

Atul D. Bali, MD
@ABaliMD
Followers
1K
Following
8K
Media
182
Statuses
2K
Interventional Cardiologist @lenoxhill / @ZuckerSoM🫀| Interests #CHIP #PERT #CardiacCriticalCare | Previously @nymedcollege @PennMedicine | tweets are my own |
New York, NY
Joined March 2017
Our paper now out in @JCardFail 📜.We summarize the current landscape of PE intervention & MCS platforms for high risk disease 🫀.🔹limitations in current risk strat.🔹transcatheter therapies/data/devices.🔹MCS choices, platforms, and implementation.

1
4
25
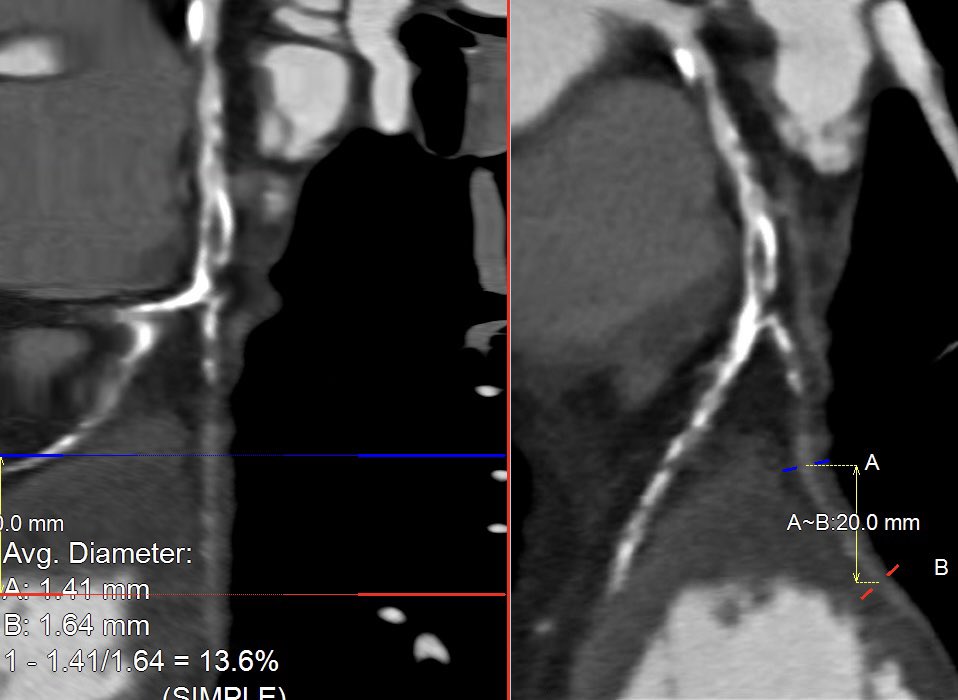
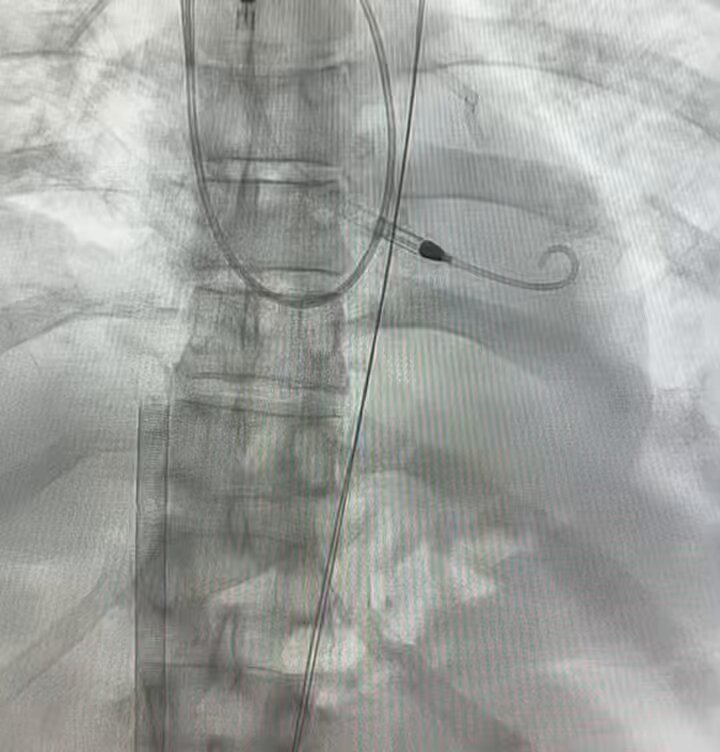
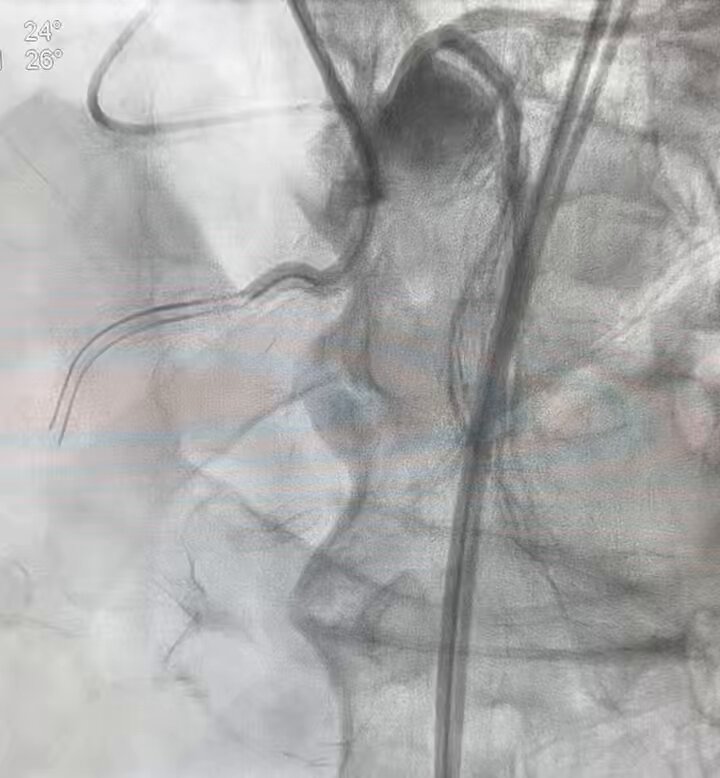
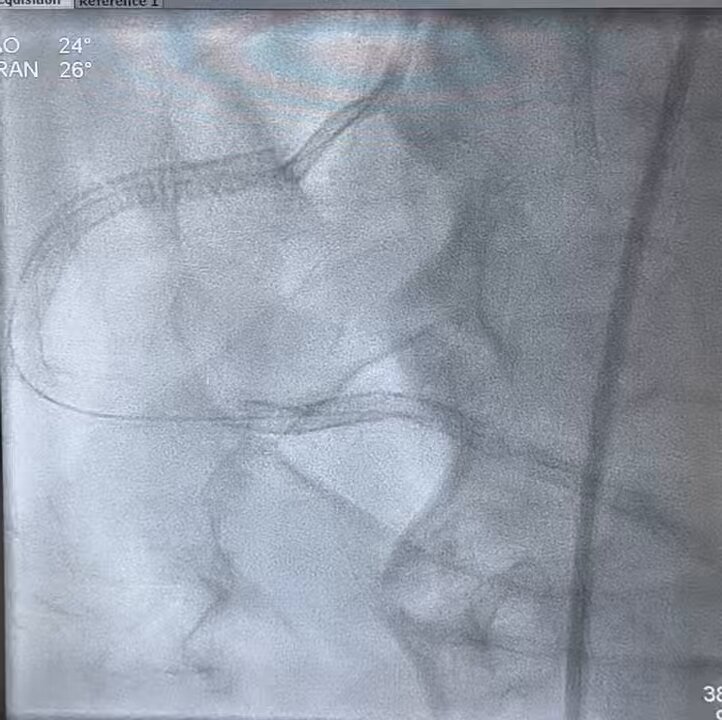
Our paper in the August issue of @InvasiveCardiol . IVBT is effective for multilayer ISR at 1-year follow up. 🔑 diligent imaging to eval morphology 📷 stepwise lesion prep prior to IVBT delivery. TLR at 1 year 10.9% - slightly improved when compared to previously reported data.

📖 Read the August issue now! @CCAD_MHIF @esbrilakis @m1chaella_alex @Dr_JHAnderson @tulliopalmerini @DrDamluji @DLBHATTMD #cardioTwitter #cardioX #cardiology #interventionalcardiology

1
2
5

Generate videos in just a few seconds. Try Grok Imagine, free for a limited time.
495
358
3K
An excellent learning case with a super educational discussion in the comments by the masters. Bravo. #CTOPCI #CHIP.

1/3 Very proximal (and long) calcified 🪨 RCA CTO (with no good native or graft retrograde options). Carlino followed by Scratch and Go with Hornet 🐝 14 wire. Subintimal traversal with P200 wire then STAR ⭐️ into RPDA with Mongo wire…



0
0
1
2/ . As always, feedback appreciated 🙏🏽 . @realarainmd @Laserrman @jl35wilsonMD @SaidAshrafMD @DrBIqbal @SripalBangalore @evandrofilhobr @DrRajeshG1 @mandeep_mayo @TWilsonMD @ShariqShamimMD @agtruesdell @DrIHHashmi1 @MichaelMegalyMD @AntoniousAttall @jedicath. #CTOPCI #CHIP.
1
0
0
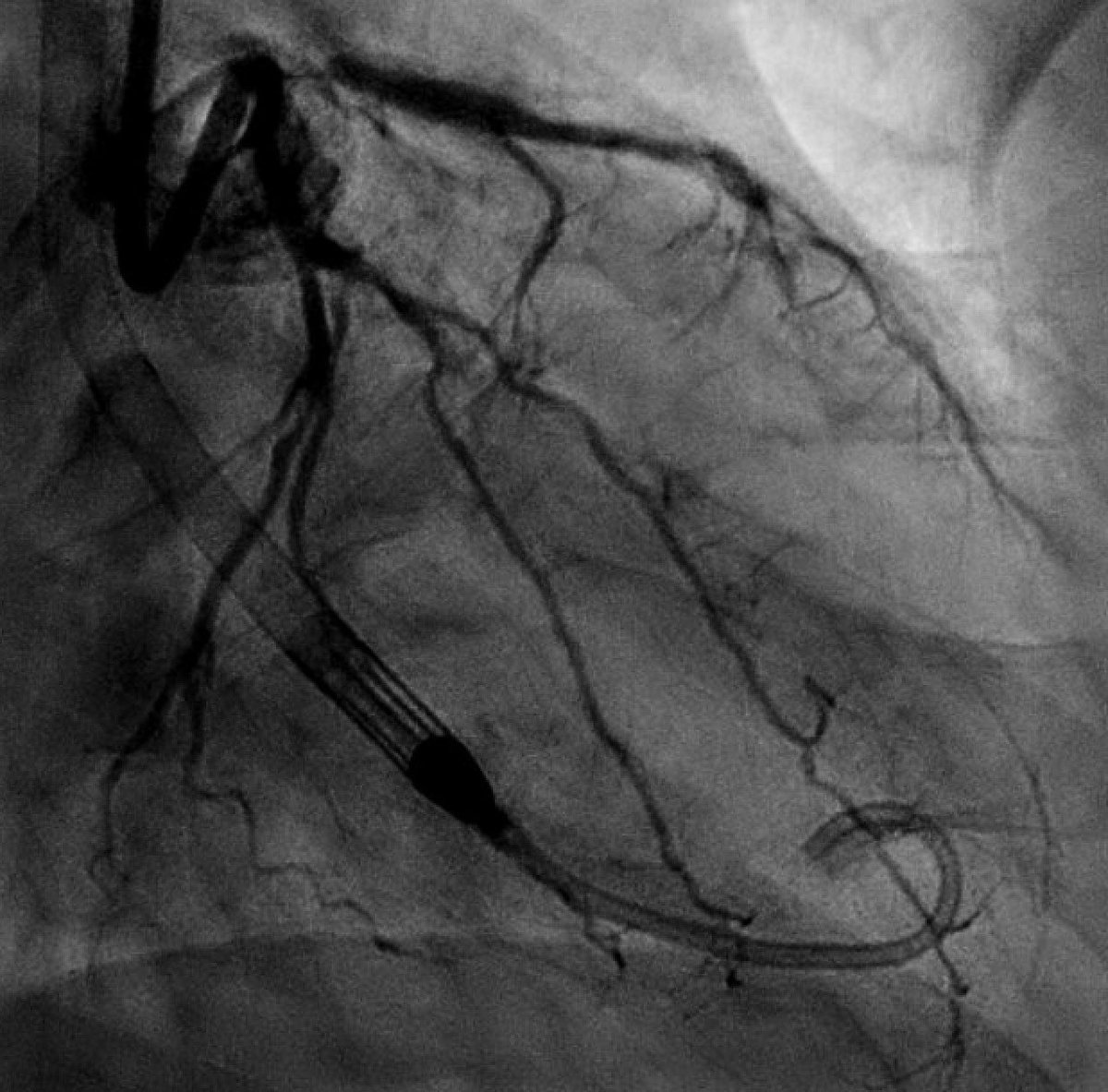
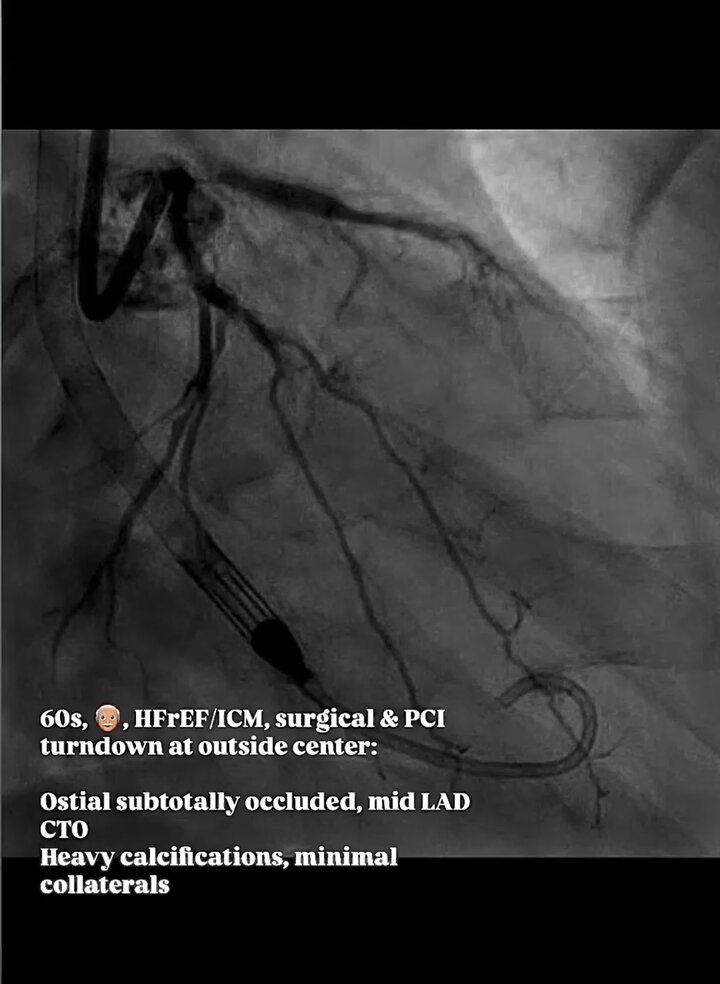
Tough Impella #CTOPCI case w/ heavy calcium:. 60s👴🏽, LVEF 35%, MV-CAD🫀. G3 ➡️ CP12 cross ostium & puncture mid ➡️ MC ❌ ➡️ free rota wire, 1.25 burr ➡️ serial NC/CB ➡️ DESx2 to prox/mid➡️ IVUS w/ poor ostial Ca+ mod ➡️ IVL to ostium ➡️ crossover DES Left main-LAD. Full PCI vid:
6
2
13


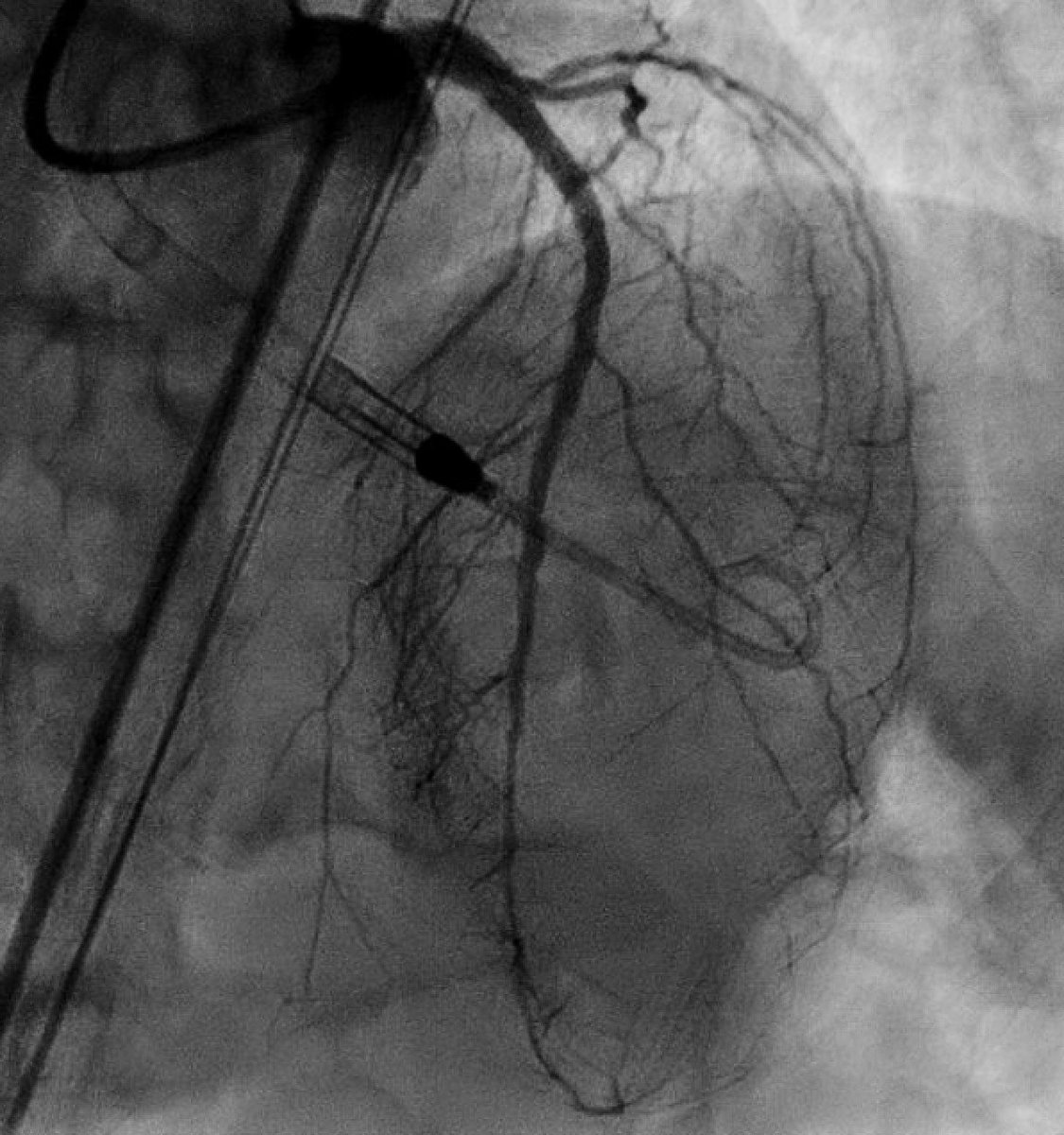
2/. Full intervention:. Mid segment where MC was “bent” was balloon uncrossable - hence up-front 1.25 mm burr.
3
0
5



2/. I typically go 1.25 burr (high speed) if 1.0 balloon or MC uncrossable for channel creation. @mandeep_mayo @realarainmd @jl35wilsonMD @TWilsonMD @SripalBangalore @evandrofilhobr @SrihariNaiduMD @SaidAshrafMD @ShariqShamimMD @Laserrman @agtruesdell @DrBIqbal @TanyaSh112
2
0
4


Int-high risk #PE by @ESC_Journals criteria, elevated #CPES score🫀💉. RV/LV ratio impressive 1.4, elevated biomarkers, and +DVT. Interestingly symptoms were mild, even on ambulation. Given degree of RV dysfunction, young age, elevated CPES - offered intervention. #PERT


0
4
14
These two have brought magic back to the tour. The future of tennis is secure. Congrats @carlosalcaraz, what an absolute warrior and champion! Picking up right where Rafa left off - Vamos 🇪🇸! . #RolandGarros.


0
0
2
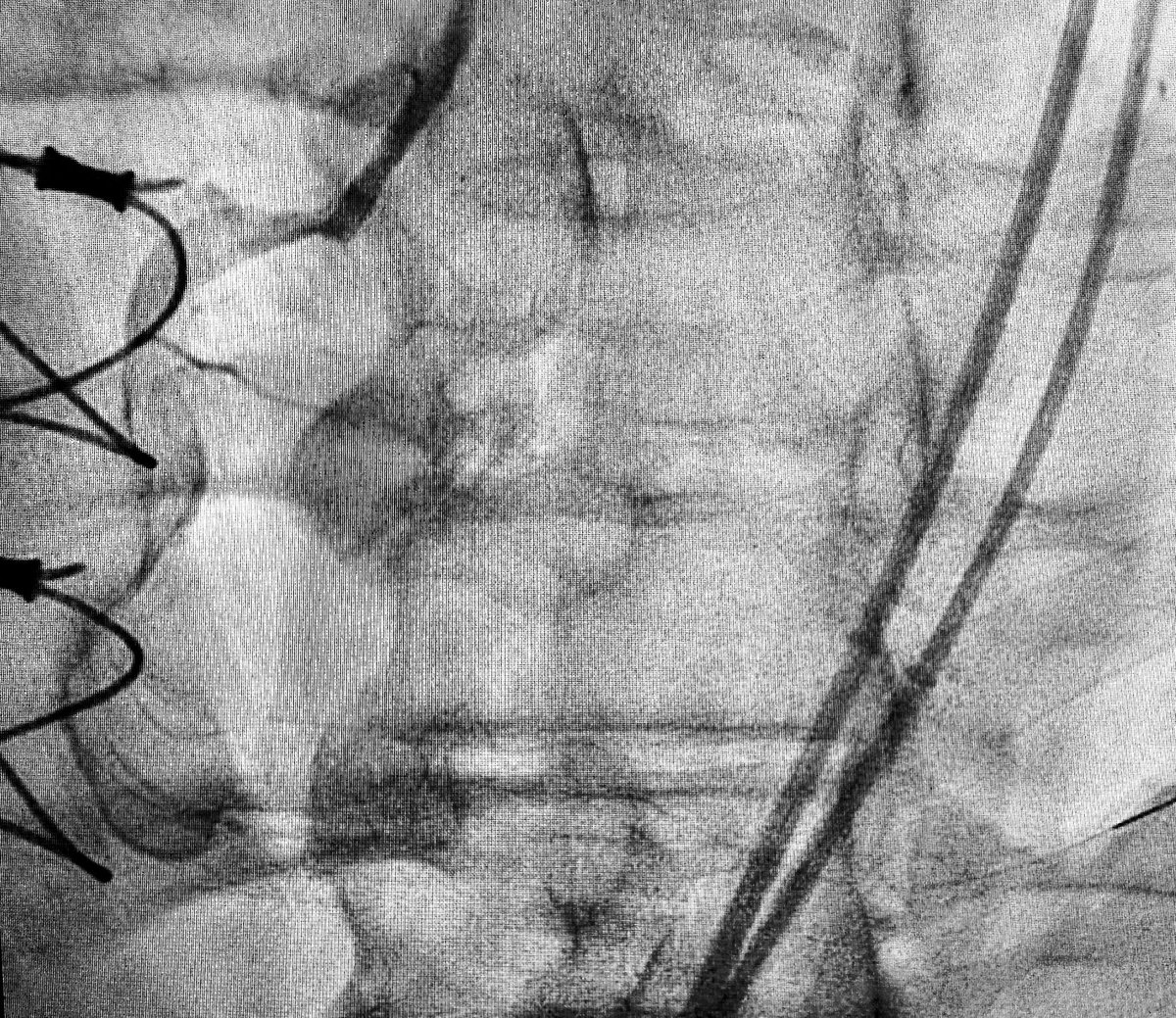
Tough one - #ECPR mid week. VA-#ECMO cannulation in ED resus for AMI w/ refractory VF ⚡️.Lucas device in-place facilitated cannulation. Door to cannulas~ 30 minutes. Followed by #Impella for LV venting & primary PCI of culprit pLAD. VF terminated after PCI. #CardiogenicShock

3
6
50
3/. As always feedback appreciated 🙏🏽. @realarainmd @Laserrman @jl35wilsonMD @evandrofilhobr @DrBIqbal @SripalBangalore @SrihariNaiduMD @MichaelMegalyMD @LAzzaliniMD @agtruesdell.
0
0
0
0
0
1

