is bigger in Texas.
Grateful & excited to be a part of the
@IfThenSheCan
exhibit, featuring 120 statues of women in STEM fields - the largest statue collection of women in the US!


24
20
322
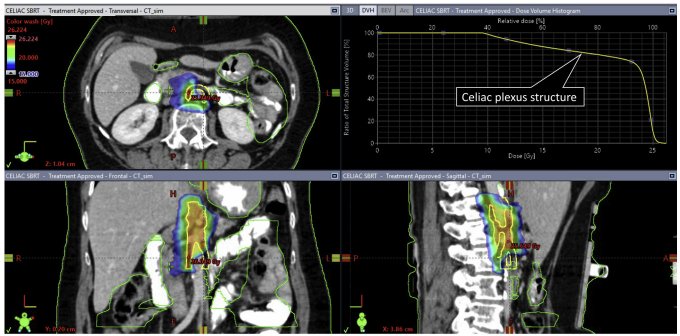
Phase II trial of SINGLE fraction (25 Gy) RT to celiac plexus for pain.
Of 90 pts, 53% had pain decrease, decrease in opioid usage & improved QOL.
Celiac plexus pain often debilitating & medication refractory.
Single fx RT looks convenient & effective!
#GI23
@Oncoalert
18
92
311
Why do some journals still require HANDWRITTEN signed/dated and scanned disclosures from all authors (while others have a completely electronic process)?
Collecting signatures is pretty tedious...I mean I ain't running for student body president here.
14
24
285
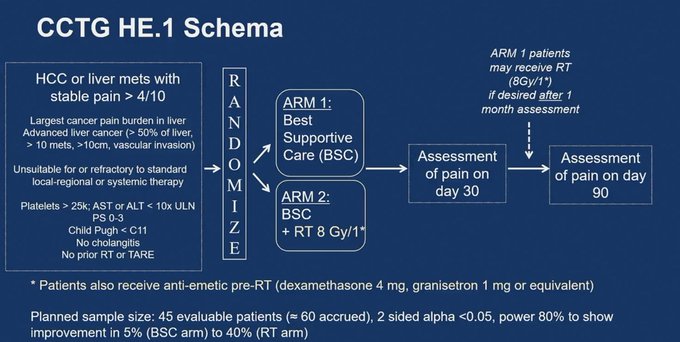
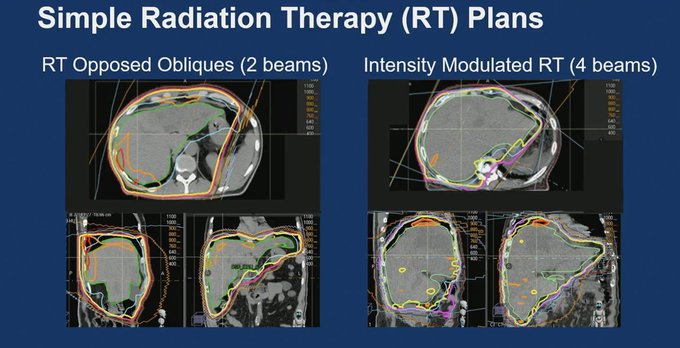
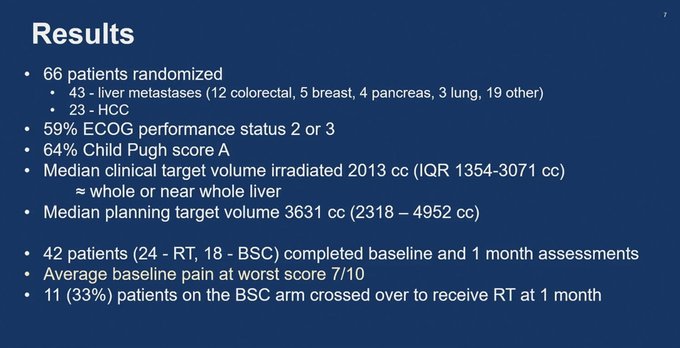
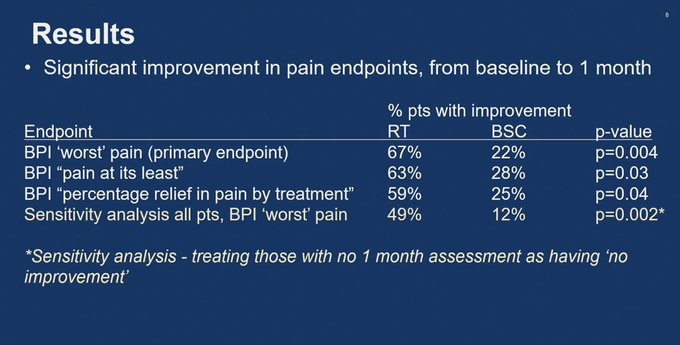
RCT of SINGLE fraction (8Gy) RT vs. BSC for painful liver metastases.
Patients receiving RT had improved pain on validated assessments. Also trend to improved OS (not powered).
Single fraction RT easy to administer (whole liver), cost effective, & convenient.
#GI23
@OncoAlert
7
121
275
When Ceci died, soooo many folks reached out to us from near & far. TY❤️.
But some sorta close to us, surprisingly never did. I can only give benefit of doubt they felt awkward.
My advice from other end now: ALWAYS reach out-text, email. Every little bit helps.
@KayeSteinsapir
17
4
273
Happy New Year. Heading back to work 1/4 & looking forward to it. Traveling to several places Jan/Feb.
Just putting it out here: please try not to feel awkward around me, like you can’t joke/laugh w/ me. Those who know me know I’m unoffendable, as long as the intention is good.

10
3
255
Got warning email re: need to complete 3 hrs of learning modules by 10/1 or else EMR suspension (granted, I procrastinated).
One of the modules is on physician burnout/fatigue/wellness.
#TheIrony
#TooTiredtoLOL
15
29
254
I have also been chaperoned while pumping during board exam.
Standing semi-nude in a bathroom stall w stranger, next to where someone just took a dump💩, to provide nourishment for my child, while also scarfing down lunch (pump during lunch or lose exam time)...was dehumanizing.

Dear
@ABR_Radiology
, Women are now > half of med school grads. Childbearing yrs & board exams will coincide. We are done being the ones who always have to adapt.
Love,
A dual Board-certified doctor mom of 3 who pumped in a bathroom w/ a chaperone & no extra time during Boards
15
88
427
27
41
238
Rad onc =
#1
for professional fulfillment 🙌🏽
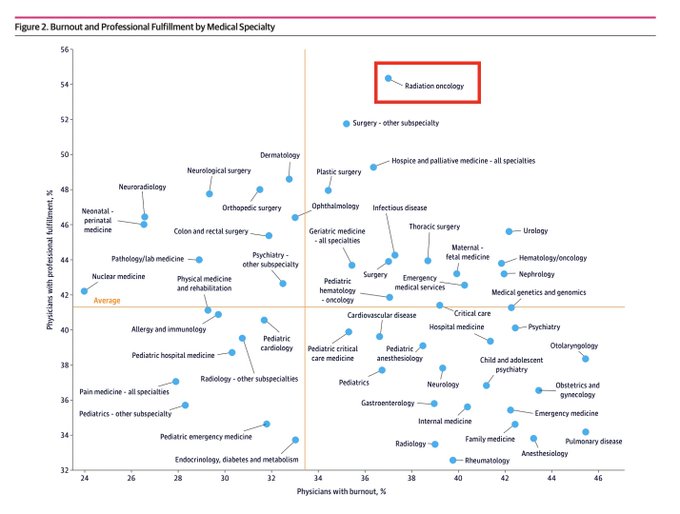

1 in 3 academic physicians report they are considering leaving their institution within 2 years. Burnout and lack of professional fulfillment were associated with intention to leave; a comprehensive approach will be needed to reduce physician turnover.
22
257
701
14
71
239
Thank you
@childrens
for including our family.
And thank you to everyone who has been so kind, patient & supportive over the past year.
❤️

"Life is short, beautiful and cruel. … We hope for Ceci to positively impact the world, and this fund is one way she will be able to do that." -
@NiuSanford
Read more about UTSW physicians Nina & Ethan's endowment in their youngest daughter's honor:

0
18
87
11
14
228


Feel like I've been living under a rock, but for anyone else who didn't know,
@jryckman3
has made ALL his notes available at .
Name of site suggests RT-specific, but information spans onc specialties across almost all disease sites. Incredible.

7
49
207
Honored to represent
#womenwhocurie
in this March 2020 issue of
@marieclaire
alongside these other badass diverse women scientists👩🔬
@IfThenSheCan
- including a shark researcher 🦈 , cosmetic scientist 💄astrophysicist 🌟 & AI innovator 💻.
#IWokeUpLikeThis
#Not
.




9
29
199
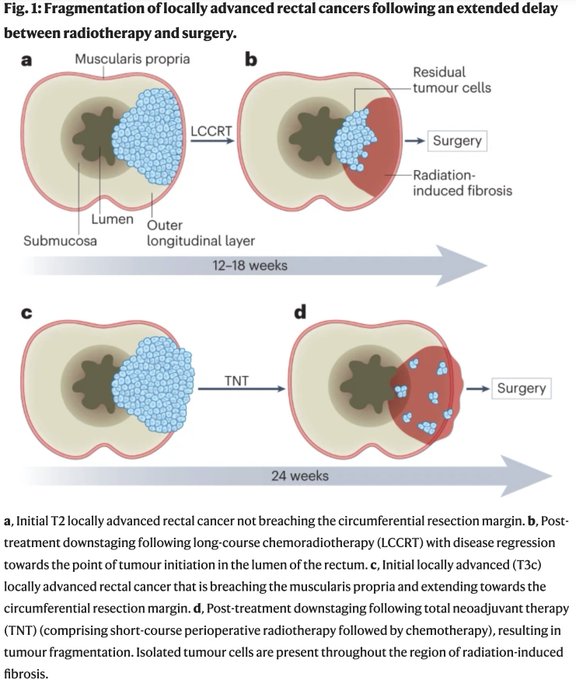
Better pCR but worse local recurrence w short course TNT in RAPIDO is counterintuitive.
This piece suggests could be due to fragmentation.
Fragmentation occurs after prolonged delay between RT and surgery and leads to pockets of isolated tumor cells including outside
9
76
200
I love a good debate, and last night’s was outstanding.
Thank you to
@bariweiss
and
@TheFP
for all that you do!


Amazing night in Dallas with
@TheFP
.
Grateful to
@cenkuygur
,
@SohrabAhmari
,
@nickgillespie
,
@AnnCoulter
.
And a huge thank you to
@TheFIREorg
🔥🔥🔥
22
45
562
9
13
193
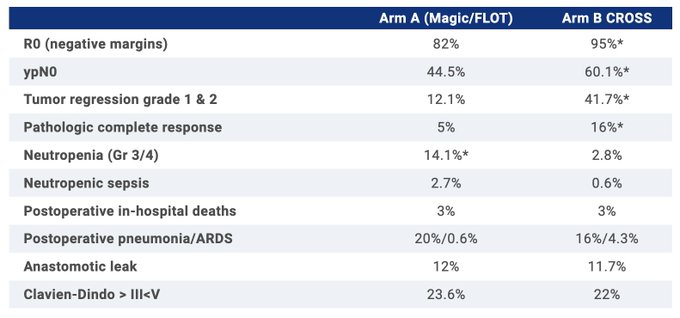
Neo-AEGIS: FLOT v CROSS for esoph/GEJ (n=362)
362 pts. No dif in 3-yr OS (57% v 55%), though path outcomes improved w chemoRT.
Not surprised that for all-comers no dif, clearly not one size fits all. Interested in future studies of chemo-->chemoRT-->surg.
#GI23
@OncoAlert
6
73
190
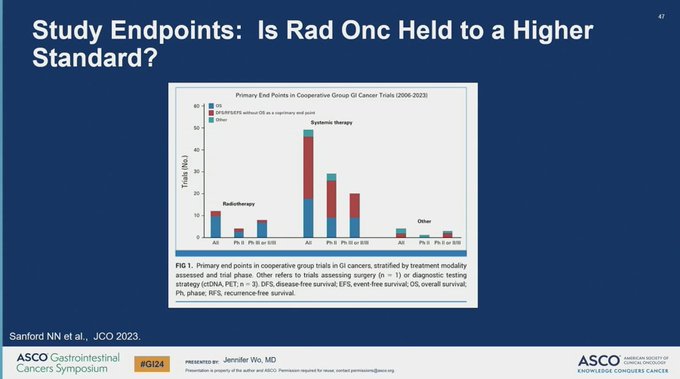
Out now in
@JCO_ASCO
!
Our work on clinical trial endpoints & inclusion criteria in GI oncology trials, and how we can better leverage RCTs to demonstrate the value of RT going forward.
With
@whallradonc
and
@TedHong9
.
Brief thread below.

4
63
165
Our editorial on radiation omission trials is out in
@JCOOP_ASCO
.
We analyzed 3 RT omission studies (PROSPECT rectal, PRIME II breast, EuroNet-PHL-C1 peds HL) & described separate methodologic considerations for each trial.
@whallradonc
, Chris Booth

10
59
163
5-year results of RAPIDO Ph III RCT are out.
Short course TNT vs. long course > surgery > adj chemo for high risk LARC (n=912!).
Short course TNT arm continues to have lower rate of disease-related treatment failure (1 endpt), driven by distant mets.

2
58
157
👋 Excited (& a bit nervous) to publish our piece on radiotherapy in pancreatic ca.
Thx
@JAMAOnc
for providing us a forum to discuss our controversial viewpoint, my awesome mentor
@TedHong9
, & the 2 reviewers who helped refine our message.
@OncoAlert
8
29
147
Out now in
@IJROBP
, my piece with
@BobTimmermanMD
describing a new way to approach radiation toxicity that we term as CUT: calculated useful trauma.
11
40
146
@sfmcguire79
Wow. I went to Princeton after graduating from a big public high school. I had taken a few advanced classes, but my preparation was far inferior to classmates from elite private schools, & we all ended up in the same college courses.
Would never have thought to suggest this.
19
1
141
How did 2Gy/fraction become standard in RT?
Answer: ram testicles.
Lab work done by the French showed less skin/sterility issues with 2Gy to ram testicles vs bigger fractions.
Much of the dogma in our field is based upon strong opinions, urban legend...& livestock lab data.
11
32
143
@KekoaMDPhD
@ASTRO_org
You shouldn't feel embarrassed that you got COVID. Hope you recover soon.
30
2
143
Out now in
@JAMAOnc
, our viewpoint arguing for better evidence supporting new technologies in RT.
The proton ship has sailed (in US), but we have window of opportunity to do the right studies for more recently debuted tech: adaptive RT, MR guided, etc

4
34
136
1/One of our senior med oncs asked me the other day what GTV and CTV stood for, which suggested that we/I are not doing a good job explaining some of the technical aspects of our field.
So, quick TWEETORIAL on RAD ONC target volume definition (what all those letters mean!):
2
53
138
@VonettaMW
@michaelharriot
Appreciate this thread.
We had hair products growing up, but had to be <$1 (i.e. Suave). Sniffed Herbal Essence for free at CVS.
One reason I loved sleepovers was cuz I got to sample friends' buffets of soap/hair products - & I def used more than recommended pea size serving🙃.
5
1
132
Reviewing scans from home:
Step 1: Type in Citrix password
2. Log in with Duo mobile
3. Log into UTSW
4. Click Epic EMR app
5. PRAY PRAY Epic opens
6. Log into Epic
7. Go to patient chart
8. Log into radiology reviewer
9. Step 8 again
…Epic crashes restart at Step 1
17
4
135
This Common Sense Oncology (CSO) manifesto is a must read for the oncology community.
"CSO will promote interventions that measurably improve the lives of patients. We will celebrate well-conducted trials and promote effective treatments, but will also speak up about

Our inaugural paper, our manifesto is now out in
@TheLancetOncol
. This paper describes our mission, vision, and guiding principles. We also now invite you all to join our movement- our website is now live.
16
167
394
7
41
135
Where is RT 👀?
Despite overall dearth of RCTs comparing local modalities in HCC, we have randomized studies in support of RT across the disease spectrum:
Early/Intermediate stage: Loma Linda trial - RT (protons) vs. TACE: similar OS, RT better PFS & local control

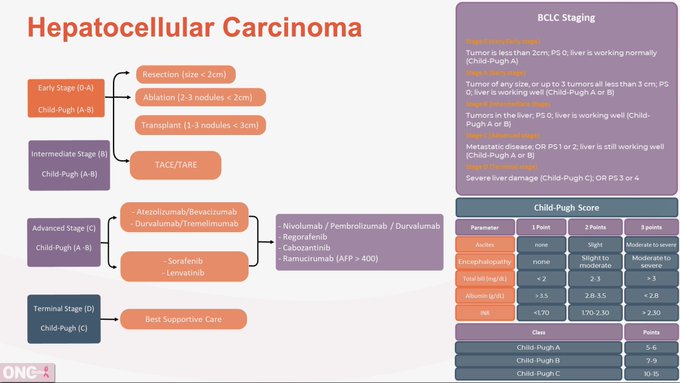
This is the
#Algorithm
we have used during our discussion w/
@GIcancerDoc
for
#HCC
!
#OncTwitter
#MedTwtitter
#gism
#MedEd
@CancerNetwrk
#OncEd
#LiverCancer
6
37
113
12
37
133
As someone who is pro-choice and lives in Dallas, seeing medical conferences boycott certain states including mine kinda feels like a slap in the face to patients/trainees/physicians living here 24/7.
18
10
128
US school systems built for families with 1 stay at home parent.
Academic MD jobs built for the same (or no kids at all).
Parents in dual working families: prepare to feel like a failure, daily.
#MondayMotivation
#TheMoreYouKnow
14
6
123
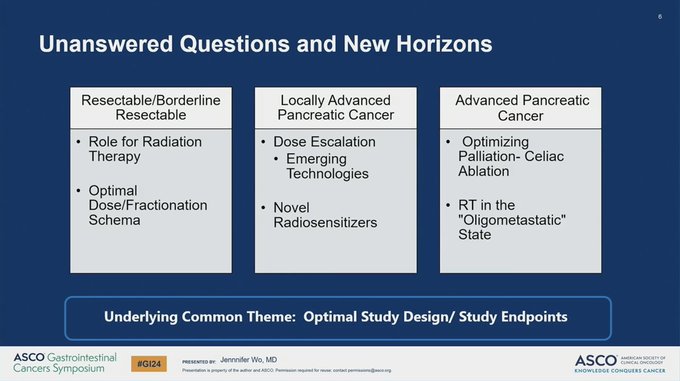
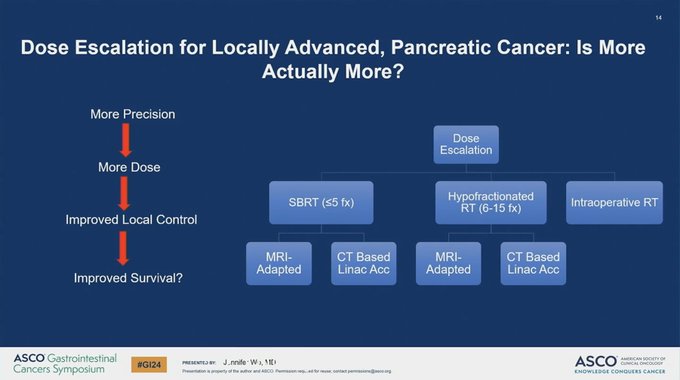
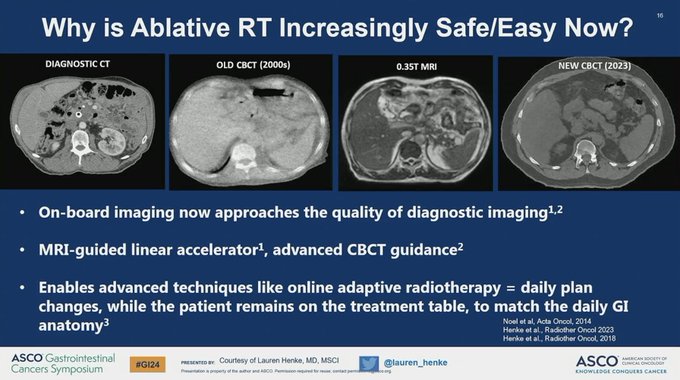
Jen Wo just gave an OUTSTANDING, balanced talk on the role of RT in pancreas cancer.
Great review of state of evidence, novel technologies, radiation planning, & studies hopefully coming down the line.
(and thx for the shoutout on our paper 🙂)
#GI24
5
35
122
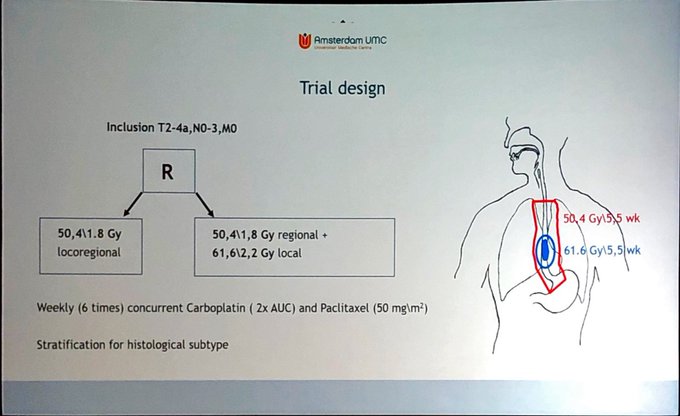
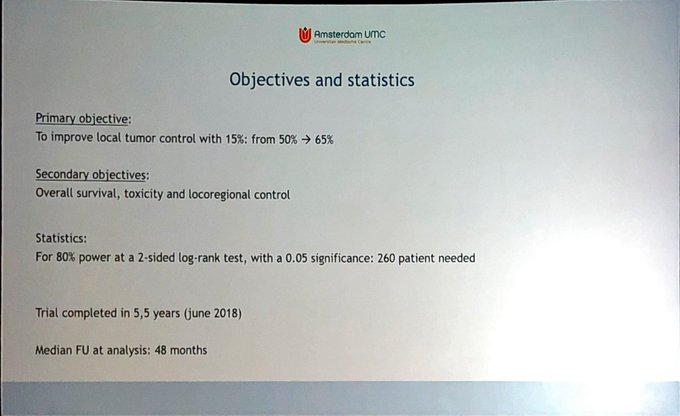
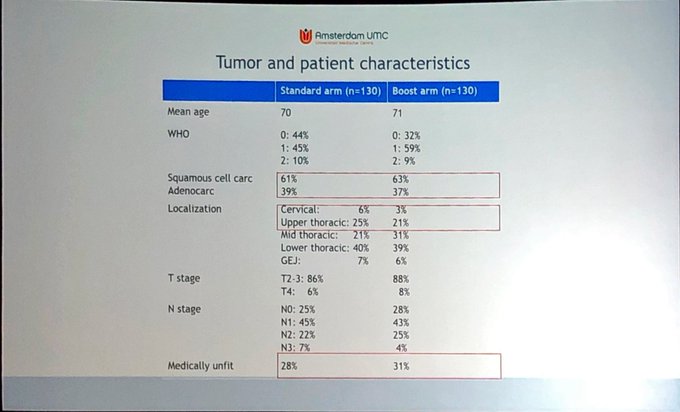
Large RCT in esophageal ca showed no benefit for dose escalation (50.4 vs. 61.6) for definitive chemoRT, even when stratified by histo. Flashback to INT0123 but w/o early deaths.
How do we reconcile lack of benefit in esoph SCC w H&N data? Still a role for higher RT?
#GI20
17
64
121
I feel fortunate & happy to be a radiation oncologist.
Thank you,
@S_W_R_O
, for highlighting!

On this
#WeWhoCurie
Wednesday, we highlight
@NiuSanford
, Dr. Sanford is an assistant professor
@UTSW_RadOnc
and chief of GI radiation! Today she shares with us the story of her path into
#RadOnc
in a fun and eloquent way that can resonate with many of us😁

3
8
58
7
10
120
Where does sparing 700cc liver RT metric come from?
Estimate of liver being 2000cc, & idea that for parallel organs, 35% must be preserved to maintain function (Red J 2005).
Surgeons individualize remnant liver requirement based upon liver size/health - think we should too.
12
28
118
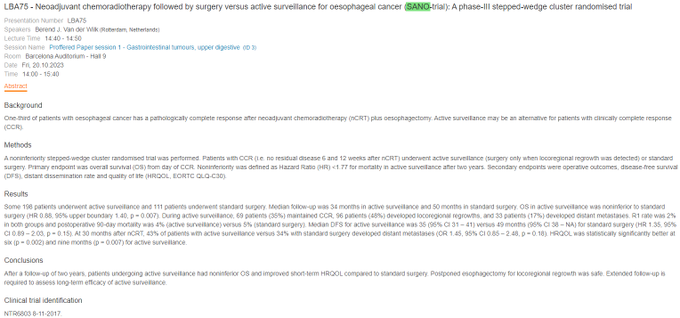
What do patients with esophagus cancer value?
In this study (n=100), patients were willing to accept a 16% decrement in 5-year OS for an opportunity to undergo an active surveillance regimen after neoadjuvant chemoRT.
Therefore, with SANO showing similar OS and better QOL with
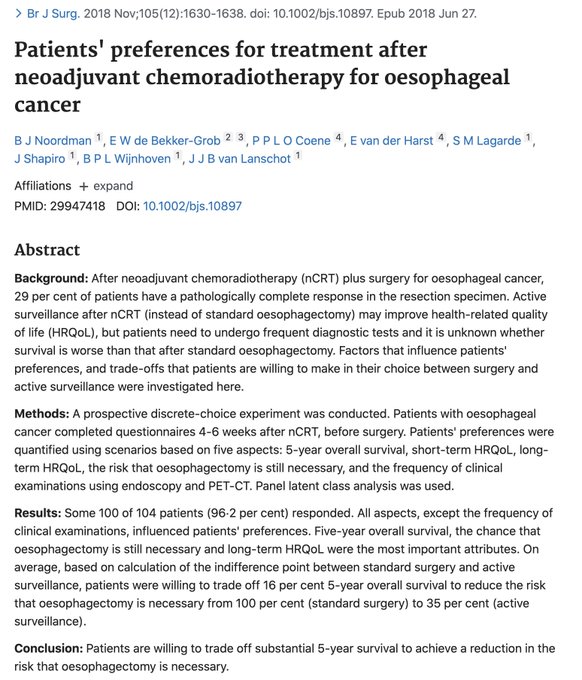

🚨🚨🚨SANO-trial!! Been waiting for this one!
Patients with esophagus ACA with cCR after CRT randomized to active surveillance vs. esophagectomy
✅Non-inferior OS and improved QoL with AS approach!
This is 🔥🔥🔥
Looking forward to manuscript to unpack the details
#ESMO23
11
97
236
3
36
117
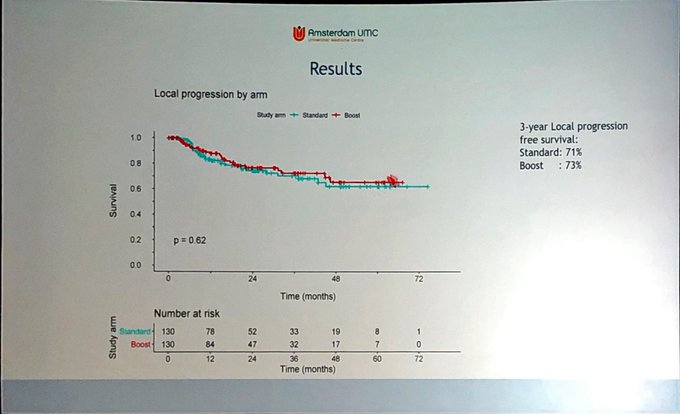
Do we finally have an RCT of RT in biliary cancers?
Look forward to RACE-GB study
#ASCO23
N=135 pts w unresectable gallbladder cancer s/p chemo x 4 mo --> chemoRT (45Gy + 9Gy boost) vs. obs.
ChemoRT improved OS (1 endpt), 10 vs. 4 months (p=0.001).
4
41
113
Here is our take on RCTs for RT in oligometastatic GI cancers.
Many have attributed negative trials to patient selection. We suggest other reasons studies may not meet endpts: large hypothesized OS benefits, crossover, & more
w
@whallradonc
,
@TedHong9
6
42
110
Totally agree w
@ldawsonmd
that it’s past time for SBRT to be included in HCC guidelines!
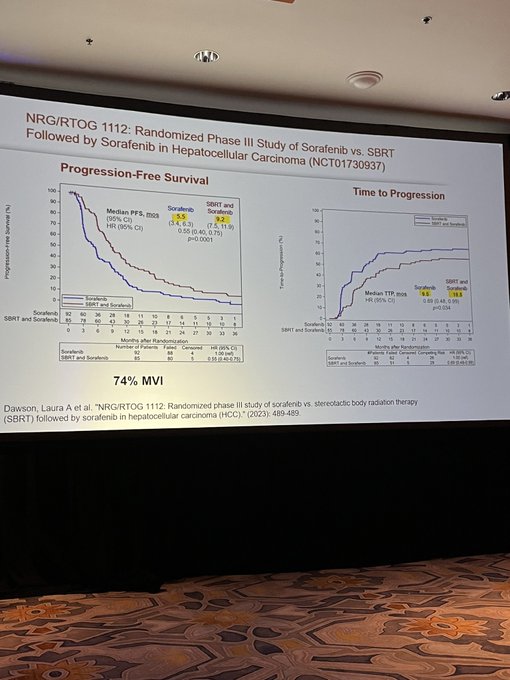
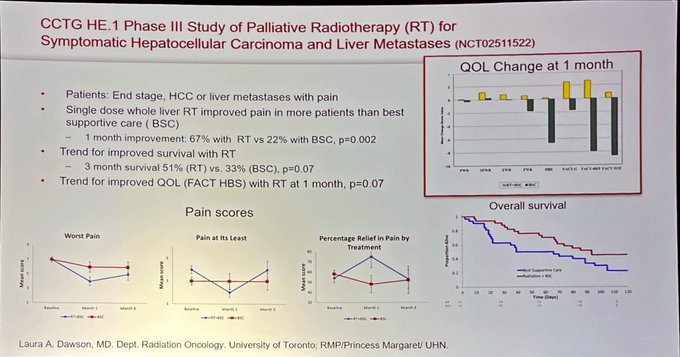
There is randomized data showing benefit to SBRT in HCC across settings (curative to palliative, with improvements in OS & QOL).
@HCCLIVEConf
5
22
109
Finally!
Our
@UTSWNews
women’s wall “Celebrating Breakthroughs Together” is live!
Excited to be included alongside so many women I admire greatly…somehow they let me slip in through the cracks 😛.
If you’re on campus, come check us out, next to medical school caf. 1/3



9
20
110
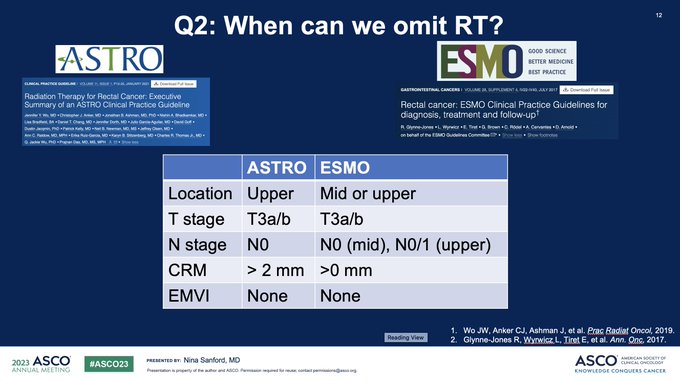
PROSPECT: many patients would have qualified for upfront surgery w/o RT per ASTRO & ESMO guidelines. Then, potential de-escalation of adj chemo pending pathologic findings.
6 months of FOLFOX in experimental arm of PROSPECT likely overtreatment for a proportion.
#ASCO23
🚨🚨🚨 PROSPECT Trial has landed!
Congratulations to all investigators,
@ALLIANCE_org
, for this important trial!
This study is important, will shape, and SHOULD alter practice for OPERATIVELY managed patients with favorable risk LA- rectal cancer.
4
81
157
6
39
109
I finally read CROSSFIRE (IRE vs. MRI-guided SBRT after chemo in locally advanced pancreas cancer) in detail.
There are a few issues. Brief thread.
8
48
105
1st time being a visiting prof & grand rounds speaker (still think it was ? mistake invite).
Thank you to the wonderful folks at U Arkansas for having me!
Loved my visit, & enjoyed sharing the cool work being done in our department by
@chikarebeccaN
@ndesai2005
@DavidSherMD
!


5
6
104

Trial participation is burdensome for patients.
Especially when randomized to control arm & essentially receive the same SOC treatment they would off study, but need to keep coming in for extra visits, surveys, testing.
Patients should be reimbursed for trial participation.
7
11
97
1/I am honored to be named a Dedman Family Scholar & grateful to the Dedman family for their transformative gift, which I plan to use in studying racial disparities in young onset colorectal cancer.
I will also share that I applied for the same award last year and was rejected.

Congratulations to Nina Sanford, M.D. (
@NiuSanford
) on being awarded the Dedman Family Scholar in Clinical Care!
The award is given to two early career faculty members each year and totals $600,000 over the course of four years for each scholar.
2
2
21
16
4
96
AWESOME to see powerhouse female GI radiation oncologist
@mpalta1098
chairing this year’s GI ASCO meeting!!!
#GI22

2
11
96
#GI22
: PD-1 blockade alone for dMMR locally advanced rectal cancer
@LumishMelissa
et al, NCT04165772
Stage II-III dMMR LARC treated with anti-PD-1 alone x 6 months.
All N=12 patients responding (ORR=100%) & 7/7 (100%) completing 6 mo. of treatment achieved cCR!

1
45
95
Congrats Bob Timmerman on the Watson Award,
@UTSWNews
highest clinical honor. Bob often tells us that his 1st study on SBRT was rejected by almost every journal & he was booed during 1st podium presentation. He is a thought leader, mentor, & exemplifies grit & persistence.

2
16
95
This is a great
@ASCO
educational chapter on multiD management of rectal cancer led by
@KristenCiombor
(med onc),
@JoseGuillemMD
(surgeon), & Corrie Marijnen (rad onc - PROSPECT discussant).
Take a read! I learned a lot.
0
40
95
Wanted to give a shout out/THANK YOU to pathologists. The often unsung heroes. Several worked so hard to help Ceci. First, her primary pathologist
@childrens
, Dr. Ameet Thaker (& Veena Rajaram) spent so much time on her case: 40+ stains, reading primary literature, & more 1/5.
2
8
95
My unsolicited advice to future trainees: in residency you’ll get to work w many attendings.
On each rotation, maximize your learning based on their strengths (Anatomy? Bedside manner? Literature?)
But also learn from their weaknesses by committing not to repeat them in future
3
8
94
In year 5 of my attending life.
I’ve dabbled in way too many things since I started.
What should I focus my career on!? How do I decide?
Any other no longer junior faculty feeling a bit lost!?
17
4
94
Why isn't organ preservation more of a thing for esophagus cancers (other than upper SCC)?
In CROSS, pCR was 49% for SCC, 23% adeno - and that was with 41.4 Gy. With higher dose of RT, addition of IO, and longer interval to assessment, we could probably improve upon complete
18
16
95
Goodbye to
@IyengarPuneeth
who leaves us this week for
@MSKCancerCenter
.
Great mentor, colleague, leader, friend.
Don’t forget us in Dallas.


6
5
93
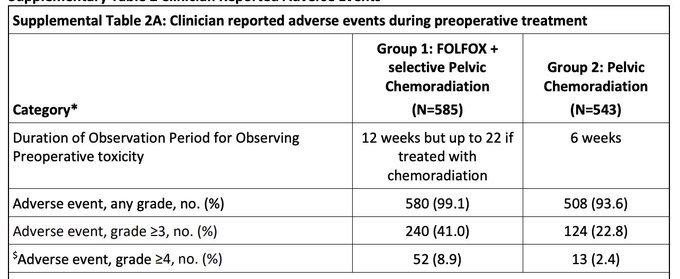
Need to carefully consider toxicity trade-offs in PROSPECT.
Rates of pre-operative Gr3 & 4 toxicity were 2x and 3x higher in FOLFOX group vs. chemoRT.
#ASCO23
5
45
92
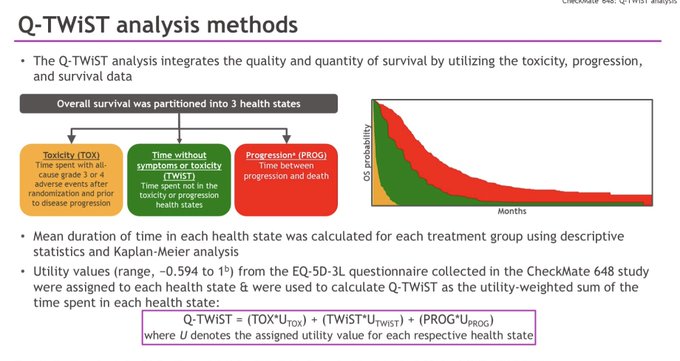
At least 2 presentations at
#GI24
(Checkmate 648, FRESCO-2) use Q-TWIST as an endpoint.
Q-TWIST integrates BOTH quality and quantity of life.
Surviving time is partitioned into 3 states weighted differently:
1. Time with grade 3 or 4 toxicity (TOX)
2. Time without symptoms of
6
30
92
What is the opposite of radiation omission in breast cancer?
CONGRATS to absolute boss rad onc
@AsalRahimiMD
on her $2 million
@CPRITTexas
grant studying non-operative management with definitive RT in early stage breast cancer!
👏🏽👏🏽👏🏽
(1/2)Congratulations to our Chief of Breast Radiation Oncology Service and Associate Vice Chair for Program Development,
@AsalRahimiMD
, who was awarded $1,999,963 to conduct a clinical trial using a preop ablative radiation approach for patients who have early-stage breast cancer

5
15
71
4
14
92
Just saw this rectal cancer study in
@JAMAOnc
– lots to digest.
Despite absolute 50% drop (87% to 37%) in use of neoadjuvant RT for lower risk (cT1-3, N0-1, MRF-) rectal cancers from 2011 to 2016, no difference in local recurrence & survival improved.
3
32
90
A non-inferiority trial with protons doesn't make sense, b/c they are much more expensive.
Need to show protons superior.
And the non-inferiority margin here is 1.53 - so PFS can be 53% worse with protons, & the study is still considered a proton win?


@drmattmc
@seanmmcbride
@subatomicdoc
@EvanThomas84
@DrChowdharyMD
It is not rigorous. It’s design is a concession to the proton lobby. The prior data suggests we will learn nothing from the PFS primary end point.
Academic point since ASTRO encourages treating off trial anyway though.
1
1
12
7
22
91
So, school is now virtual for my 4 year old in quarantine after exposure to a COVID+ classmate.
At the same time we just got notified by my department that we are no longer allowed to see patients by televisit/i.e. no WFH.
Just more impossible situations for working parents.
9
7
89
Wow
@costplusdrugs
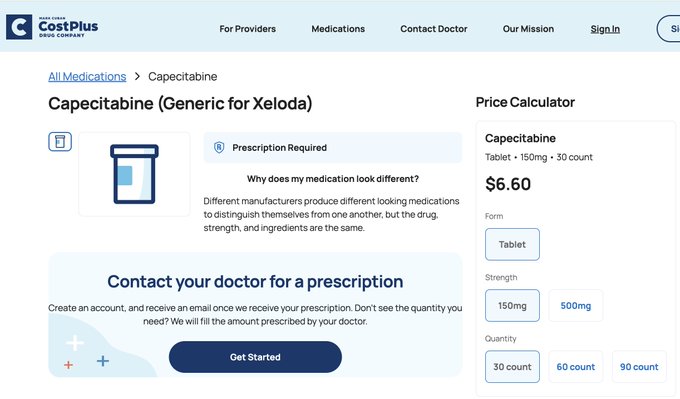

Shout out to
@mcuban
FTW again with generic xeloda (capecitabine) for $40/mo
@costplusdrugs
. Seriously this is a total game changer for so many of our patients, esp with this drug on national shortage.
1
8
43
3
22
90
An alternate take: 4 months of peri-op ECF/FLOT was no better than 5 weeks of carbo/taxol with 41.4 Gy RT (one could also argue outdated).
Toxicities were worse with peri-op chemo. Conversely, there was no difference in post-op morbidity.
At the end of the day, the study showed
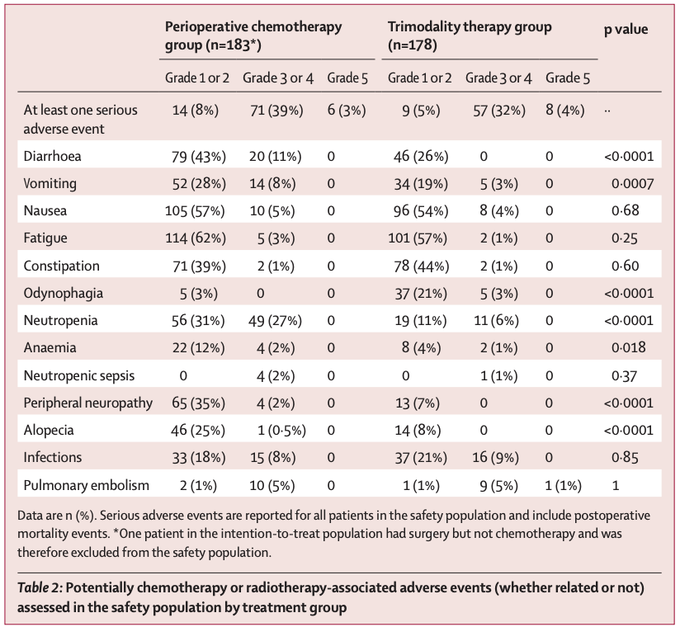

Neoadjuvant Chemorads vs (outdated) Chemo for esophageal adenocarcinoma - no difference in survival. So what does the radiation therapy add other than increased surgical morbidity and long term pulmonary toxicity?
8
20
66
6
38
88

Spending some time reading about QOL measures in oncology trials, & not feeling too reassured. Some issues I’ve seen:
-Little consistency on what is considered clinically meaningful
-Range of survey instruments used
-Lots of drop off, particularly at later time points. If a
11
14
90

Highlighting a few fantastic rectal cancer trials presented at
#ASCO22
yesterday assessing novel RT strategies/combinations to increase organ preservation.
@OncoAlert
1
35
86
Slides! Retrospective study of short vs. long course RT for watch and wait at MSKCC.
Similar rates of initial complete response (46%), but response appears more durable with long course --> higher rates of organ preservation. Dose matters.
#GI23
@OncoAlert
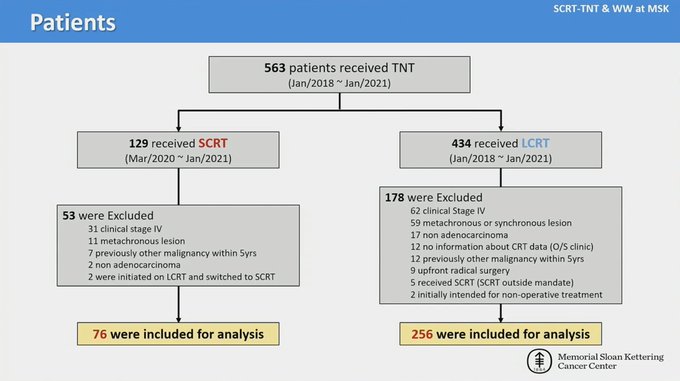
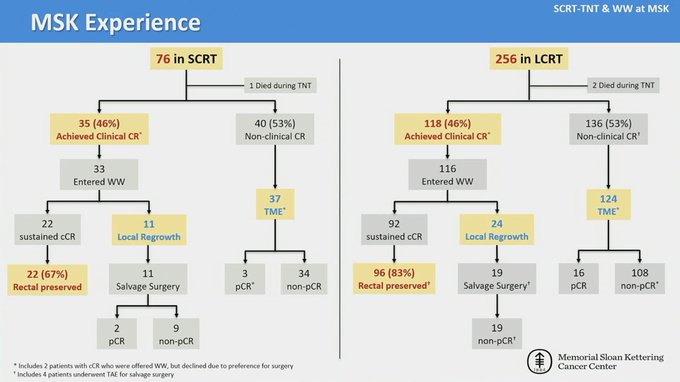
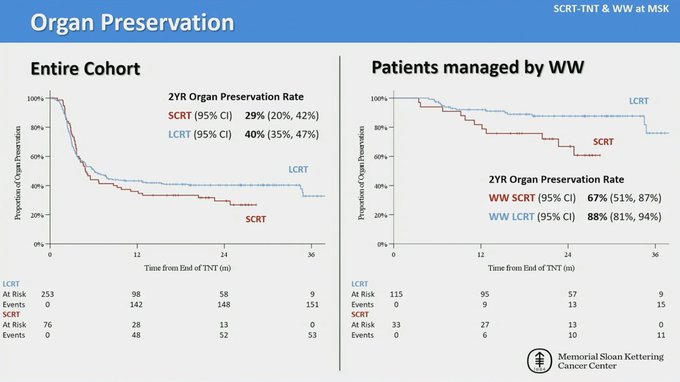
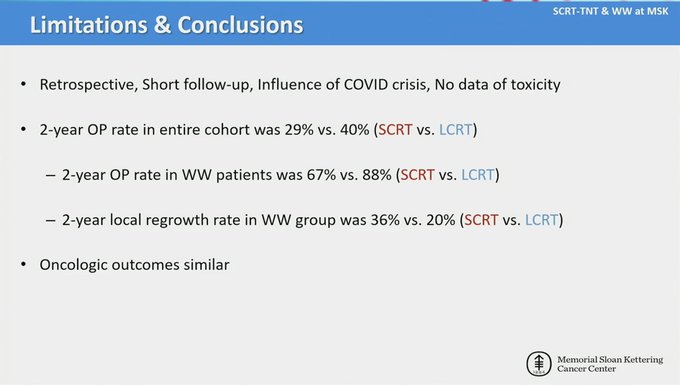
3. Retrospective study from MSKCC (n=332) of long course v short course TNT strategies. Short course during COVID, reducing selection bias.
No dif in cCR (46%), but long course had lower rates of regrowth (20% v 36%) --> higher rates of 2-year OP (40% v 29%).
@JoshSmithMDPhD
0
8
32
4
31
87
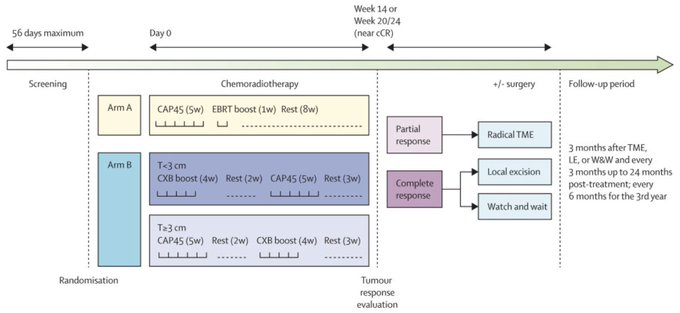
Impressive results from OPERA RCT, just published.
3-yr organ preservation rate for tumors <3 cm was 97% w brachy boost after chemoRT. 1st RCT showing higher RT dose -->higher OP.
Couple points after reading paper (that I didn’t catch at ASCO). 1/5
3
54
82
Folks who eat with camera on during Zoom meetings are my people.
6
0
81
Since we're on the topic of radiation dosing, this piece in
@IJROBP
by Timmerman on SAbR & constraints is a MUST read.
Re: Timmerman constraints: "In all honesty, except for spinal cord, all other limits for the original table were my educated guesses."
3
21
79
There will be lots on ctDNA at
#GI24
.
Ahead of the meeting, this is a really good review on the various indications for liquid biopsy (detection, surveillance, therapy selection, etc), their evidence & potential pitfalls.
2
19
80
Rad Onc trainees on the COVID19 frontline, including
@DrChowdharyMD
,
@AmandaRiveraMD
,
@goharmanzar
.
We are doctors first, then oncologists, then radiation oncologists.
#RadiateLove
Proud of them for stepping up to the challenge, but wish they never had to be in this position.
3
12
76
I passed rad onc oral boards! Grateful to my colleagues, mentors and most important my family - including hubby
@EthanLSanford
who puts my with my crazy and our 4 month & 2.5 year old (anti)study buddies who keep it REALLY real all day everyday.
#blessed
#postboardslivin
#HROP
9
3
78
Thank you, Accelerators, for hosting a great pod episode featuring
@BobTimmermanMD
!
Topics discussed: radiation toxicity/risk tolerance, technologies & Wagyu beef.
Our conclusion is that rad onc needs 30+ more Bob Timmermans.
Just finished taping – stay tuned!

5
8
80
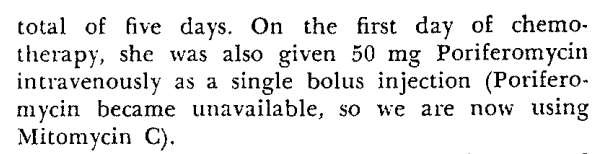
Interesting fact.
How did mitomycin C come to be used in anal cancer?
By chance, pretty much! Original plan was for poriferomycin, but pharmacy ran out. No preclinical data or Phase I studies for mitomycin C in anal cancer.
See below, patient 1, original 1974 Nigro paper.
2
22
79
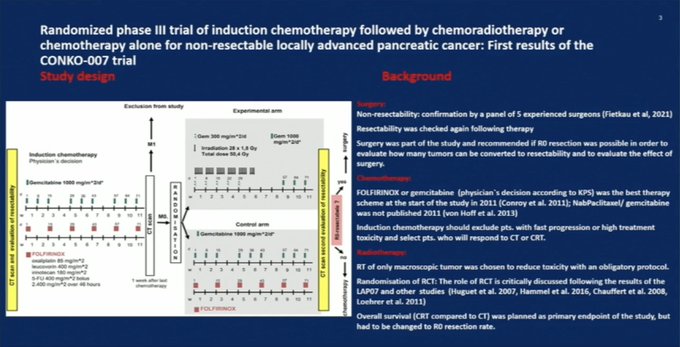
CONKO-007: RCT of induction chemo +/- chemoRT for locally advanced PDAC.
At face value, this is (another) negative RT pancreas trial. For all comers, no difference in R0 resection (primary endpoint), no difference in median OS. 1/4
#ASCO22
@OncoAlert
1
41
78
Been gone too many weekends.
Worst part was missing out on weekly Costco runs. Finally back at my happy place now.
This $1.50 combo never disappoints.

5
1
79
Hanging with one of my rad onc role models
@ldawsonmd
at
@HCCLIVEConf
conference in Huntington Beach!
*Cue Laguna Beach theme song*

3
3
77
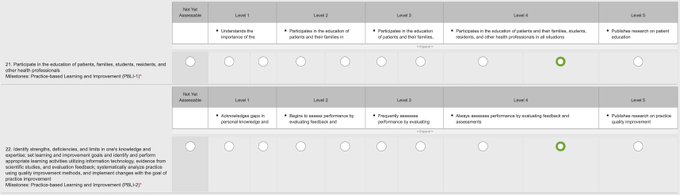
Filling out eval for my outstanding rad onc resident.
Why does achieving Level 5 require publishing research in that specific milestone?
Shouldn't this be an assessment of clinical competency above all else?
What if resident does research but is clinically mediocre?
#MedEd
13
4
76
Excited for
#ASTRO23
Humbled (truly) to be presenting 0 posters/0 talks 😃
Finally en route to SD - see everyone soon!!!

5
1
76
Compliance & Toxicity of TNT in OPRA:
No difference in chemo completion rates b/w induction vs consolidation chemoRT (~85% FOLFOX, ~75% CAPOX)
-->reassuring that chemoRT 1st didn’t decrease ability to complete all intended cycles of neoadjuvant chemo.
1
27
75
Today I turn 33.
I have kids that are happy & confident, and family is healthy thus far - something I would have taken for granted 10 years ago.
I live in Texas, and my favorite hobby is grocery shopping - things I would never have expected.
Feeling especially thankful today.

13
0
75
Huge thanks to
@PreetiNMalani
, A Piece of My Mind section editor, for all her help/back and forth emails.
Also thank you to
@ndesai2005
for reading an earlier version.
2
1
74
We may not have SD beaches - but we have rooftop pools.
@UTSW_RadOnc
here to celebrate Chika’s
@chikarebeccaN
bday 🥳

1
4
75
"The goal of all cancer treatments is to maximize efficacy while minimizing side effects"
A balanced interpretation of PROSPECT.
This piece was written by the senior author of PROSPECT (Harvey Mamon) and others.

@nytimes
and
@Telegraph
may want to read
@ASTRO_org
piece from GI experts on how to interpret PROSPECT.
I’m not a journalist, but as a scientist always want to ensure what I write is accurate. Starting with experts may help.
7
26
78
2
20
73