
Nanashī 🫀
@The_Nanashi_O
Followers
3,326
Following
846
Media
854
Statuses
20,967
I study ECGs and POCUS
England, United Kingdom
Joined February 2015
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
ENCOURAGE TO SAROCHA REBECCA
• 512040 Tweets
ALL EYES ON RAFAH
• 485405 Tweets
Dinero
• 184463 Tweets
#LovelyRunnerEp16
• 168450 Tweets
デカ女ブーム
• 160349 Tweets
NuNew Show At KCL
• 99412 Tweets
Meyer Habib
• 89391 Tweets
DeNiro
• 74929 Tweets
Blanche
• 49189 Tweets
التعاون
• 47799 Tweets
Sura
• 44878 Tweets
TayNew Fun Night LH🩷
• 44141 Tweets
Angela Rayner
• 41668 Tweets
PORC
• 35507 Tweets
Washed
• 34803 Tweets
Black Ops 6
• 34556 Tweets
Guiraud
• 32369 Tweets
KCL AWARDS BEAUTY QUEEN FAYE
• 27443 Tweets
Game Pass
• 25344 Tweets
재난문자
• 22297 Tweets
Eto'o
• 21109 Tweets
Faker
• 20133 Tweets
CRIMINALIZA FAKE NEWS
• 19981 Tweets
Las EPS
• 19953 Tweets
#星野源ANN
• 18264 Tweets
Dick Schoof
• 17763 Tweets
Lied to you
• 16893 Tweets
Ahri
• 16511 Tweets
De Luca
• 13829 Tweets
Thaisa
• 12874 Tweets
대남전단
• 10569 Tweets




















@dedoyinajayi
You don't apologise to gain forgiveness or feel good. You apologise to make the offended/wronged see that your actions are regretted and you're ready to right wrongs. Whatever response you get, as long as it is not "negative" MUST be "acceptable" to you.
26
286
4K
@dedoyinajayi
You most definitely should not be looking to control the outcome of your apology by expecting/demanding a certain feel-good response.
And, "it's OK" is as magnanimous a response as it gets.
6
35
324
@ojayfemi
@DGlaucomflecken
–7.5 here.
Let's just say, it's not been easy. I'm paralysed without my specs.
3
0
117
@drkeithsiau
Respiratory ran out of bed space and there's a history of something remotely gastroenterological from 10 years ago.
3
3
111
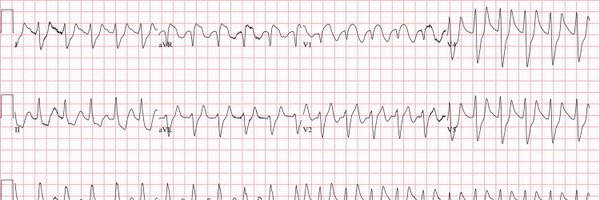
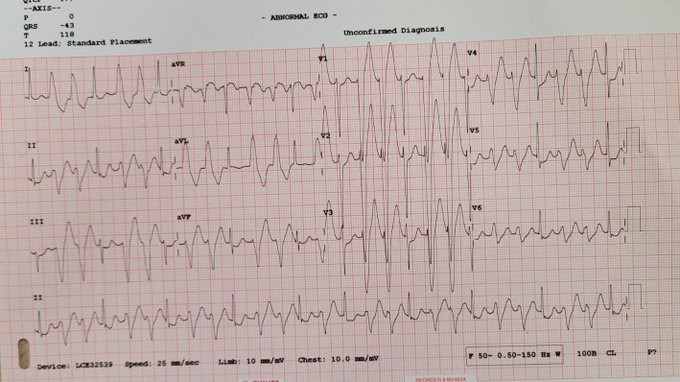
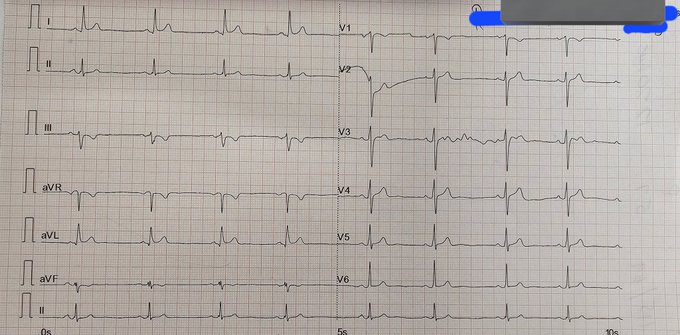
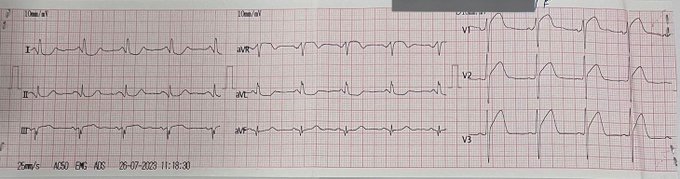
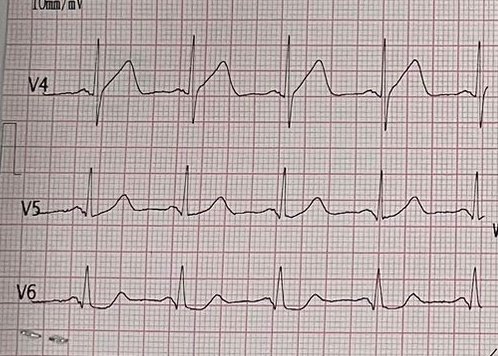
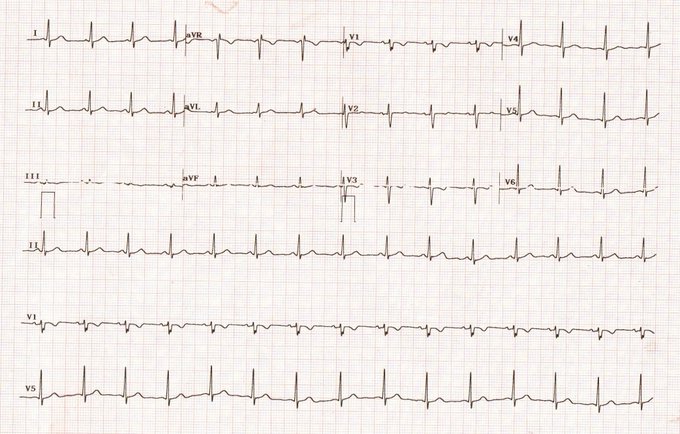
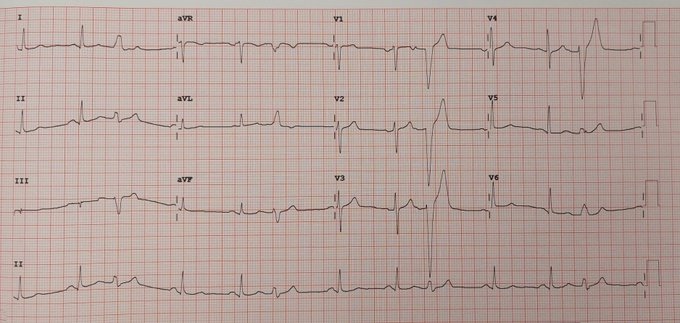
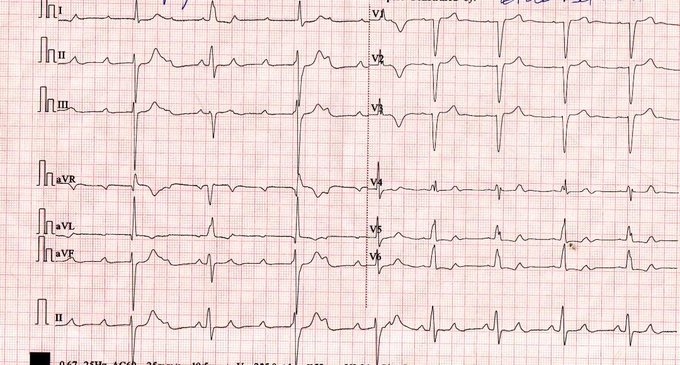
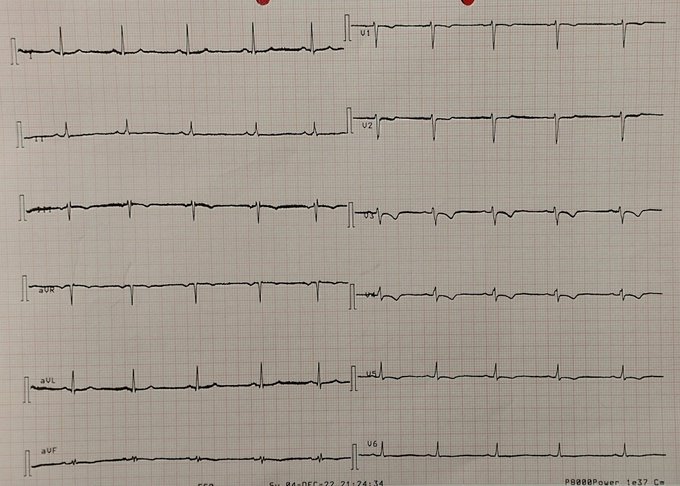
56/M with atypical chest pain. ECG recorded during pain.
@smithECGBlog
@BrooksWalsh
@AslangerE
@PendellM
@ekgpress
@EM_RESUS
@DidlakeDW
@ecgrhythms
@marioalrb84_a
@brun_dav
@MaruanCarlos
@UlhasDr
@Vadeboncoeur_Al
@RobertHermanMD
@cummingb1
@EMS12Lead
#ECG
16
25
93
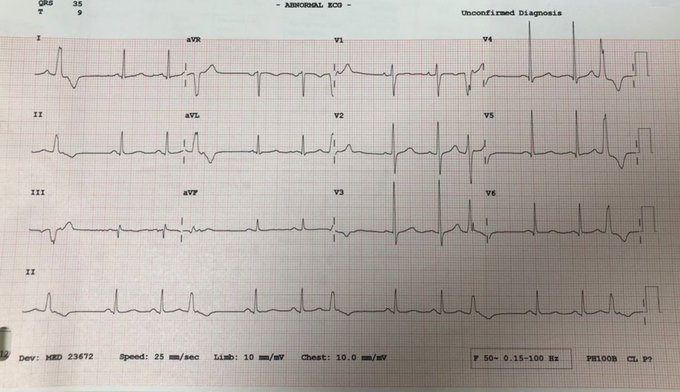
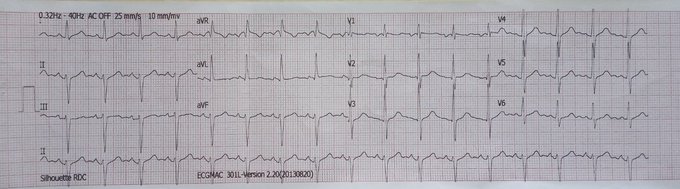
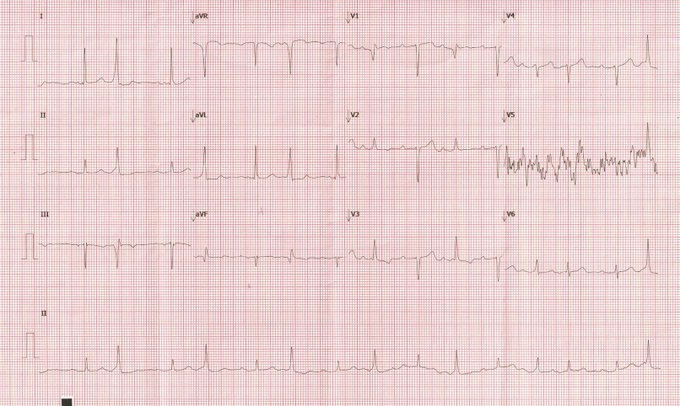
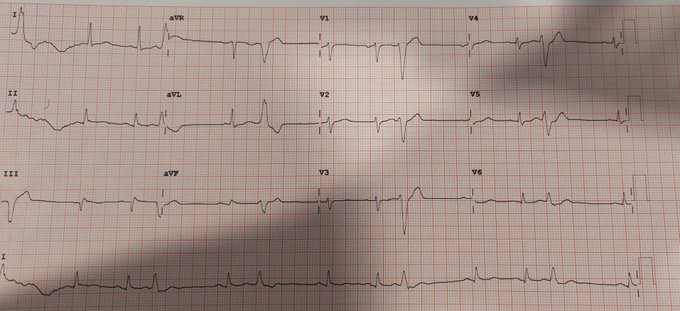
"Throat pain". Shared by a colleague.
#ECG
#CardioTwitter
#FOAMed
@smithECGBlog
@PendellM
@EcgOxford
@ecgrhythms
@MaruanCarlos
@Arron_Pearce_
@DidlakeDW
@BrooksWalsh
@EM_RESUS
@AslangerE
@RobertHermanMD

24
20
91

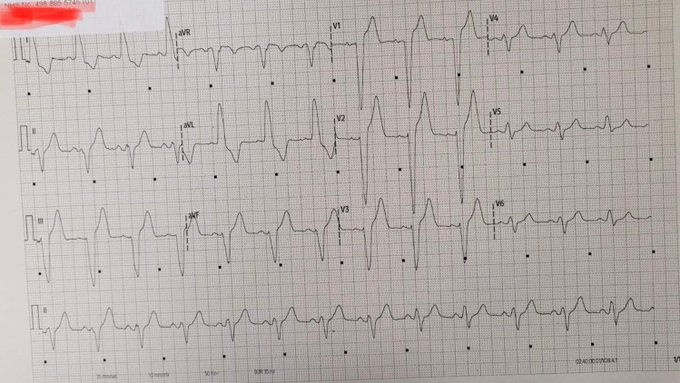
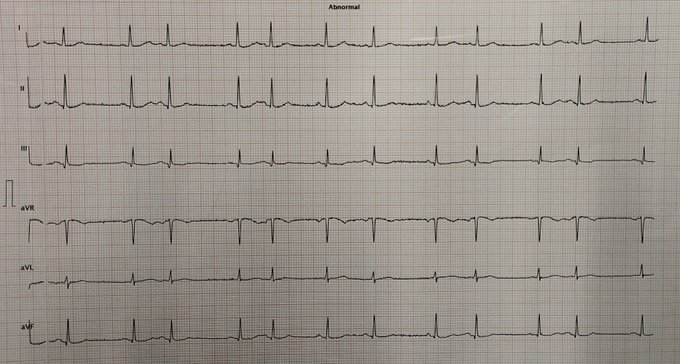
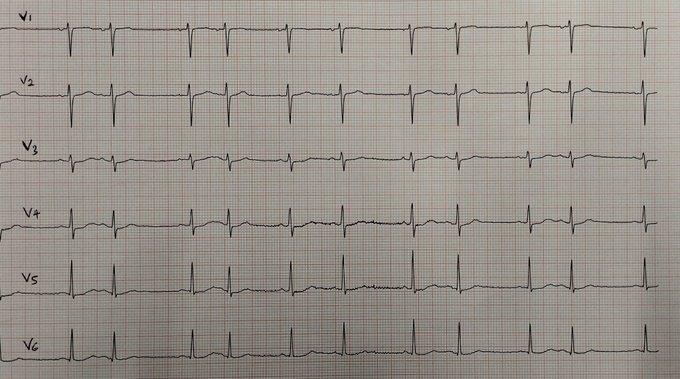
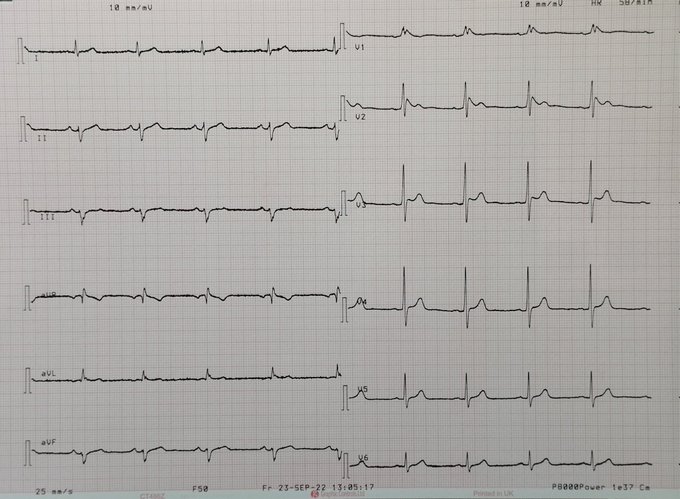
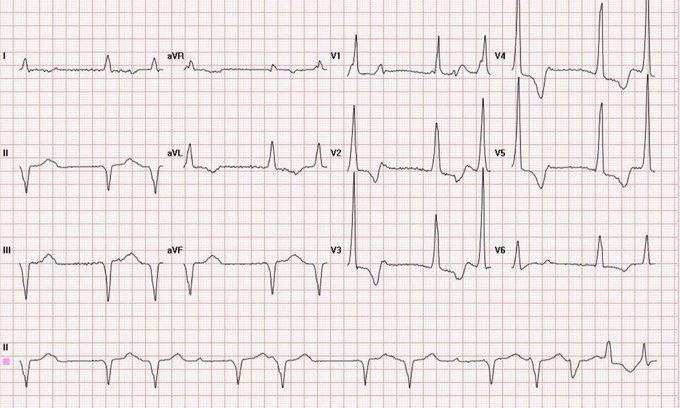
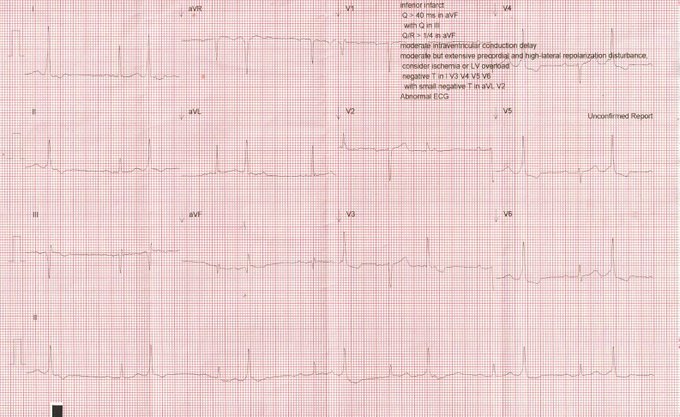
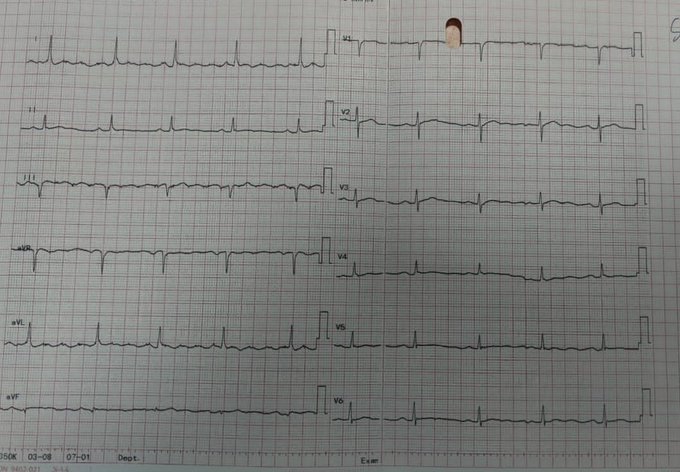
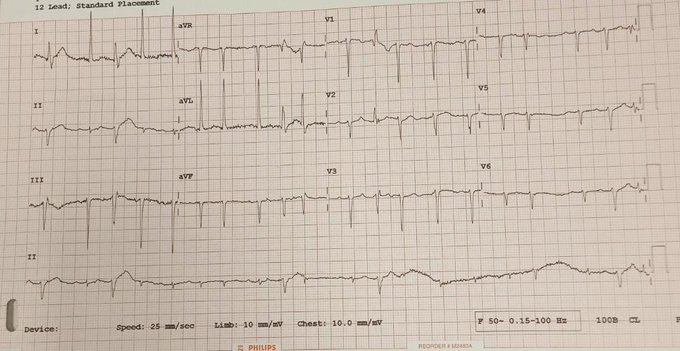
30-something hypertensive male with right-sided pleuritic chest pain for 1 week.
@smithECGBlog
@BrooksWalsh
@EM_RESUS
@brun_dav
@MaruanCarlos
@adribaran

19
11
70
@shifter_cat
@dedoyinajayi
Agreed!
If the offended responds positively, it is their graciousness that informs it. If the offender doesn't get a positive response, they are at the mercy of the offended. There are nuances to this, but this is the way of offence, forgiveness, and relationships.
1
0
65
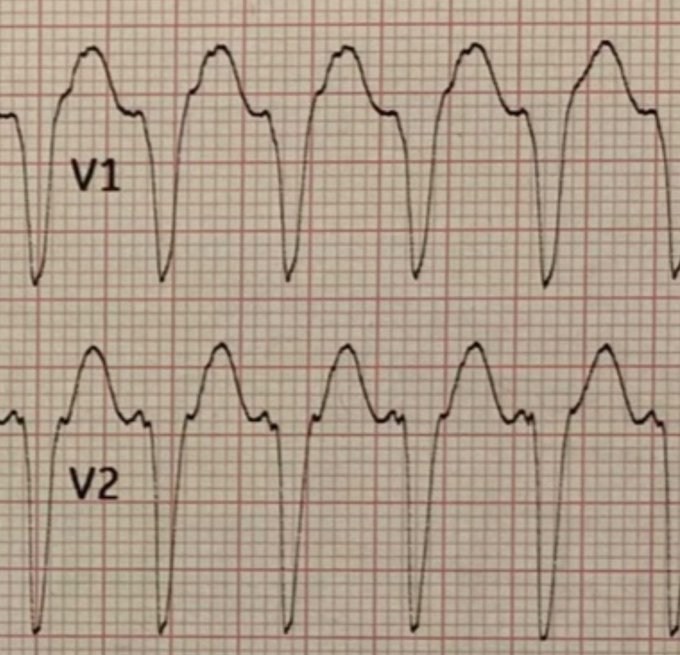
Thoughts on the rhythm? I was not provided the full 12-lead.
@DidlakeDW
@ekgpress
@BrooksWalsh
@adribaran
@Hapa_EP
@gerben_robbers
@ecgrhythms
@ECG_Emily
@smithECGBlog
@AslangerE
@EM_RESUS
@paramesh_mohan
@UlhasDr
27
8
62
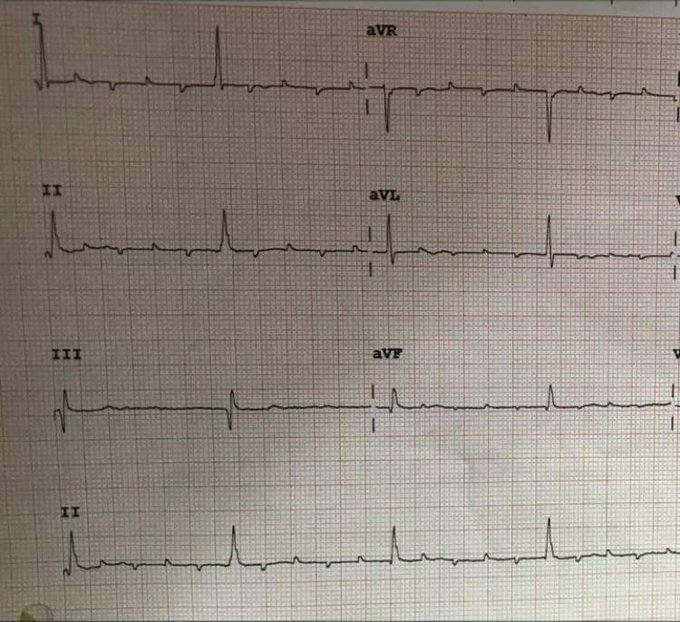
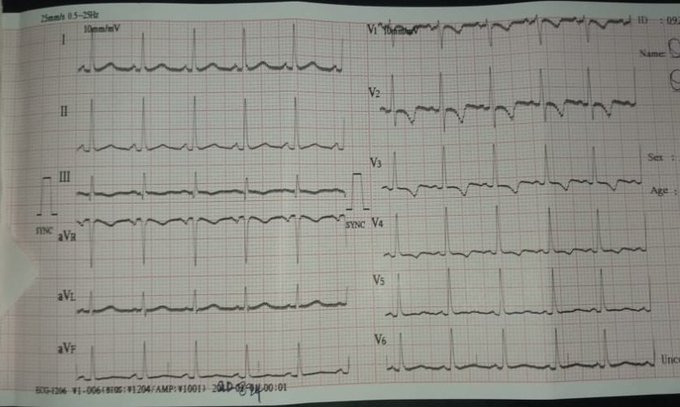
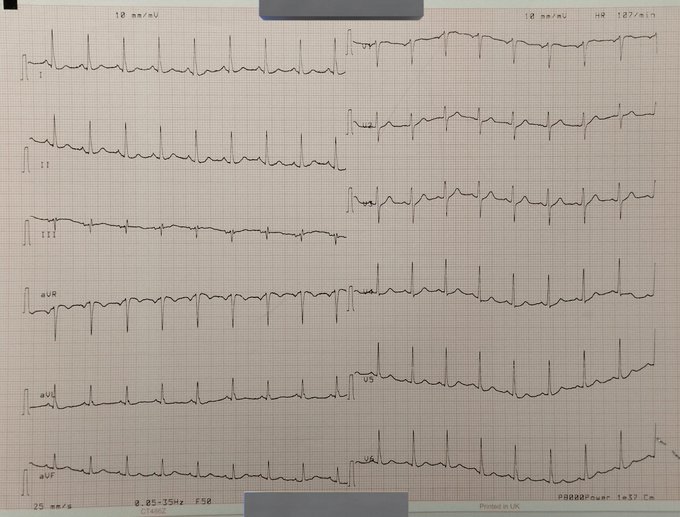
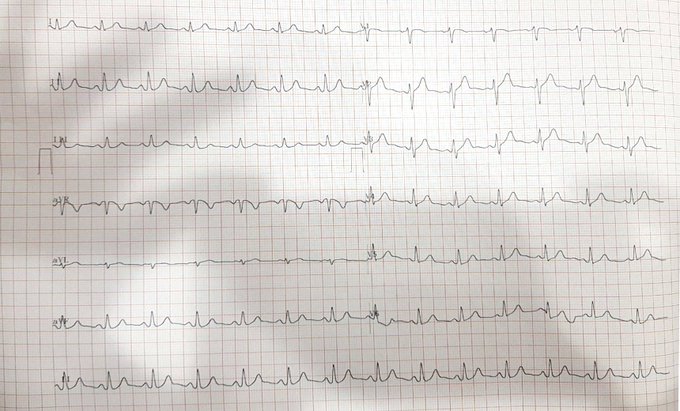
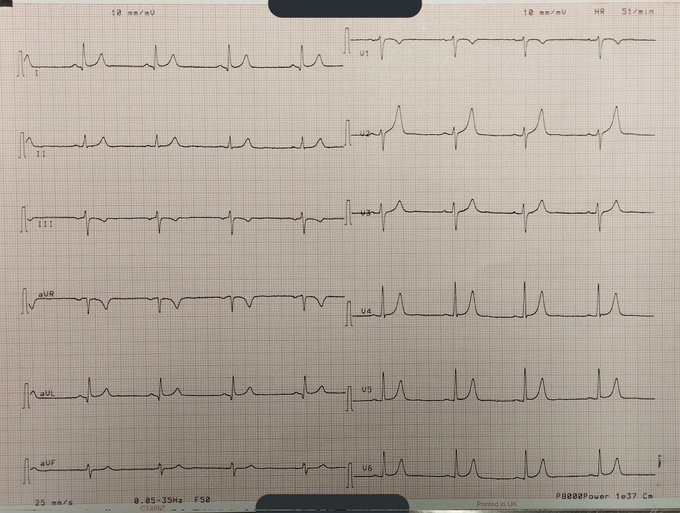
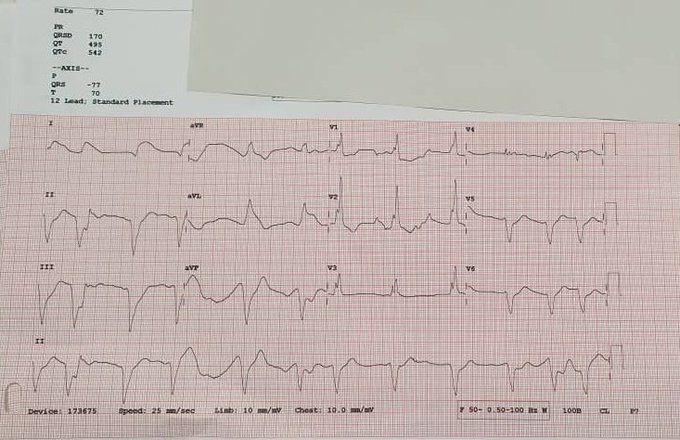
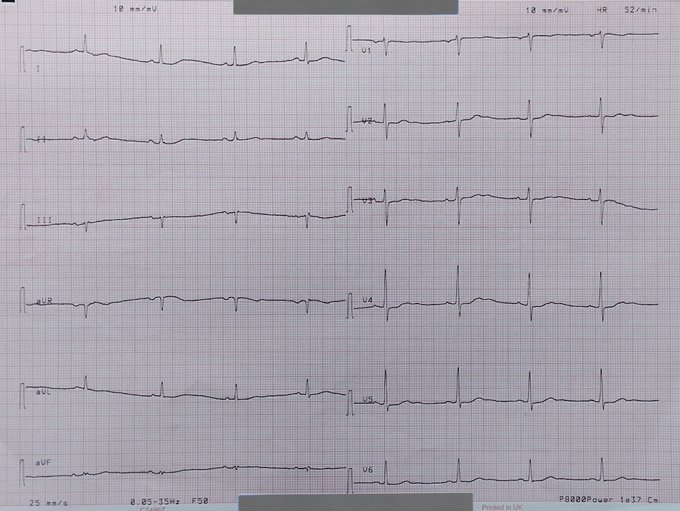
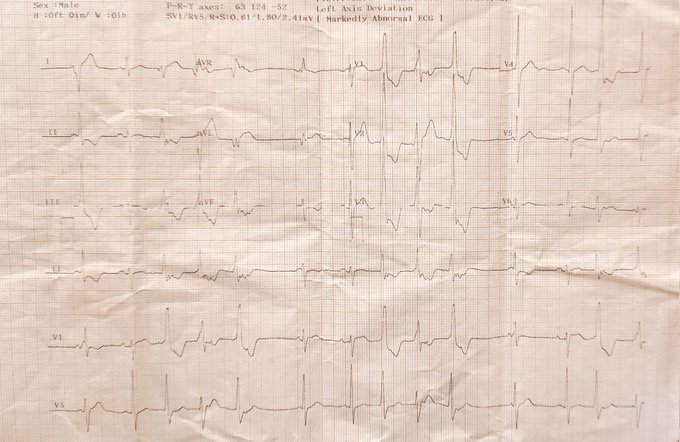
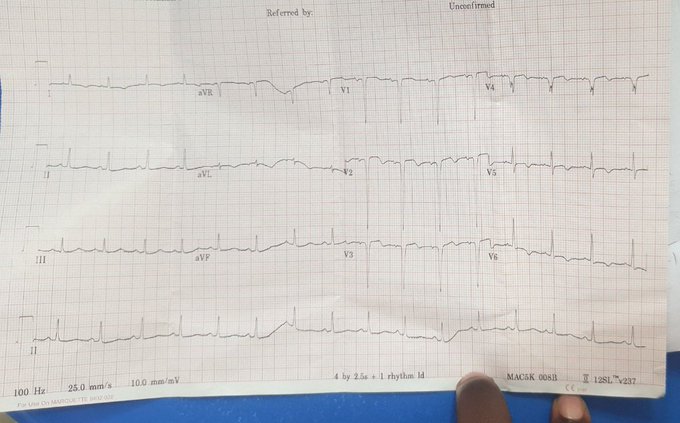
57-YO known hypertensive presented with tiredness, profuse sweating and headaches. BP 234/137 mmHg, PR 80 bpm. Thoughts?
Best picture sent to me. Please bear with me.
@smithECGBlog
@BrooksWalsh
@EM_RESUS
@brun_dav
@MaruanCarlos
@rob_buttner
@PacoDardon
@ecgrhythms
@AslangerE
17
12
58
@EM_RESUS
"Recorded immediately" should mean that we wait a while and get a repeat because the low-flow state/expected relative acidosis can produce all sorts.
If we had to take this one at face value, then the very wide QRS could be any sodium channel poison — ⬆️ K+, ⬇️pH, SCB meds, etc.
0
0
57
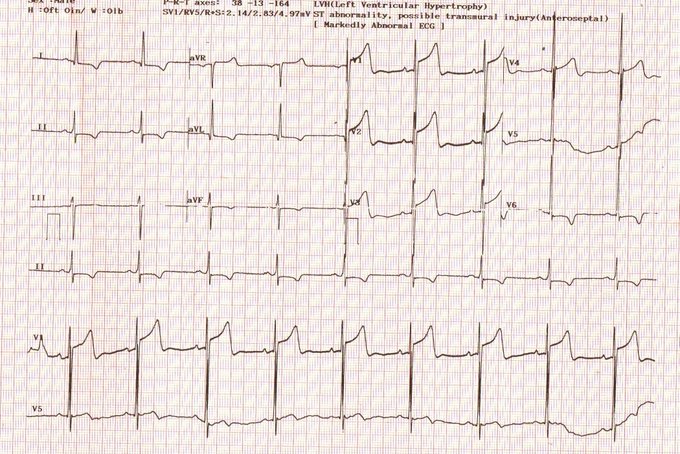
Middle-aged man with chest pain. What do we think of this?
@smithECGBlog
@EM_RESUS
@brun_dav
@MaruanCarlos
@BrooksWalsh
@ecgrhythms
@PacoDardon
@doctor_roig
@PendellM
12
16
54
@EcgsOnly
Good example of how PVCs can show acute ischaemia better than sinus beats.
Through the PVCs, we can see inferior, posterior, and lateral injury. We can also see anterior injury (TWs of PVCs in V3, V4) coupled with a suspiciously flat ST in V1 (sinus) to suggest a pRCA OMI.
1
4
52
75-yo female, HTN, with sudden-onset palpitations 3 hours prior. Thoughts on this?
@smithECGBlog
@BrooksWalsh
@ecgrhythms
@PendellM
@UlhasDr
@DidlakeDW
@gerben_robbers
@brun_dav
@MaruanCarlos
@FloydECGs
@anunay_cardio
@SchakrabartiEP
@syamkumarmd
@Hapa_EP
@AslangerE
16
11
49
Case from a colleague. Rhythm diagnosis?
1. Tachy
2. After Amiodarone
#EPeeps
#ECG
#CardioTwitter
@SergioPinski
@willyhfrick
@DidlakeDW
@Arron_Pearce_
@DaveRichley
@Hapa_EP
@adribaran
@ACH_epteam
@ecgrhythms
@ecgandrhythmRoe
@doctor_roig
@EM_RESUS
@smithECGBlog
@BrooksWalsh
12
22
48
A 32-year-old primigravida at GA 22 weeks with 2 episodes of sudden fainting spells and spontaneous recovery. Electrolytes are normal.
This was all the history I got.
@ecgrhythms
@ojayfemi
@BrooksWalsh
@EM_RESUS
@smithECGBlog
12
12
44
@EM_RESUS
Sodium channel blocker toxicity.
Take your pick between TCA overdose and hyperK+.
Sinus tachycardia and RAD tilts me towards TCA tox.
0
1
45
65-yo male with a history of intermittent palpitations of unknown aetiology. Location?
#EPeeps
#CardioTwitter
@syamkumarmd
@DidlakeDW
@BrooksWalsh
@smithECGBlog
@adribaran
@SchakrabartiEP
@Arron_Pearce_
19
8
41
@EM_RESUS
SR + qRBBB + Acute proximal LAD OMI pattern, until proven otherwise.
Old inferior injury.
Dissonance in the ST shift from V2—4 is probably due to high placement of V1, V2.
1
2
42
Middle-aged male with this pre-op ECG. What do you see?
#ECG
#CardioTwitter
#FOAMed
@ecgrhythms
@ecgandrhythmRoe
@BrooksWalsh
@Arron_Pearce_
@MaruanCarlos
@jeffrey_vinocur
@AThomazAndrade
@UlhasDr
@DidlakeDW
@MartowMartow
@ECG_Emily
@SergioPinski
@ekgpress
@Hapa_EP
15
14
40
@gerben_robbers
1. Kosuge's sign: with acute chest syndrome, TWI in V1 and III
1b. TWI in the chest leads will often involve V1—3 or 4
2. S1Q3T3
3. Tachycardia, typically sinus
2
5
41
Premature beats were labelled PVCs. Agree?
@ecgrhythms
@DidlakeDW
@BrooksWalsh
@Arron_Pearce_
@RobertHermanMD
#EPeeps
#ECG
#CardioTwitter
12
11
41
Rhythm diagnosis?
@DidlakeDW
@ecgrhythms
@BrooksWalsh
@Arron_Pearce_
@EcgOxford
@EcgsOnly
@ECG_Emily
21
9
42
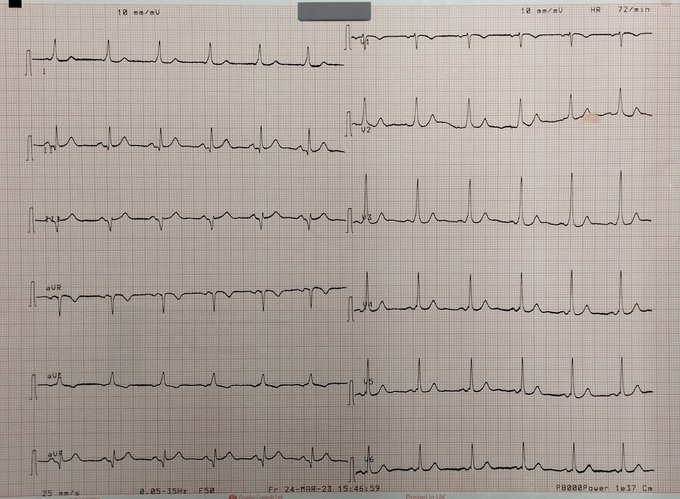
Persistent tachy. Computer says "sinus tachy". Agree?
ECG 1: 2wks ago
ECG 2: Today
#EPeeps
#ECG
#CardioTwitter
@SchakrabartiEP
@syamkumarmd
@MaruanCarlos
@brun_dav
@DidlakeDW
@ekgpress
@BrooksWalsh
@smithECGBlog
@adribaran
@ALFIEEP1
@SergioPinski
@Hapa_EP
@ecgrhythms
15
9
36
60-yo male with breathlessness and chronic cough.
@smithECGBlog
@EM_RESUS
@brun_dav
@BrooksWalsh
@MaruanCarlos
@EkgHacks
@ecgrhythms
@AslangerE
@ECGfan

9
8
38
From a colleague: 40/M with retrosternal CP. ECG 1 at t-0 and ECG 2 at t-5 hrs. Initial trops negative. Thoughts?
@smithECGBlog
@EM_RESUS
@BrooksWalsh
@PendellM
@TahaMD_EM
@MaruanCarlos
@brun_dav
@PacoDardon
10
7
36
49/M, HTN, walks with a c/o poor sleep over the past few weeks. No other symptoms.
Without the benefit of the history, would this be interpreted as AMI?
@PendellM
@BrooksWalsh
@smithECGBlog
@DidlakeDW
@ecgrhythms
@MaruanCarlos
@brun_dav
@adribaran
@FloydECGs
@TahaMD_EM
4
7
35
@RJS_med
First ECG was already diagnostic of inferoposterior OMI, in the right context.
Second looks more scary, but the first is no less real.
Either way, making it a habit to get serial ECGs is simply gold. 👍
1
1
37
A shared by a colleague:
40/M Obese. Rushed to the ER following a fall with faecal incontinence and altered consciousness, weak pulses, unrecordable BP, SpO² 96%, RBG 13.7 mmol/L.
@smithECGBlog
@BrooksWalsh
@EM_RESUS
@AslangerE
@DidlakeDW
@TahaMD_EM
@FloydECGs
@PendellM
12
8
36
23-yo female with central chest pressure of a few hours duration 24 hours after ingesting marijuana-laced cake.
@smithECGBlog
@UlhasDr
@ecgrhythms
@ekgpress
@EM_RESUS
@BrooksWalsh
@brun_dav
@MaruanCarlos
@TahaMD_EM
@syamkumarmd
@ECGfan
@PacoDardon
13
12
35
9
7
35
40-something male with near collapse and a history of syncopal attacks with associated seizures.
@BrooksWalsh
@smithECGBlog
@StephenRahm
@DidlakeDW
@ecgrhythms
@MaruanCarlos
@brun_dav
@EcgOxford
@AslangerE
@UlhasDr
@ECG_Emily
@EM_RESUS
@paramesh_mohan
@Jagdish26039718
15
10
34
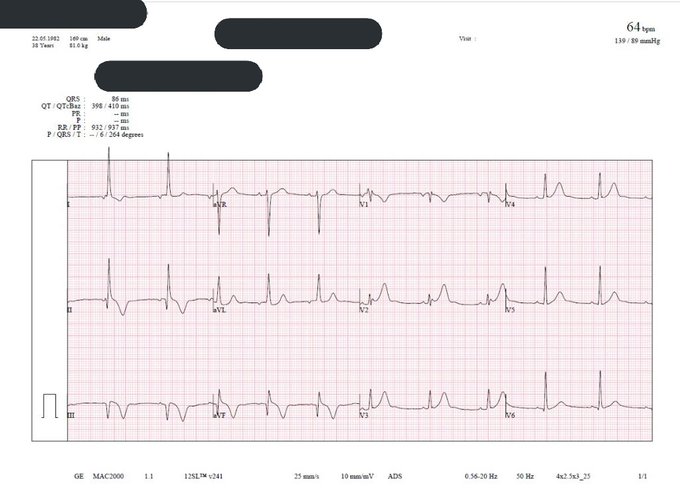
This was hyperK+ 8.0 mmol/L.
The TWs in the praecordial leads (not tall) have a narrow base than expected and the PRI is prolonged. Remarkably, the QRS complexes remain quite narrow (86 ms).
This was a case of obstructive uropathy.
What do you think?
#CardioTwitter
#ECG
#FOAMed
#EPeeps
@smithECGBlog
@PendellM
@BrooksWalsh
@DidlakeDW
@ecgrhythms
@syamkumarmd
@EM_RESUS

4
6
31
6
6
33
@EM_RESUS
Transmural injury pattern in the LAD territory. Given likely blunt force trauma to the chest (or maybe even penetrating), the possibilities are:
1. Myocardial contusion
2. Traumatic LAD/LM injury (dissection, rupture, etc)
3. A badly-timed thrombotic LAD OMI.
Contrast chest CT.
0
1
31
50s/M, asymptomatic. ECG for pre-op evaluation. K+ at this time, 4.7 mmol/L.
"Vagotonic ECG"?
@syamkumarmd
@BrooksWalsh
@MaruanCarlos
@brun_dav
@AslangerE
@DidlakeDW
@smithECGBlog
@ecgrhythms
@FloydECGs
@DaveRichley
@ekgpress
@ecgrhythms
@adribaran
@AThomazAndrade
@UlhasDr
18
6
30
Courtesy
@Rodrigue_Ekollo
Rhythm + other diagnosis?
@adribaran
@Arron_Pearce_
@AslangerE
@BonaJenn
@BrooksWalsh
@DidlakeDW
@EcgOxford
@ecgrhythms
@smithECGBlog
@ekgpress
@ECG_Emily
@SchakrabartiEP
@syamkumarmd
@EM_RESUS
@TahaMD_EM
#EPeeps
#CardioTwitter

12
13
31
@EM_RESUS
Acute proximal LAD or, less likely, LM occlusion. Q waves develop within the the first hour in ½ of MIs.
The presentation sounds like either LV dysfunction with reduced CO vs papillary rupture with MR and pulmonary oedema.
Activate Cath lab but quick echo just to see.
0
1
31
What do you think?
#CardioTwitter
#ECG
#FOAMed
#EPeeps
@smithECGBlog
@PendellM
@BrooksWalsh
@DidlakeDW
@ecgrhythms
@syamkumarmd
@EM_RESUS
4
6
31
28-yo female, 3 days post Caesarian delivery, with c/o sudden onset of breathlessness, intermittent palpitations dizziness, and vague chest discomfort. Vitals stable, RR 18, SpO² 98-99% in room air.
@BrooksWalsh
@smithECGBlog
@ecgrhythms
@DidlakeDW
@gerben_robbers
@EM_RESUS
17
8
30
75-yo male with no history of cardiovascular disease. PMH is only significant for dyspepsia. What do you make of this ECG?
@smithECGBlog
@BrooksWalsh
@ecgrhythms
@EM_RESUS
10
6
30
Courtesy
@Rodrigue_Ekollo
Had trouble figuring this one out because of the machine configuration.
NB: First 3 beats in the rhythm strip is reproduced in all 12 leads.
#EPeeps
#ECG
#CardioTwitter
@syamkumarmd
@MaruanCarlos
@Arron_Pearce_
@DidlakeDW
@DaveRichley
9
6
29
@docnadel
@ecgrhythms
@BrooksWalsh
@smithECGBlog
@ECGTalk
@SchakrabartiEP
@amalmattu
@EM_RESUS
@EMS12Lead
@ECGfan
@narrowQRS
@Basalus
Junctional escape rhythm with retrograde P waves whose repolarisation waves (Ta) — which are of opposite polarity to the PWs — cause a pseudo-ST elevation. We see the reverse in leads with an upright retrograde P wave. Praecordial leads look like old anterior MI.
3
4
30
@drkeithsiau
Waterhouse-Friderichsen syndrome?
Only thing I can tie adrenal failure to septic shock right now.
2
0
29
Out-of-hospital cardiac arrest. Thoughts?
@smithECGBlog
@EM_RESUS
@BrooksWalsh
@brun_dav
@MaruanCarlos
@rob_buttner
@ecgrhythms
@PacoDardon
@iustinianos
12
8
29
Courtesy
@Carlos_ROOV
60+/M with chest pain. *The rhythm is paced*
@smithECGBlog
@PendellM
@DidlakeDW
@BrooksWalsh
@jonnywatt
@ecgrhythms
@ekgpress
@EM_RESUS
@brun_dav
@RobertHermanMD
@MaruanCarlos
@AThomazAndrade
@Arron_Pearce_
#ECG
#CardioTwitter
#FOAMed

6
14
28
60s ♂️ with this ECG described as "mostly normal". Do you see anything abnormal?
1st ECG — 2½ months prior
2nd ECG (LLs and V leads) — today
#ECG
#FOAMed
#CardioTwitter
10
3
26
89-yo male with severe peripheral artery disease. No chest pain.
8
7
26
Asked about the likely site of origin of the PVCs. What do you think?
#FOAMed
#ECG
#CardioTwitter
#EPeeps
13
5
28
Asymptomatic gentleman
#ECG
#EKG
#EPeeps
#CardioTwitter
@DaveRichley
@Arron_Pearce_
@BrooksWalsh
@MaruanCarlos
@DidlakeDW
@willyhfrick
@ekgpress
@ecgrhythms
6
8
27
@EcgsOnly
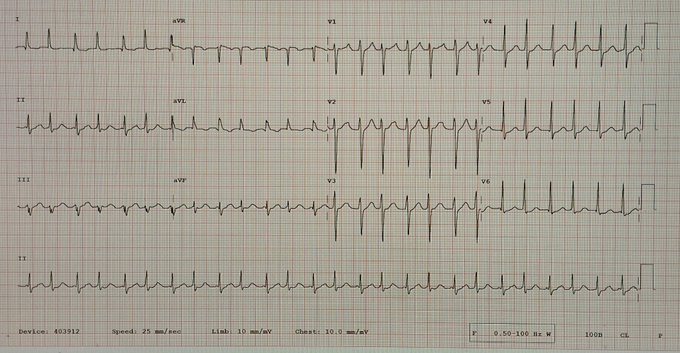
2:1 AFL/AT with LBBB-type aberrancy. Leads V1 and V2 show both sets of flutter/atrial waves.
One just before the peak of the T and another just before the next QRS complex.
1
2
27
True or pseudodelta wave? PRI is 112 ms and QRSd is 88 ms.
@BrooksWalsh
@MaruanCarlos
@smithECGBlog
@UlhasDr
@narrowQRS
@brun_dav
@ecgrhythms
@ECGfan
@TahaMD_EM

8
5
26
@EcgsOnly
Brugada pattern in V1 and V2 and in aVL (extra-praecordial manifestation) + the history = BrS.
When's the ICD going in?
3
0
25
Came across this ECG in a stack. Only medical history available is hypertension. What do we think?
@smithECGBlog
@BrooksWalsh
@brun_dav
@MaruanCarlos
@ecgrhythms
@TahaMD_EM
@ekgpress
@EM_RESUS
9
8
25
@SergioPinski
1. LA/LL lead reversal
2. AFL/AT (sawtooth, so obviously AFL more likely)
3. Complete LBBB
4. Bi-level AV block — 2:1 at the upper level and 3:2 at the lower level with Wenckebach periodicity (giving a cumulative 6:2 AV conduction pattern)
0
0
25
@ecgandrhythmRoe
4 reasons:
1. RV injury
2. 2:1 AV block — unsure of this from this tracing but it does appear to be present
3. LV injury (combination of 1 and 3)
4. Bezold-Jarisch reflex
Culprit here is the proximal RCA.
1
2
23
Adult male with chest pain. What's wrong with this tracing? List everything you can see.
#FOAMed
#MedEd
#ECG
#CardioTwitter
10
5
23
25-yo male with this ECG after noticing an irregular pulse on exam.
@BrooksWalsh
@ecgrhythms
@smithECGBlog
@AslangerE
@EM_RESUS
@MaruanCarlos
@brun_dav
@DidlakeDW
@FloydECGs
8
5
22
@EcgsOnly
Easily VT. AV dissociation clearly seen in multiple leads.
Negative concordance in the praecordial leads.
QS waves in anterior and inferior leads make me think scar-mediated VT (remote LAD OMI).
1
1
23
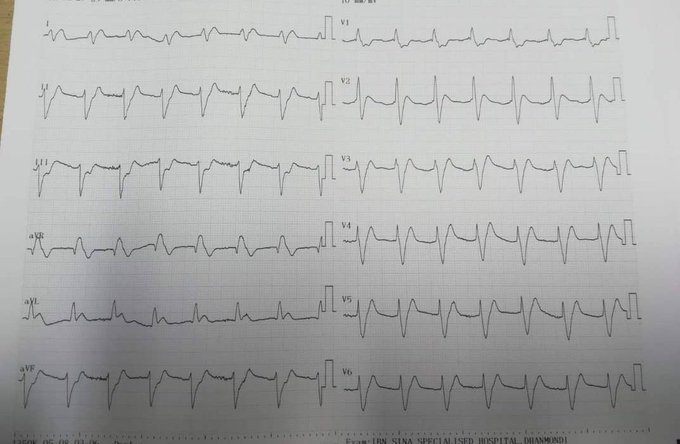
I came across this ECG belonging to a middle-aged woman without any history beyond "previous chest pain". It was termed "acute myocardial infarction".
I was thinking LVA.
Please, lend your thoughts.
@BrooksWalsh
@ecgrhythms
@smithECGBlog
@PendellM
@EM_RESUS
8
8
20
32-yo Caucasian/F, asymptomatic. ECG for pre-op evaluation. No hx of CV disease. Only known CVS risk factor is obesity. No family hx of heart disease.
@BrooksWalsh
@smithECGBlog
@ekgpress
@EcgOxford
@DidlakeDW
@RobertHermanMD
@ecgrhythms
@EM_RESUS
@ECGcases
@adribaran
11
7
23
@EcgsOnly
A weird de Winter pattern but still unmistakeable. Acute LAD OMI, enough to cause transmural injury (HATWs in V1—3) but not complete, and so subendocardial ischaemia superimposed.
Tachycardia portends LV dysfunction with pulmonary oedema vs cardiogenic shock. Prognosis bad.
0
0
22
5
9
21
Rhythm? Couldn't get a better image. Apologies.
@BrooksWalsh
@smithECGBlog
@EM_RESUS
@DidlakeDW
@syamkumarmd
@RobertHermanMD
@ecgrhythms
@EcgOxford
@PacoDardon
@marioalrb84_a
@brun_dav
@MaruanCarlos
@ekgpress
@ECG_Emily
@AThomazAndrade
@UlhasDr
@adribaran
15
6
21
20+ female with intermittent palpitations. AT vs AFL?
@SchakrabartiEP
@syamkumarmd
@UlhasDr
@smithECGBlog
@BrooksWalsh
@TahaMD_EM
@brun_dav
@MaruanCarlos
@ekgpress
@PendellM
@ecgrhythms
@narrowQRS
@PPodrid

10
7
20
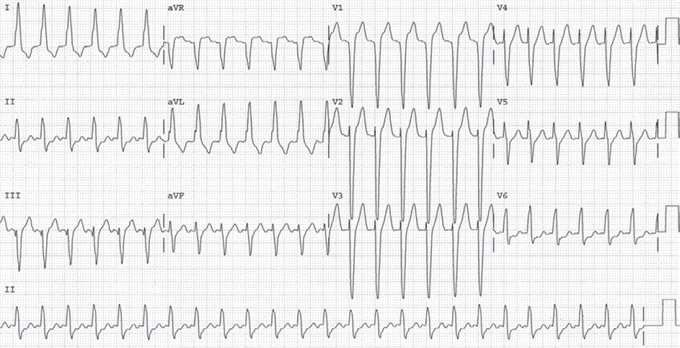
@smithECGBlog
@PendellM
We get the best sense of the QRS duration in lead II — a whopping 280 ms just by eyeballing and probably slightly more!
Only 2 entities can produce such a superwide QRS:
1. Severe hyperK (itself a Na+ channel blocker)
2. Pharmacologic Na+ channel blocker
0
0
21
@narrowQRS
Looks like two different artefacts mimicking AFL. One is more conspicuous and originates in the left leg (sparing lead I) and the other does a better job of mimicking actual AFL/AT and is affecting every lead but I can still make out a normal P wave in lead I.
Needs repeating.

2
3
20
@Tellerzee
@esther_toluu
I stand for too long, I get cramps, I get tired, my back hurts, I lose concentration, and my productivity drops. From then on, my only aim is to get out of the clinic as fast as possible. Learning can and should be less stressful.
1
3
20
@RobertHermanMD
@PMcardioBot
@smithECGBlog
@PendellM
@DidlakeDW
@BrooksWalsh
@tbouthillet
@Vadeboncoeur_Al
@ecgrhythms
@EM_RESUS
Doesn't look like acute OMI to me. V1, V2 are too high. SR with RBBB and RAD (not convincing for LPFB).
Abrupt voltage loss after V4 makes me think left-sided pneumothorax, especially with the history.
Naturally, I'd get more ECGs, CXR/Chest CT, and echo.
2
1
19
@EM_RESUS
Inferior injury is obvious. HATWs + reciprocal ST-T changes in leads I and aVL.
V1 and V2 are too high, so dubious about ST-T changes there to suggest posterior involvement but this is at least an evolving inferior OMI.
Do the usuals, then straight to cath.
0
0
20
@the_beardedsina
Insulin – dextrose/glucagon
Beta blockers – glucagon
Warfarin – vitamin K
Cholinomimetics – atropine
TCAs – normal saline + sodium bicarbonate
Etc
1
6
18
@EM_RESUS
Acute posterolateral wall injury pattern. OMI is most likely.
STE + large T waves in I and aVL with reciprocal ST-T changes in II, III, aVF. STD in V1—6, maximal in V3—4.
LCx or OM1 culprit for me.
2
0
19
@smithECGBlog
@willyhfrick
OMI with reperfusion.
Normal coronaries could mean, if this is type I MI, the thrombus has autolysed and one will need IVUS to recognise the site of plaque rupture.
Alternatively, it could be vasospasm or myocardial bridging or any other cause of type II MI.
0
0
18
@IM_Crit_
@BrooksWalsh
, I think I gasped a little after seeing the CT for "chest discomfort".
I was expecting a PE.
1
0
18
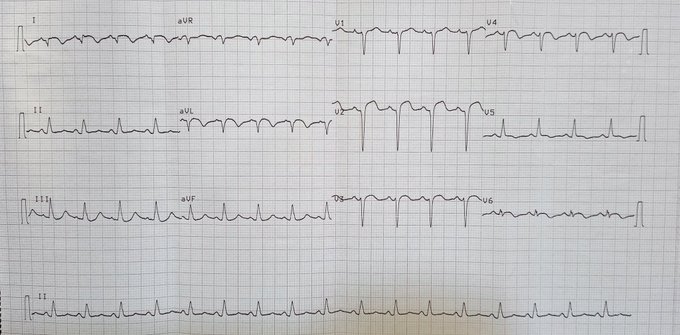
I believe I can make out 2:1 AV relationship here, making this 2:1 AT/AFL, not AVNRT.
#ECG
#EPeeps
#CardioTwitter
#FOAMed
@ecgrhythms
@DidlakeDW
@BrooksWalsh
@EM_RESUS
@UlhasDr
@Arron_Pearce_
@narrowQRS
@smithECGBlog
@EcgOxford
@RobertHermanMD

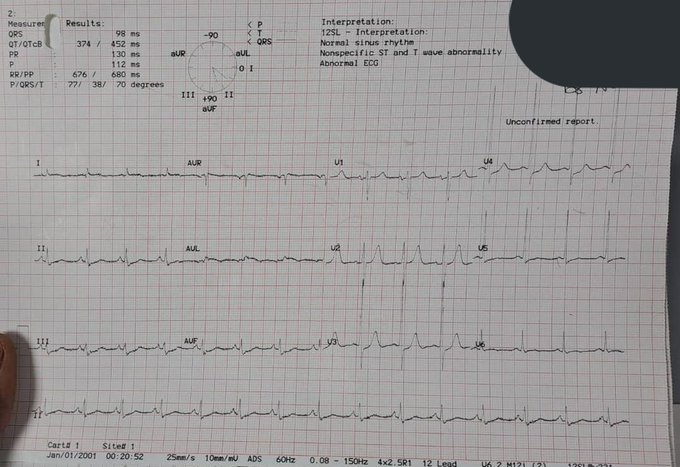
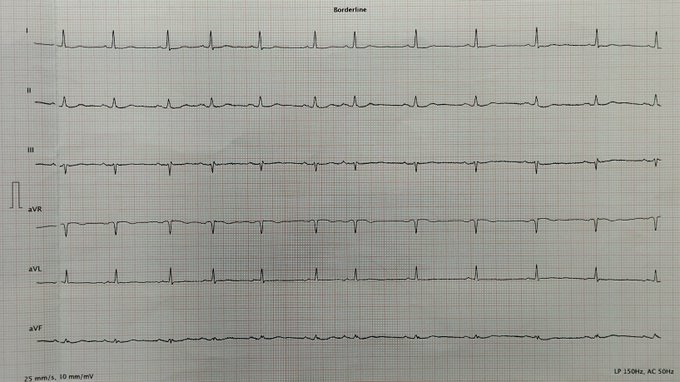
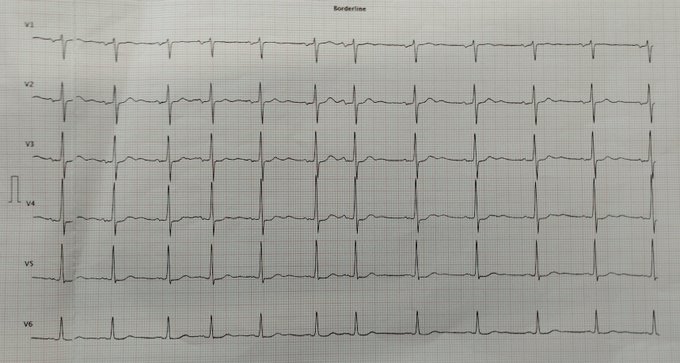
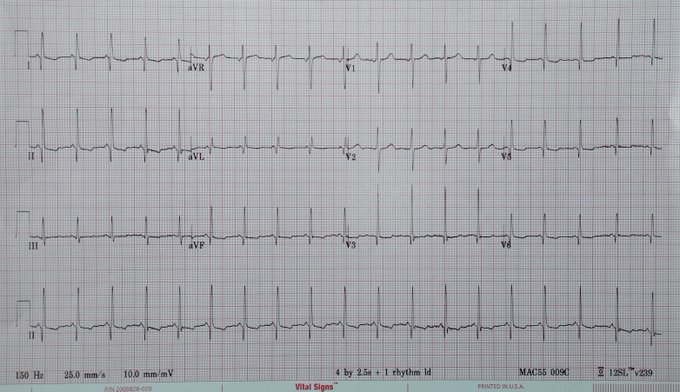
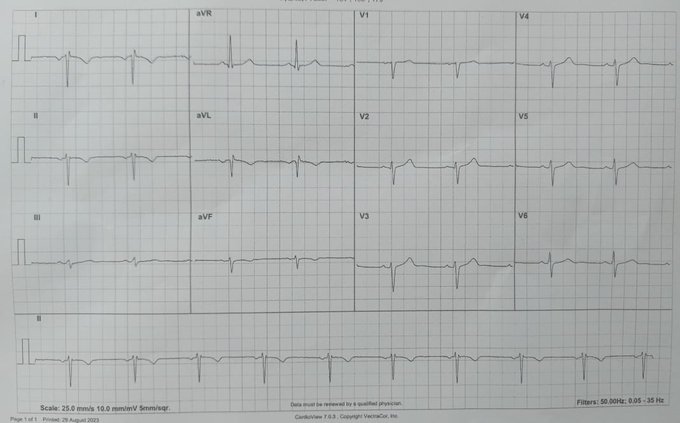
A 78 y.o. female is admitted after a fall. Her history raises the possible of syncope. She continues to remain lightheaded. An ECG is obtained.
- What's your interpretation ?
👉 Answer and Interpretation:
#medtwitter
#foamed
#ecg
#CardioTwitter
14
12
104
5
3
18
@EM_RESUS
Inferior, posterior (we know, we know), and lateral OMI.
Big RCA.
Would've quickly moved over V4—6 to the right to r/o RVMI.
1
1
17
@AngryTiger__
Having to swim through corpse-infested waters to find the corpse of your son murdered extrajudicially by those meant to protect and enforce the law, and then to not have justice.
#EndSARS
0
2
16
@EM_RESUS
SR + 2:1 AVB and ventriculophasic arrhythmia + LBBB.
Disparity between ST in V1 and V2—4 is weird in LBBB so maybe there's silent (?chest pain) RVMI and PWMI here (and so, pRCA OMI). AVN ischaemia would explain the rhythm disturbance.
0
0
18
@MaruanCarlos
1. Bradycardia (due to CHB)
1b. CHB by itself with the AV dissociation
2. Injury of the inferior, posterior, and lateral walls. LVEF could be impaired
3. Attenuated STD in V1 suggestive of RVMI as well. RVMI with RV dilation would severely diminish preload
2
2
18
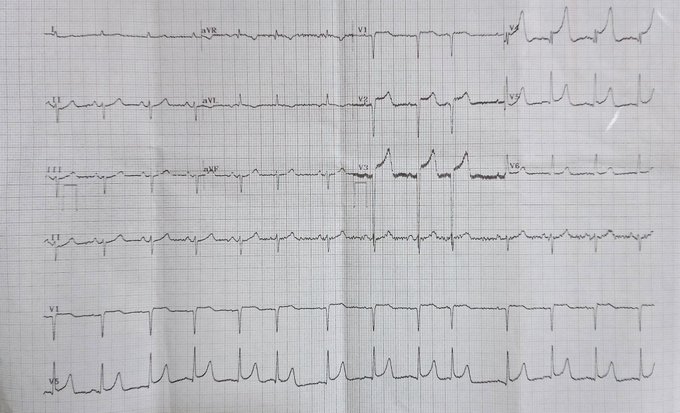
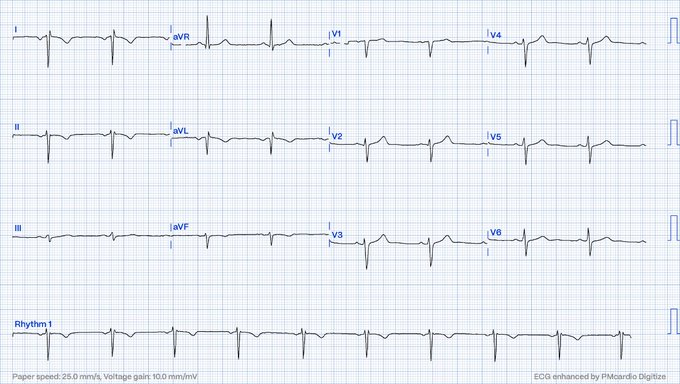
Courtesy my colleague,
@Yzmaria001
70/M, HTN/AF w/ localised left-sided CP.
*Original and digitised images shown.
#ECG
#FOAMed
#EPeeps
#MedTwitter
#CardioTwitter
#MedEd
@Arron_Pearce_
@MaruanCarlos
@DidlakeDW
@DaveRichley
@ECG_Emily
@willyhfrick
@BrooksWalsh
@smithECGBlog
9
3
18
Can VT occur simultaneously with a SVT? Got any examples?
@ecgrhythms
@narrowQRS
@brun_dav
@MaruanCarlos
@ECG_Emily
@AslangerE
@smithECGBlog
@BrooksWalsh
@EcgOxford
@UlhasDr
@Toaster_Pastry
@DidlakeDW
@ekgpress
12
2
18
"Those are not PVCs" was my reply.
1. P waves precede them (best seen in V1—3)
2. Very narrow/rapid initial aspect of the QRS (best seen in V3, V4)
PACs with LBBB aberrancy.
Asked about the likely site of origin of the PVCs. What do you think?
#FOAMed
#ECG
#CardioTwitter
#EPeeps
13
5
28
1
1
16
@Sports_Fan7
Nice motion (or tremor) artefact from the left leg (since lead I is spared completely).
0
0
16