
Angela Reiersen, MD, MPE
@AngelaReiersen
Followers
5,750
Following
5,913
Media
268
Statuses
6,672
Associate Professor of Psychiatry @WUSTL ; Opinions are my own; Tweets are not medical advice. Say my name:
St Louis, MO
Joined October 2020
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
#母の日
• 337969 Tweets
#นาฏราชครั้งที่15
• 309964 Tweets
WIN AT NATARAJA AWARDS
• 119280 Tweets
Feliz Dia
• 117976 Tweets
テンハッピーローズ
• 109104 Tweets
Mães
• 84346 Tweets
#光る君へ
• 71957 Tweets
カーネーション
• 54573 Tweets
MC NUNEW EP1
• 49618 Tweets
Cibeles
• 44500 Tweets
#やまラスト
• 37877 Tweets
新ビジュ
• 35582 Tweets
DONBELLE BOX OFFICE LEGACY
• 31905 Tweets
Ohm X Nataraja Awards
• 17094 Tweets
#光る君ヘ
• 16011 Tweets
GENCelebrate Music With BINI
• 12262 Tweets
清少納言
• 10366 Tweets
















Pinned Tweet

We are still recruiting Missouri & Illinois residents for our fluvoxamine long COVID trial. See this flyer for contact info.
3
27
56
How fun. Now I have COVID for the 5th time, and I am simultaneously having a shingles outbreak. Turns out there is some evidence COVID may increase the risk for a shingles outbreak in people over 50.

1K
342
1K
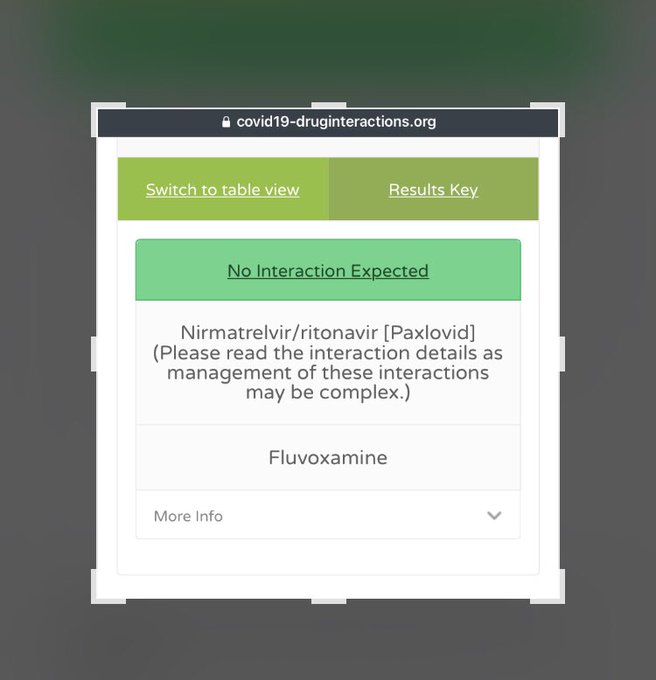
So, I have acute COVID again (3rd time). I am taking both Paxlovid and fluvoxamine since they have different mechanisms that I think should be complimentary. This is not medical advice. Everyone should speak to their own doctor about what is right for them.
193
128
1K
Ontario becomes the first province to list fluvoxamine as a COVID-19 treatment to consider via
@CTVNews

32
212
629
There is a hint that fluvoxamine may have prevented the most severe forms of long COVID: those randomized to fluvoxamine were about half as likely to report being less than 60% recovered at follow-up. Small sample size, not statistically significant (low power), but interesting.
21
99
534
Fluvoxamine: an inexpensive pill that works against Covid-19.
29
165
458
Just published a new paper with
@Bradley_A_Fritz
,
@EricLenze2
,
@farid__jalali
, and
@HoertelN
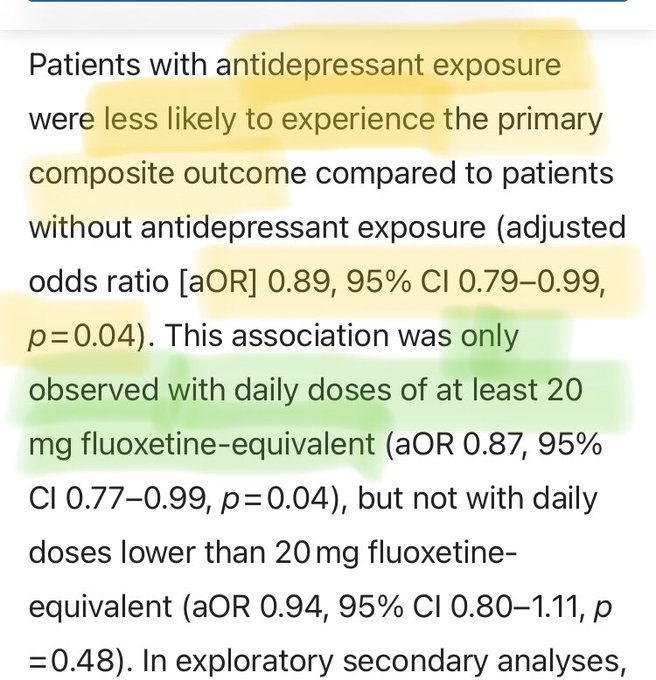
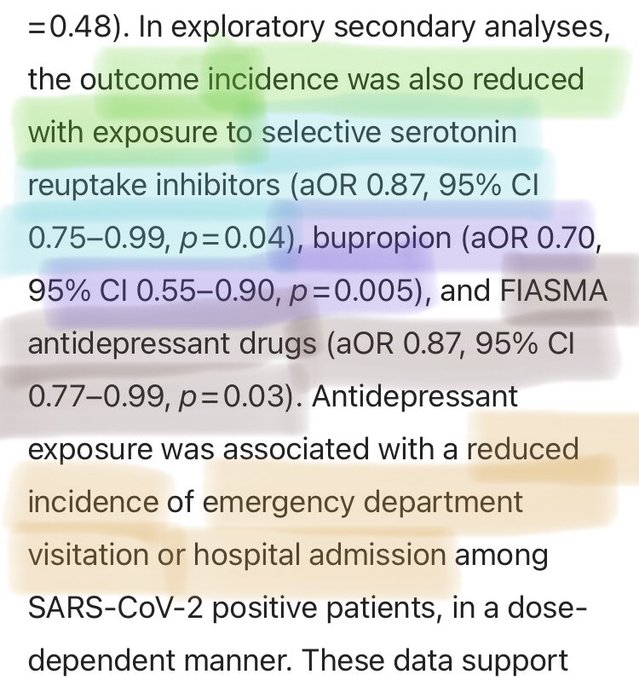
. It seems that any of several antidepressants can have protective effects against severe COVID outcomes (ER visits, hospitalizations).
26
131
444
A few people requested that I re-post a link to this article I wrote for Cerebrum magazine. It describes how I got the idea to use fluvoxamine as a treatment for COVID-19.
46
169
427
I wonder how many long haulers are having this problem: "It was found during sleep studies on [post-acute COVID] patients...that the REM phase of sleep no longer restricted movement, which wakes you up."

14
101
320
More information about potential effects of melatonin on COVID-19.

13
92
274
One reason I am disappointed in FDA decision about fluvoxamine EUA is the difficulty in getting COVID diagnosis within first 5 days of illness, when Paxlovid should be started. Even for doctors like me, this can be tricky. Initially thought it was allergies + long-COVID symptoms.
23
19
261
Doctor Submits Fluvoxamine EUA Application to FDA | MedPage Today

12
76
237
Today NIH updated their COVID treatment guidelines to mention SC2 and TOGETHER Trials. They have not adjusted their stance on fluvoxamine. They still do not recommend either for or against fluvoxamine for COVID. Disappointing that they have not changed recommendation to “for”.
19
40
240
I think Paxlovid+fluvoxamine worked very well for my acute COVID episode. Day 10 now. Off Paxlovid past 2 days. Feeling good, like my long COVID baseline (not like acute illness or long COVID flare). Continuing fluvoxamine & famotidine. Decided to also add some lactoferrin.
30
40
229
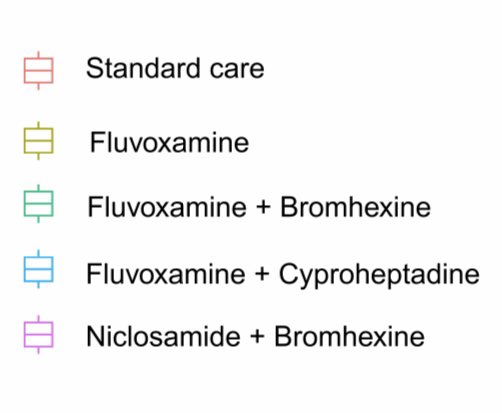
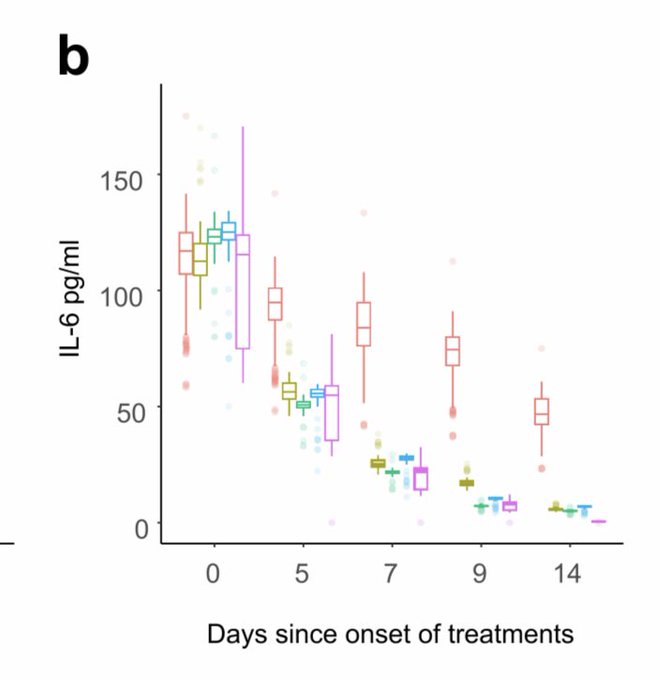
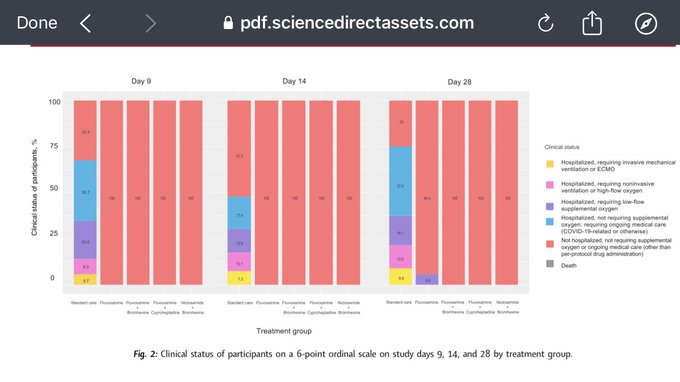
Replication of fluvoxamine's benefit for treating acute COVID-19, in Thailand. There is also evidence from this study that fluvoxamine prevents long COVID symptoms:
Early treatment with fluvoxamine, bromhexine, cyproheptadine, and nicl...
16
78
232
Old drug fluvoxamine, new hope for COVID-19 | SpringerLink

24
153
204
Just watched this. I have not been totally convinced that ivermectin works as well as some people think it does, but there is enough evidence for it and low enough risk of harm from the drug, that this should be taken seriously.

H-Hour: 0900, D-Day: 6/1/21
Tuesday, 9am Pacific, I will be talking live in the DarkHorse studio with
@PierreKory
of FLCCC /
@Covid19Critical
on the pandemic, the care of COVID-19 patients and the multidimensional campaign against Ivermectin. Buckle up...
241
1K
3K
27
44
192
Nice WSJ article about fluvoxamine.

9
61
180
Antidepressant prevents most serious COVID-19 complications - Futurity

9
58
179
This meta-analysis is now published: Ivermectin for Prevention and Treatment of COVID-19 Infectio... : American Journal of Therapeutics
7
76
175
More evidence that fluoxetine may have a protective effect against bad outcomes in patients with COVID-19.
13
53
175
“We know that when you have the COVID infection you have trouble breathing and that’s because there’s infection in your lung, but an additional explanation is that the virus enters the respiratory centers of the brain and causes problems there as well,” l
11
64
175
I think the reason I got sick again is because whatever variant I have is not easily taken care of by antibodies formed against previous variants or by vaccines based on those variants, and because hardly anyone cares about masking and social distancing anymore.
19
12
173
There is good evidence for treating COVID early with monoclonal antibodies and fluvoxamine. It is important to get the word out, so people who become ill will know they can talk to their doctors about treatment options.

@firasd
I don't think it's dishonest to say that there are innovative treatment options, I think it's just true! And while monoclonal antibodies in particular are highly effective, uptake isn't very high, which is part of why Covid is still a problem.
2
1
20
13
59
169
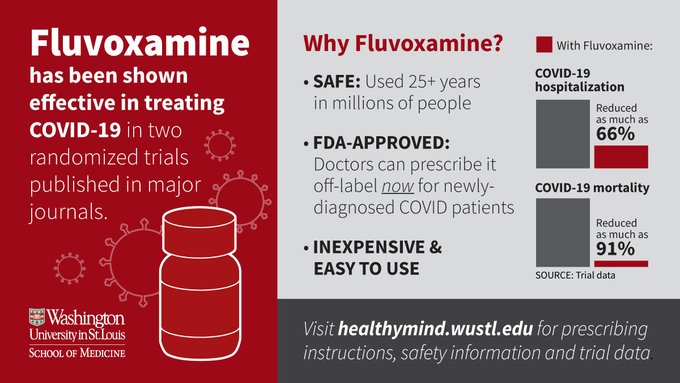
"In a secondary analysis of participants who took at least 80% of their pills...Risk of hospitalization or extended emergency care was reduced by two-thirds, and...[there was] a reduction in mortality risk of 91%."

11
73
160
Here is the new fluvoxamine fact sheet from Ontario COVID-19 Science Advisory Table. It contains useful information for prescribers and pharmacists.

13
61
162
ICU patients in Croatia taking fluvoxamine 100mg TID showed reduced mortality compared to matched controls.

4
48
148
I find it interesting that after I tweeted that I have acute COVID for 3rd time, there were a lot of appropriate supportive comments, and also some from individuals who seemed to make extreme assumptions about my vaccination status, in one of 2 opposite directions…
17
13
152
Interesting article about NAC.
N-acetyl cysteine: A tool to perturb SARS-CoV-2 spike protein conformation
10
54
145
Fluvoxamine EUA application has been submitted.

#IDTwitter
we submitted EUA Application for
#Fluvoxamine
for
#COVID19
to
@US_FDA
with the assistance of
@EricLenze2
@AngelaReiersen
@drklausner
@ShohamTxID
, and Ed Mills
If you want to sign a letter of support
(names are not public & will be reviewed)
14
43
139
12
37
144
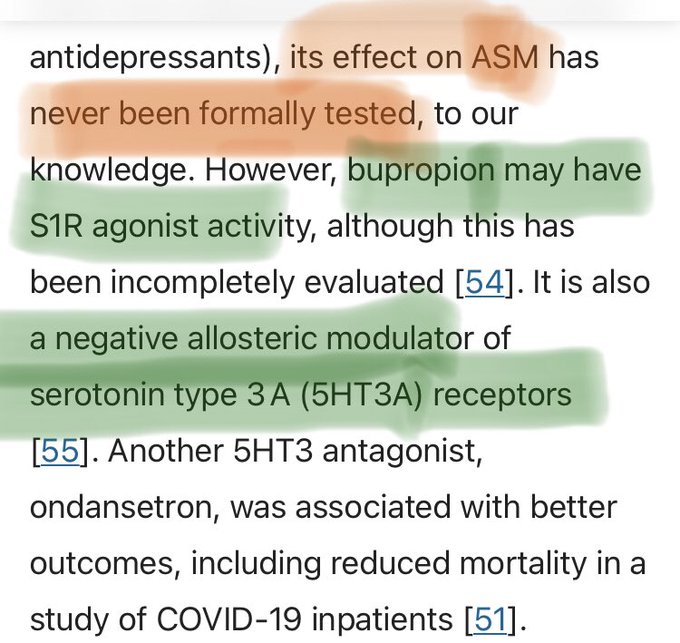
A surprise here was the statistically significant benefit of the dopamine and norepinephrine re-uptake inhibitor BUPROPION, which is not an SSRI, but might be a sigma1 receptor agonist, and is a negative allosteric modulator of 5HT3A receptors.
11
20
146
Majority of people in this study reported continued post-COVID symptoms 2 years after acute infection. This is not surprising to me based on accounts I've heard from individuals who had their first SARS-CoV-2 infection more than 2 years ago.
13
47
146
Our full paper on possible mechanisms of fluvoxamine in treating COVID19 has now been published in
@FrontiersIn
Pharmacology.

16
53
140
See this new article about fluvoxamine for treatment of COVID-19, including a video abstract which is available on the journal website.

8
52
131
Sotrovimab may be the only MAB that works against Omicron, but it is NOT “the only Covid treatment that works against Omicron”. Fluvoxamine can reduce clinical deterioration, emergency medical care visits, hospitalizations, and deaths.

11
43
135
Doctors can still prescribe fluvoxamine off-label, but it would best to have an official EUA from the FDA to support this. Not everyone can take Paxlovid, and it has problems like rebound. We need multiple treatment options.

9
31
126
Case reports on 2 COVID19 patients showing signs of serotonin excess & improving with cyproheptadine. If this is caused by platelet hyperactivation, an SSRI given early in the course of COVID19 could potentially prevent this.
@farid__jalali

Check out my published case reports on 2 patients with what appears to be an unprovoked serotonin-like syndrome in
#covid19
#medtwitter
please share
@TelehealthBot
0
22
48
10
35
129
This situation seem pretty bad, but there is a good COVID19 outpatient treatment option that many people are ignoring or have not heard about: FLUVOXAMINE.

2. Lack of Rx options. At least one of our mabs not effective vs omicron due to SGTF mutations and as
@EricTopol
points out in his new opinion piece we don’t have paxlovid in quantity
17
40
284
8
38
124
Check Interactions of COVID19 drugs with each other and with your other medications here.
24
47
121
1/ 4 years ago (3/17/2020), I first noticed symptoms of my first episode of COVID-19. About a week later, while experiencing the inflammatory phase, I thought of a possible way to prevent inflammation-related respiratory deterioration using an existing drug called fluvoxamine.
6
31
126
Column: With fluvoxamine, doctors find an old drug that may actually work against COVID-19

10
41
121
Article states, "In COVID-19 cases, the virus “hijacks” stress-response machinery, including sigma receptors, in order to replicate in the body. Interfering with that signaling appears to be the key...," but RCTs are still needed for these 2 compounds.

21
44
117
@Covid19Crusher
Increase in melatonin level may be one reason for fluvoxamine’s apparent benefit. Maybe they are even better given together.

4
34
106
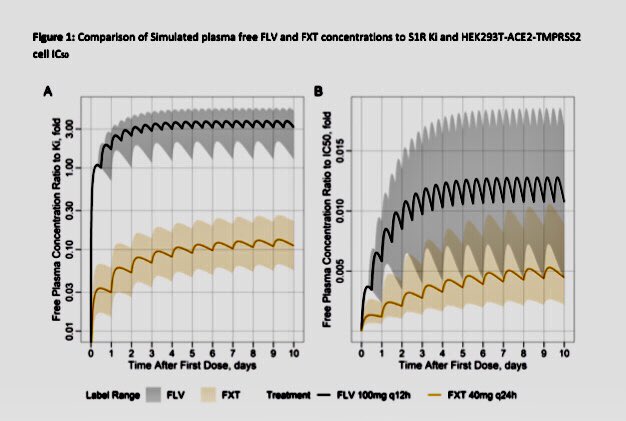
New publication including pharmacokinetic modeling of fluvoxamine & fluoxetine: Suggests fluvoxamine dose of 100mg BID may be ideal to ensure occupation of S1R, and fluoxetine level may not get high enough even at FDA maximum dose.
15
40
108

6
33
100
EFFECT OF EARLY TREATMENT WITH FLUVOXAMINE ON RISK OF EMERGENCY CARE AND HOSPITALIZATION AMONG PATIENTS WITH COVID-19: THE TOGETHER RANDOMIZED PLATFORM CLINICAL TRIAL | medRxiv

6
34
100
1/ Just in case any long haulers are interested: I had COVID 1st time March 2020. I think benefits of vaccination are greater than risks for many people, but I had recurrence of long COVID symptoms after the 2-shot Pfizer series (~Jan2021) so chose not to get mRNA boosters.
20
6
102
This article describes one mechanism that might possibly contribute to neurological symptoms of COVID-19: viral ORF proteins forming amyloid.

9
37
102
Important video about Ivermectin for treatment of COVID19. Includes description of a meta-analysis of mortality risk. Raises questions regarding WHO recommendations.
9
39
98
Effect of early treatment with fluvoxamine on risk of emergency care and hospitalisation among patients with COVID-19: the TOGETHER randomised, platform clinical trial

6
35
94
@amandalhu
Some pro-vax people are also anti-early-treatment for some reason. Sometimes when I post about COVID treatment research findings, some pro-vax people pop out and say they’d prefer to just get vaxxed. Getting vaxxed does not 100% prevent COVID. We need treatments too.
8
17
93
Some assumed I must have got sick a 3rd time due to being unvaccinated/unboosted, so not having strong enough immune response. Others though I must have got COVID a 3rd time because I WAS fully vaccinated/boosted and that this impaired my immune function. Both are wrong.
6
9
92
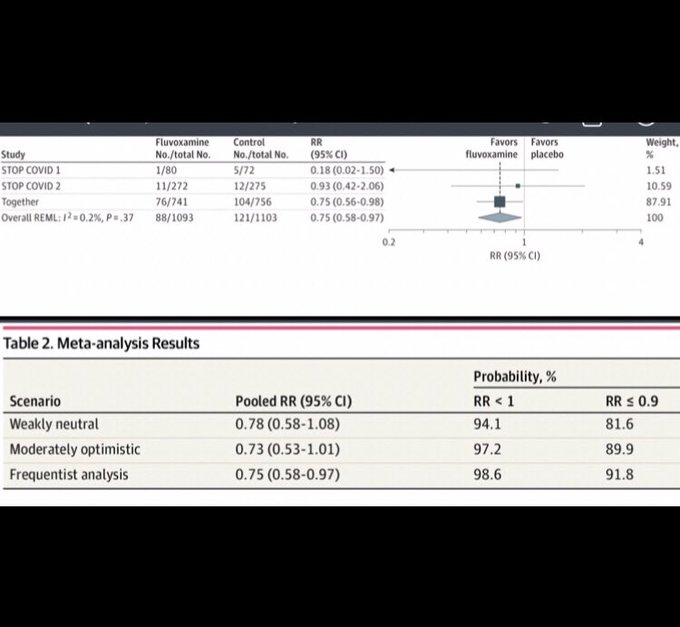
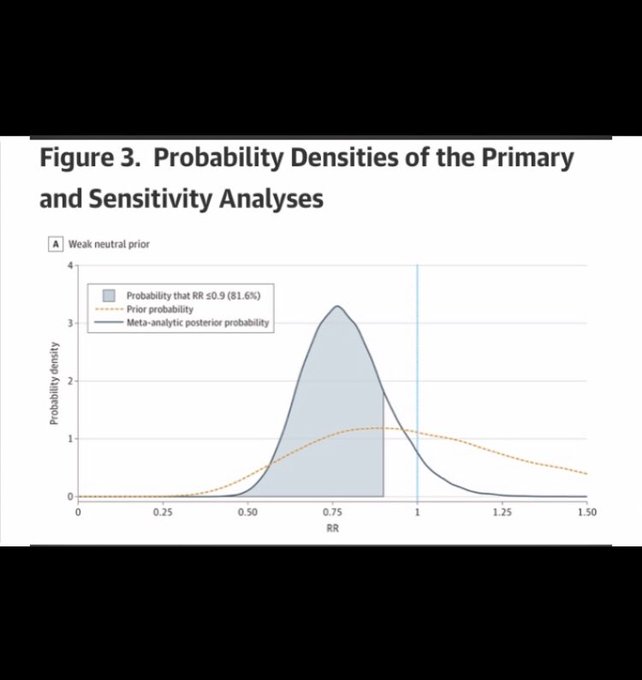
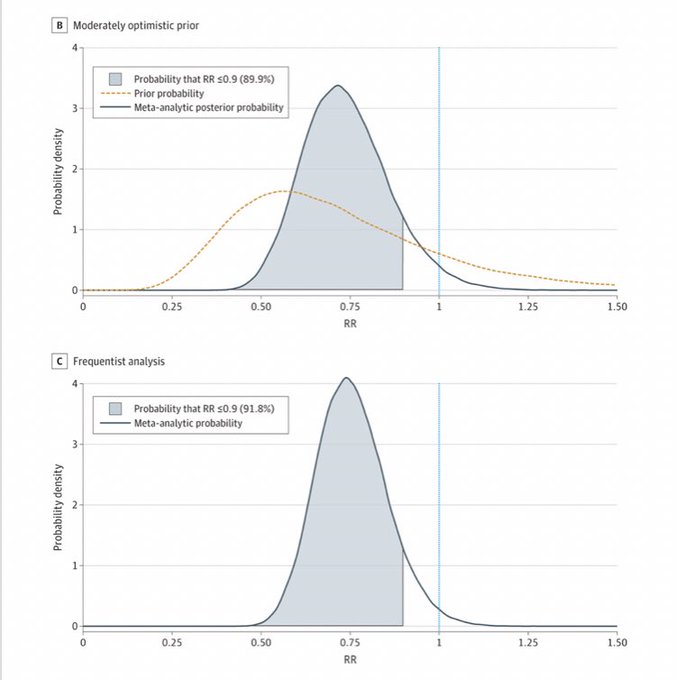
Meta-analysis has been published: Fluvoxamine for Outpatient Management of COVID-19 to Prevent Hospitalization via
@JAMANetworkOpen
part of
@JAMANetwork
3
23
90
Thanks to Sharyn Alfonsi and the
@60Minutes
@CBS
team for this excellent story about our fluvoxamine studies.
@EricLenze2
@WUSTLmed
#COVID19
#60Minutes
#fluvoxamine
COVID-19 research points to repurposed drugs

11
29
88
It’s great that Paxlovid will be available, but not everyone with COVID will be able to get it, at least not at first. Fluvoxamine can be prescribed off-label for outpatients with acute COVID NOW.

Pfizer said production of their pill takes ~6-8 months. The pill has to be taken within 5 days of first symptoms to be effective.
There is limited availability of the drug so patients at highest risk must be prioritized to receive these pills.
14
22
93
9
21
86
Blog entry: “Treatments for COVID-19” - from Harvard Health (includes section on fluvoxamine).
3
30
86
This is an important study by
@farid__jalali
and colleagues on platelets & serotonin in COVID19.
1
39
85
I know I already tweeted this article, but I think it is very good, so I am tweeting it again.
Fluvoxamine for Coronavirus

4
26
84
@EricTopol
@NatureMicrobiol
I'd be very interested in getting a nasal vaccine against this virus, especially if a nasal vaccine might be less likely than other existing vaccines to trigger autoimmune/inflammatory-related long COVID symptom flares.
4
6
86
My article is on page 9. It describes how I got the idea to use fluvoxamine as a treatment for COVID-19.
7
28
83
And remember, fluvoxamine increases melatonin levels, so this could have something to do with fluvoxamine's benefits as well.
3
9
83
I agree with this tweet by
@farid__jalali
. We need BOTH vaccines AND early treatment options for COVID.
19
18
82
Final version of our FIASMA article is now published online: Association Between FIASMAs and Reduced Risk of Intubation or Death in Individuals Hospitalized for Severe COVID‐19

10
34
76
So, if Paxlovid only “pauses” viral replication, and the course of illness can just continue on once Paxlovid is stopped, maybe it would work better if combined with something else that has a different mechanism.

@AngelaReiersen
@DrSyedHaider2
@drbeen_medical
@ichudov
@Aguirre1Gustavo
@DarrellMello
@drakchaurasia
@Canal1point5
Summary seems to be that Paxlovid simply pauses the viral replication process - once it wears off - in 2-8 days the process continues - remnants in cells are used to synthesize whole live virus again
which has been reported to infect others again (!)
1
4
19
22
13
77
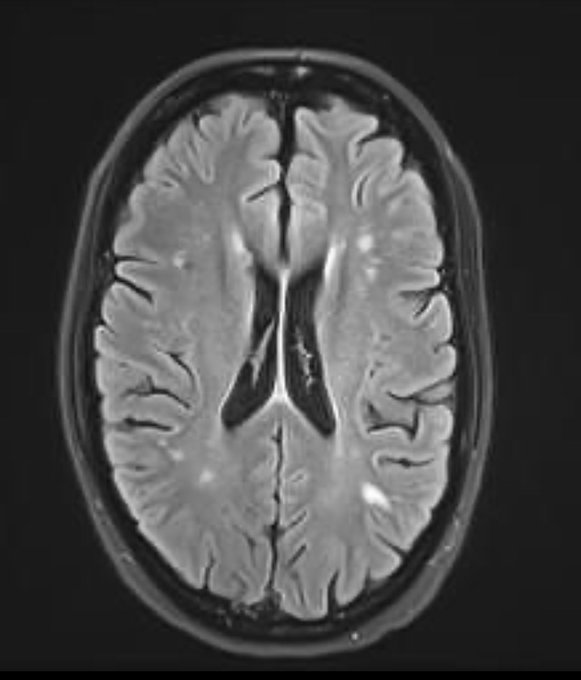
Example of “COVID brain”.
I advise trying to avoid getting COVID for as long as possible, at least until we know more about methods of preventing and treating lasting effects of the disease. Research is in progress, but we still don’t know enough about this.

Want to see what a “COVID Brain” can look like?
Here’s mine. The white spots are not supposed to be there. You can’t see the microhemorrhages or swelling.
Infected early March ‘20- pre-vaccine.But the threat is still here for everyone-vax or not, young or old.
Please mask up.
105
1K
3K
14
34
78
@loofymectin
@LongTiredRoad
@BernieDogs4
@farid__jalali
@AlisaValdesRod1
I think it is very likely that many people with long COVID have hyper-activated platelets which periodically release large amounts of serotonin. SSRIs can prevent platelets from loading up on serotonin, but that will take time since some platelets would be fully loaded already…
9
15
79
Fluvoxamine for Coronavirus | Science | AAAS
Nice quote from the article:”This is good news, since the drug is cheap and widely available, and I hope that this news is immediately affecting clinical practice”
6
23
78
@ShaneyWright
Maybe I can talk to some of my WashU ophthalmology colleagues and see if they are interested in looking into this.
2
1
76
I submitted a comment on our STOP COVID follow-up data to the JAMA network website, alongside the 2-year COVID follow-up article by 'César Fernández-de-las-Peñas' and colleagues. See the comments tab.
2
12
75
With COVID cases increasing again in some places, it is time to spread the word about fluvoxamine (again).

Stream episode Fluvoxamine for COVID-19, with Dr. Angela Reiersen by COVID Unfiltered podcast | Listen online for free on SoundCloud
0
4
10
6
18
75
@frothtimus
@farid__jalali
EUA application for use of fluvoxamine to treat early COVID was submitted to the FDA, but it could take months for FDA to review that. Omicron is here now, so it makes sense for doctors to just go ahead and prescribe it off-label now, at least for certain high-risk patients.
5
15
74
Fluvoxamine may help prevent severe overloading of the hospitals during this Omicron surge if physicians choose to prescribe it for appropriate high-risk patients.

4
25
74
@Canal1point5
@SerpinaLonghaul
@YochaiReemMD
@MrsProctor2010
@PeterHotez
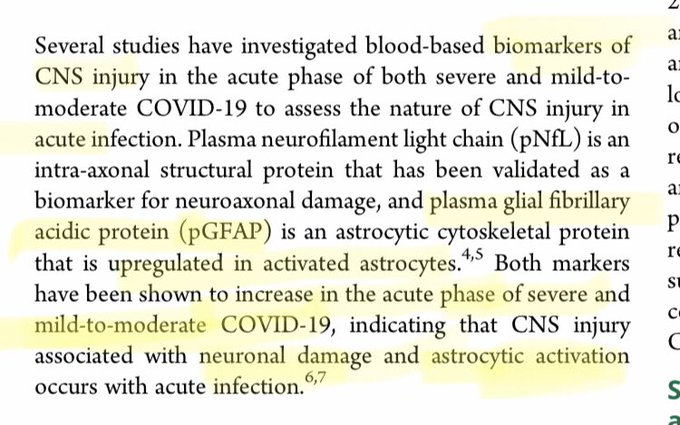
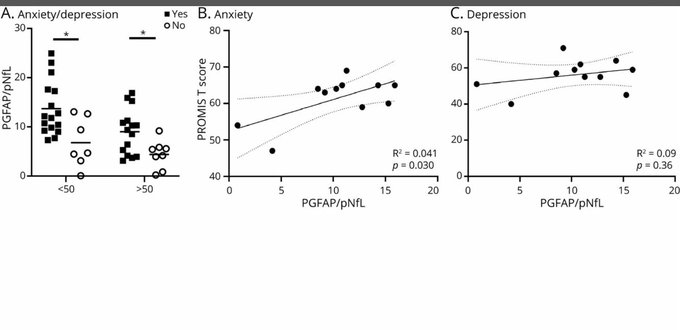
In this study, long COVID patients with higher “anxiety” tended to also have higher evidence of neuronal damage. So, high anxiety should be a reason to assess and address the neurological dysfunction that could be causing the anxiety.
4
22
72
@MVGutierrezMD
@PutrinoLab
This is true. I had COVID 3 times, Acute COVID symptoms were not as bad 2nd and 3rd time, but long COVID gets worse after each re-infection and then gradually improves to near-baseline over 5-6 months each time. I have heard similar stories from other people.
5
14
73
I think I probably have a strong (maybe even overly strong) immune response to the viral antigens my body has seen, due to both past infections and the Pfizer 2-shot series, but the virus keeps mutating, and is good at evading the immune system, So, none of this was adequate.
1
2
72
Bupropion may be a S1R agonist. This may contribute to its antidepressant activity and also to its apparent benefit in COVID-19. It would be great to see COVID-19 RCTs testing bupropion.

2
5
73
Final article now published in issue: Association Between FIASMAs and Reduced Risk of Intubation or Death in Individuals Hospitalized for Severe COVID‐19: An Observational Multicenter Study - Hoertel - 2021 - Clinical Pharmacology & Therapeutics -Wiley
5
20
70
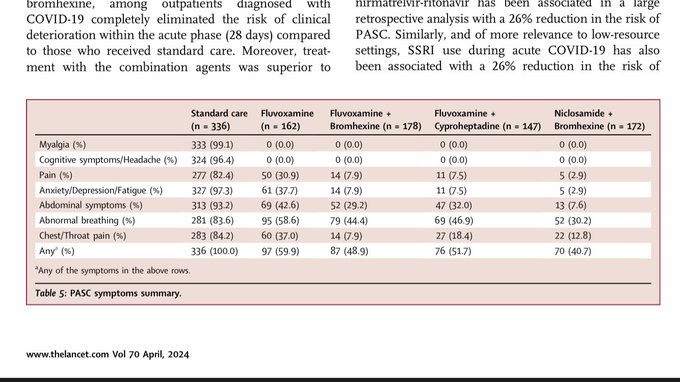
And there is also evidence from an observational study that SSRIs may reduce the risk for long COVID.
"...28% reduction in risk of PASC was observed for S1R agonist SSRIs and a 25% reduction in risk of PASC was observed for non-S1R agonist SSRIs..."
3
17
70
@LongTiredRoad
@AlisaValdesRod1
Also, many people with severe acute COVID have antibodies to serotonin 5-HT2A receptors, and these antibodies may activate those receptors as if they were serotonin. In this case a drug blocking that receptor (perhaps cyproheptadine or mirtazapine) might help.
5
15
68
@fasc1nate
@Ultracaustique
Here's what spicebush swallowtail caterpillars do if you tap them on the back. They stick put this weird Y-shaped smelly appendage that looks like a snake's tongue.
5
3
64
We need more COVID treatment options like fluvoxamine, especially considering the treatment-resistant COVID variants that have emerged. I'm glad to see that Platforma Catracha has been proactive in providing evidence-informed early COVID treatment for the people of Honduras.

Drug-evasive COVID variants are spreading globally. Very proud of our Fluvoxamine paper showing the world a safe and available option for all patients . Specially for those living in LMICs.
0
10
16
9
14
70
@dr_leshan
@farid__jalali
Will be nice to see the full results. I do think timing of treatment may be very important with fluvoxamine. Easier to stop inflammation before it gets far enough along to do significant damage.
4
11
67
PCPs: It really is a good idea to treat outpatients with COVID very early! You might even be able to help prevent overloading of ERs and hospitals!

Yes. Inhaled budesonide is in a similar situation. Dear doctors, *please* considering using fluvoxamine and/or inhaled budesonide to treat your high-risk covid outpatients. The randomized trial data are very, very clear on these two.
6
22
91
8
10
69
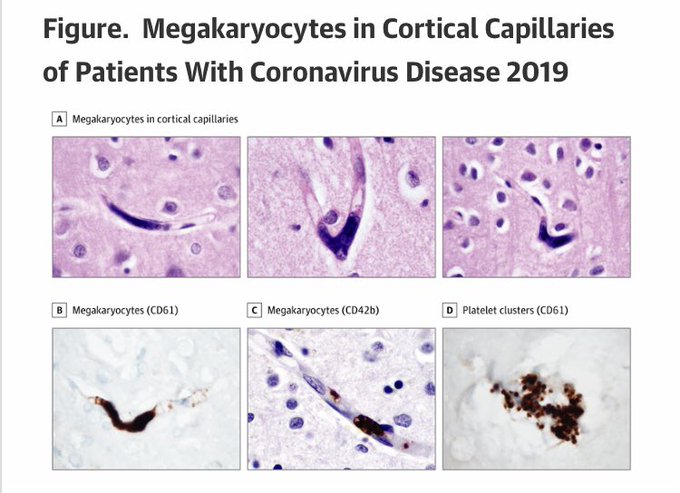
What are all these megakaryocytes doing in the brain capillaries of COVID patients?
5
32
67
I'm discussing “Mechanisms of Repurposed Drugs for COVID19” with
@PierreKory
,
@DrRomie
, and 2nd Time Around. Saturday, Jun 12 at 9:00 AM CDT on
@clubhouse
. Join us!
18
18
64
Long-haulers who have had Novavax:
What is your experience with Novavax vs other COVID shots? Do NOT answer unless you have (or have had) Long COVID and have had Novavax.
SE=acute vaccine side effects (1st 2-3 days after shot), LC=long COVID symptom status since shot.
less SE, LC improved
31
less SE, LC stable
29
less SE, LC worse
3
same/worse SE, LC worse
9
14
27
66
Interesting. The fluvoxamine mechanism described here is a type of antiviral mechanism requiring only low concentration of drug, which might explain why low dose would be effective for very early treatment.

2
18
64
1/ Here's an interesting paper. Seems that spike protein binds to lipopolysaccharide (LPS), which triggers inflammation. This is very consistent with my hypothesis that fluvoxamine's benefit for treating COVID involves activation of the S1R, which reduces cytokine production.
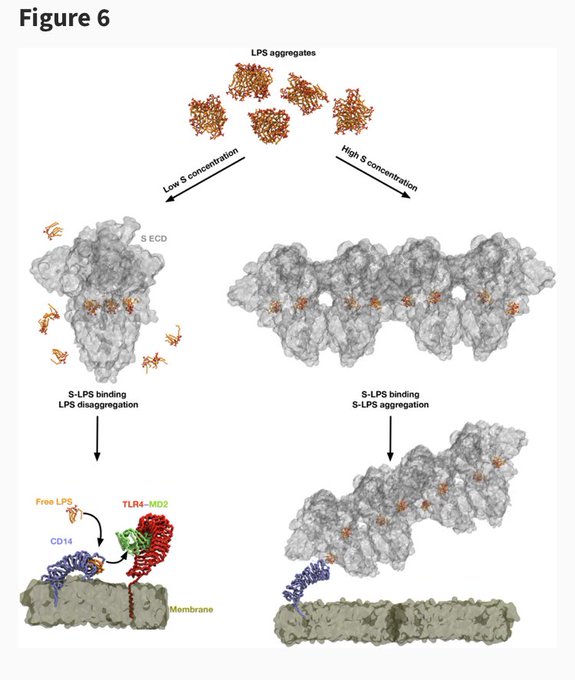
3
16
66
Well, I worked hard, along with
@EricLenze2
and many others on our STOP COVID 1&2 teams, but it was Ed Mills & his
@TogetherTrial
who ultimately got fluvoxamine over the line.
7
8
63
Study suggests very early treatment is needed to detect antiviral treatment effects (or else need huge sample size): Detection of significant antiviral drug effects on COVID-19 with reasonable sample sizes in randomized controlled trials: A modeling study

7
22
62
It looks like I never actually retweeted this, even though
@__ice9
requested all followers to do so, and I think this is potentially very important. Better late than never.

To all of my supposedly 7500+ followers (bots and dead accounts notwithstanding)--
I have one request:
𝗥𝗘𝗧𝗪𝗘𝗘𝗧 𝗧𝗛𝗜𝗦
It is the most important thing I have ever written.
Every critical care physician who reads this and understands it is worth decades of life saved.
23
224
188
1
14
64
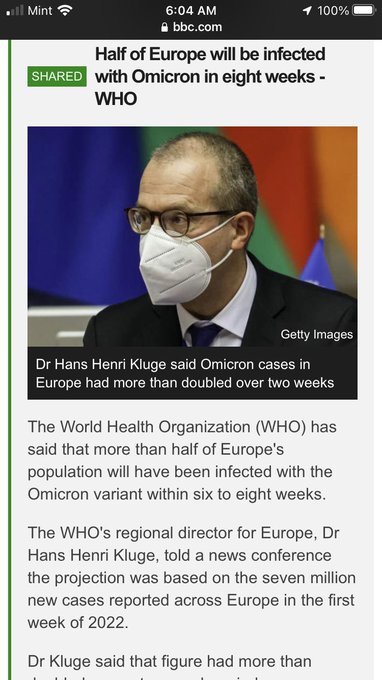
I’m thinking we really need to accelerate trials of existing drugs repurposed to treat COVID. Vaccines may not be enough to get this under control any time soon.

Mutations of mutations ...
Now a new UK variant has BOTH the increased ability to infect people like B117 and the changes to the spike protein giving it the ability to evade vaccines 50% of the time like E484K ...
"I feel the need, the need for speed"
7
19
34
9
16
65
@Canal1point5
@SerpinaLonghaul
@YochaiReemMD
@MrsProctor2010
@PeterHotez
In other words, anxiety should perhaps give stronger reason for proper assessment and treatment of potential CNS damage, rather than a reason to discount a long COVID patient’s symptoms as being caused by anxiety.
4
8
63
@nihillmatic
Did not take fluvoxamine for the first infection in March 2020. I thought of the idea while sick, but it was just a hypothesis at the time. I did take fluvoxamine the other 2 times. Also been taking it for long COVID, and I increased to max dose for acute COVID. Seems to help.
10
5
62
@richardemoe
@eongmobl
@loofymectin
@drbeen_medical
@EduEngineer
@Same_Sarikei
@Covid19Critical
@chrismartenson
@DrTessaT
@fynn_fan
@DCGreenZone1
@farid__jalali
@deNutrients
I believe in evidence-based medicine, but some EBM proponents look at mortality results like this and interpret this as evidence for NO effect because p-value is not less than 0.05, even though the point estimate suggests there most likely is an effect, but study has low power.
6
11
61
Real-world success with early use of repurposed drugs for treatment of COVID in Honduras. One predictor of worse outcome was if fluvoxamine was not given early enough in course of illness (started after 4 days).
5
14
61
Medication for autoantibodies also effective for Long COVID

6
18
63
@star9girl9
@YoDoctorYo
Might help to tell your PCP fluvoxamine is in the Johns Hopkins treatment guidelines.
3
15
60
ICER:
“… committee votes 11-2 that the evidence is not adequate to demonstrate a net health benefit for molnupiravir over symptomatic care alone; Paxlovid and fluvoxamine receive more favorable votes”
8
16
60
Nice to see fluvoxamine showing up on more hospital protocols.
5
7
61