

Lorenzo Azzalini
@LAzzaliniMD
Followers
4,798
Following
428
Media
311
Statuses
2,037
Interventional cardiologist @UWCathLab @UW @UWMedHeart . Director of Interventional Cardiology Research. Specialized in #CTO #CHIP #PCI .
Seattle, WA
Joined June 2021
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
Madrid
• 1659365 Tweets
Champions
• 711131 Tweets
Bayern
• 660763 Tweets
Joselu
• 348556 Tweets
مدريد
• 224155 Tweets
Neuer
• 172326 Tweets
Vini
• 154238 Tweets
Tuchel
• 141522 Tweets
Harry Kane
• 82551 Tweets
Luka
• 81657 Tweets
FURIA ES GRAN HERMANO
• 79017 Tweets
De Ligt
• 73404 Tweets
Uruguai
• 72604 Tweets
Steve Albini
• 65650 Tweets
Kimmich
• 55304 Tweets
Joker
• 51592 Tweets
共同親権
• 50007 Tweets
#虎に翼
• 41848 Tweets
Shai
• 38382 Tweets
Jokic
• 38124 Tweets
نوير
• 37042 Tweets
Venus
• 27594 Tweets
Shaq
• 22999 Tweets
#SalvemOCavaloDeCanoas
• 22248 Tweets
DPVAT
• 21914 Tweets
アイスクリームの日
• 20083 Tweets
Soto
• 19404 Tweets
twenty one pilots
• 17828 Tweets
Talleres
• 12579 Tweets
もちづきさん
• 10225 Tweets




















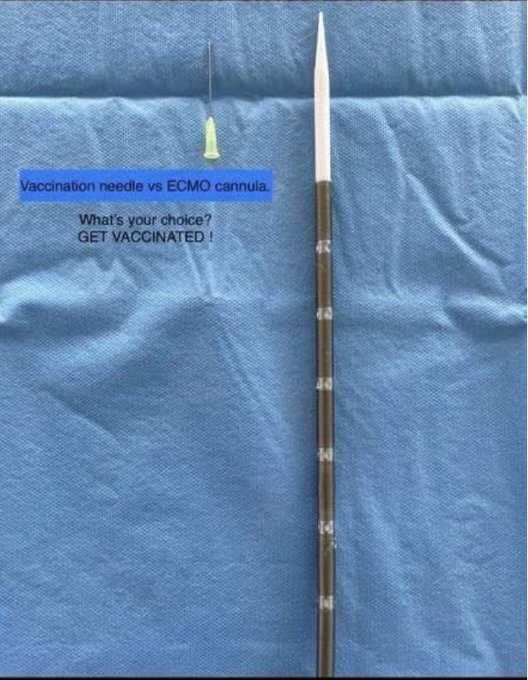

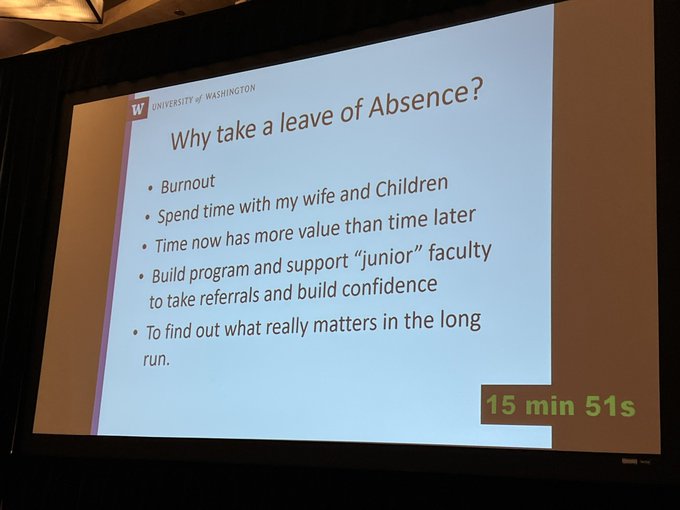
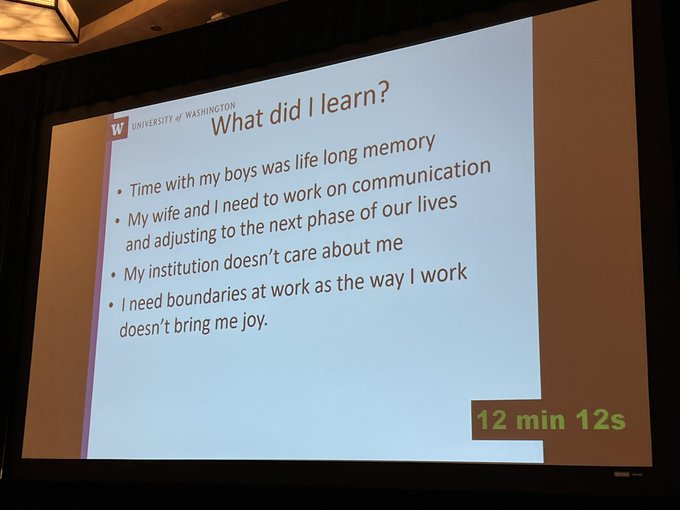
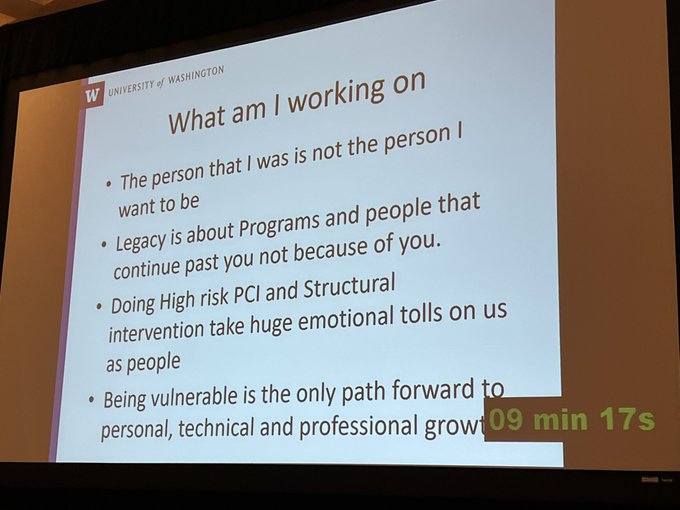
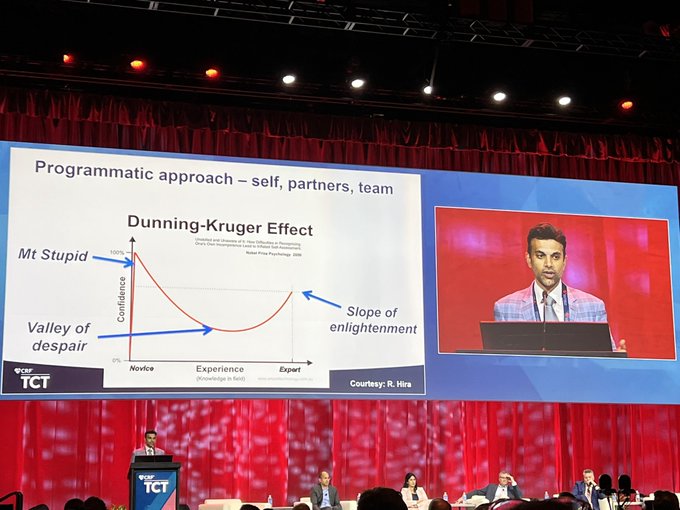
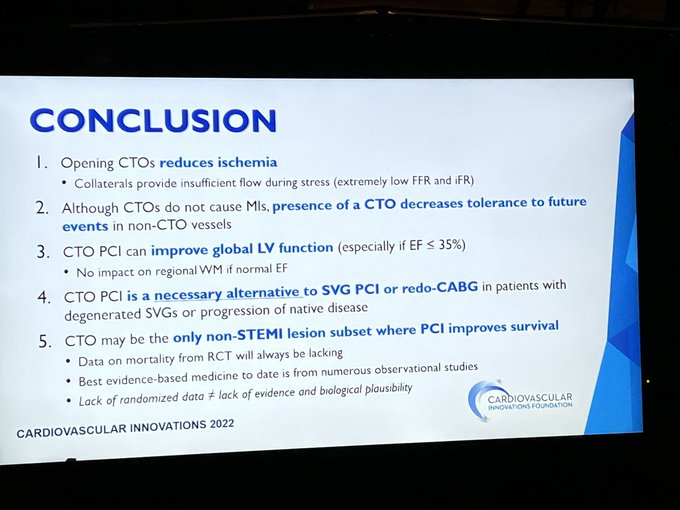
The power or vulnerability. Gigantic & inspiring talk by
@DrBillLombardi
.
#CompCourse2022
@crfheart

11
63
242
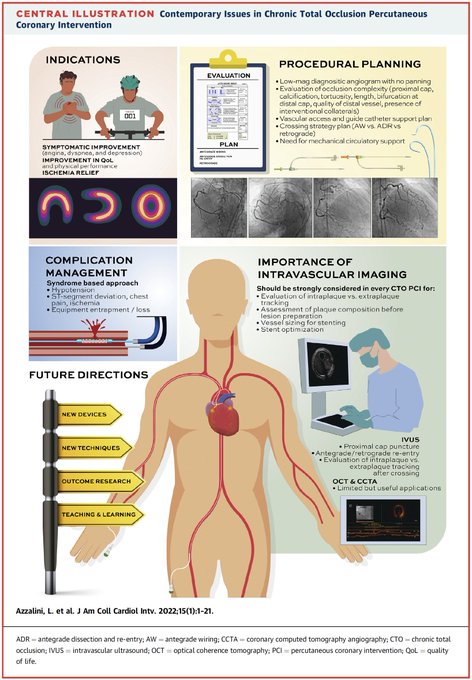
Contemporary issues in
#CTO
#PCI
-- state-of-the-art review published in
@JACCJournals
Thanks to all coauthors for their solid contribution.
@DKarmpaliotis
@rickytiago
@KambisMashayek1
@RinfretStephane
@wjn_md
@MauroCarlino3
@esbrilakis
Download link:
13
93
237
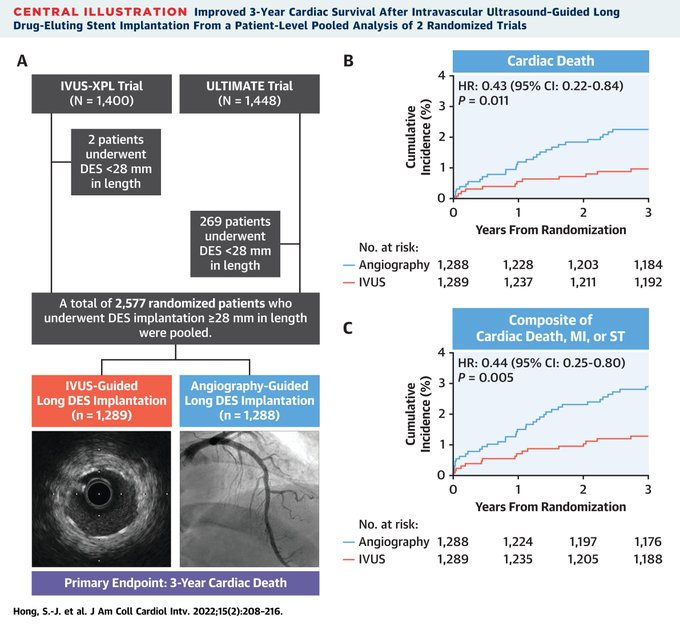
#IVUS
-guided PCI improves 3-year survival -- patient-level RCT data from IVUS-XPL & ULTIMATE.
What else do we need to get Class 1a recommendation? (currently Class IIb in ACC/AHA GL)
Probably massive training in IVUS/OCT for fellows and faculty...
5
78
217
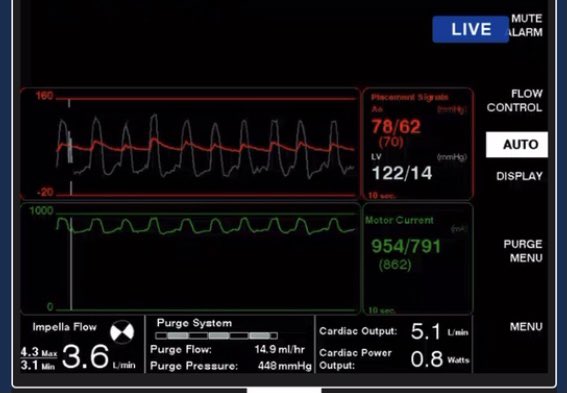
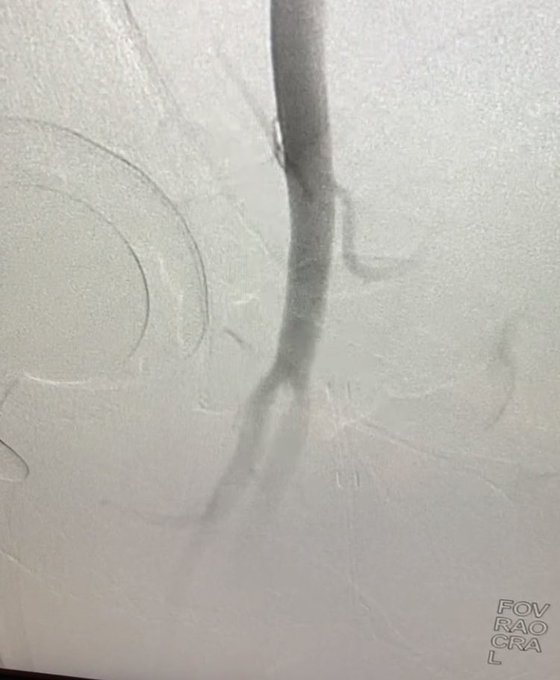
How to check for bleeding after
#Impella
single-access PCI: pull out 14F sheath, advance 4F sheath, push Perclose knots 🪢 onto 4F sheath, do angiogram👇. I learnt it from
@duanepinto
. Quite useful when you can’t do final angiogram from radial (tall pts, tortuosity, etc).
12
35
166
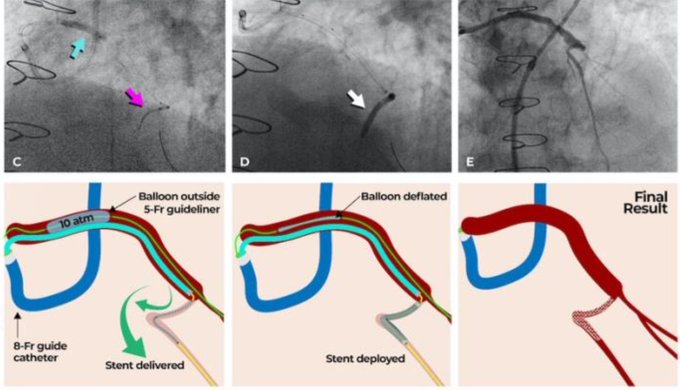
Our latest contribution to the field of
#complexPCI
#CHIP
: Guide Extension Tunnel In Landslide Technique (
#TILT
) for uncrossable/tortuous lesions. Congrats to the mastermind
@rickytiago
and our brilliant research fellow
@FrnMoroniMD
from
@VCUHealthHeart
.
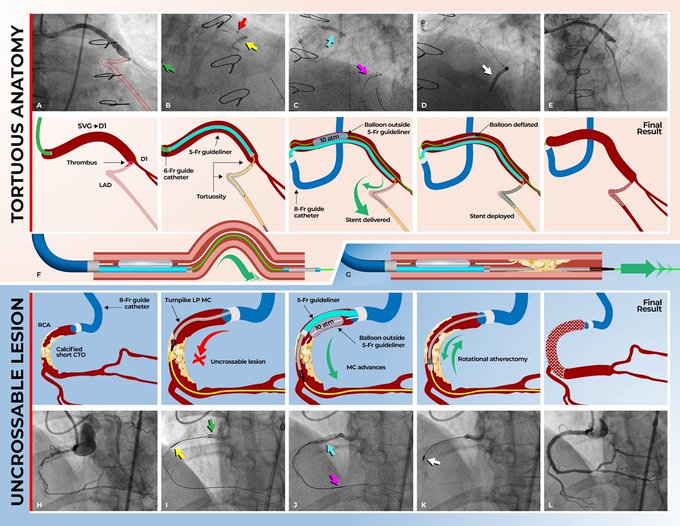

New Technique (TILT) for tortuous/uncrossable lesions described by
@LAzzaliniMD
et al. in
@EuroInterventio
: 5F Guideliner in 8F Guiding Catheter with a "buddy" balloon outside the guideliner.
@PCRonline
@SCAI
#CardioTwitter
@esbrilakis
@OptimaCTO
@CtoEuro
2
39
148
21
67
166
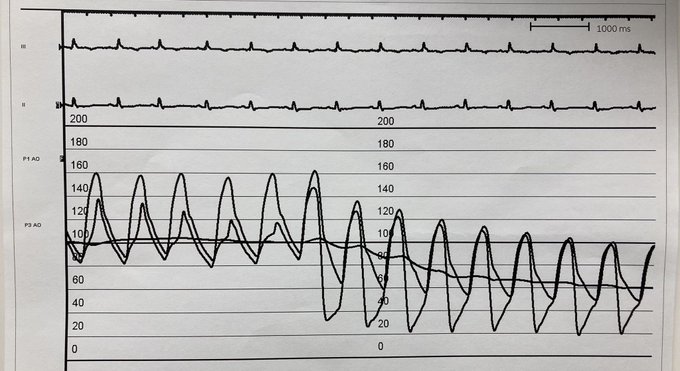
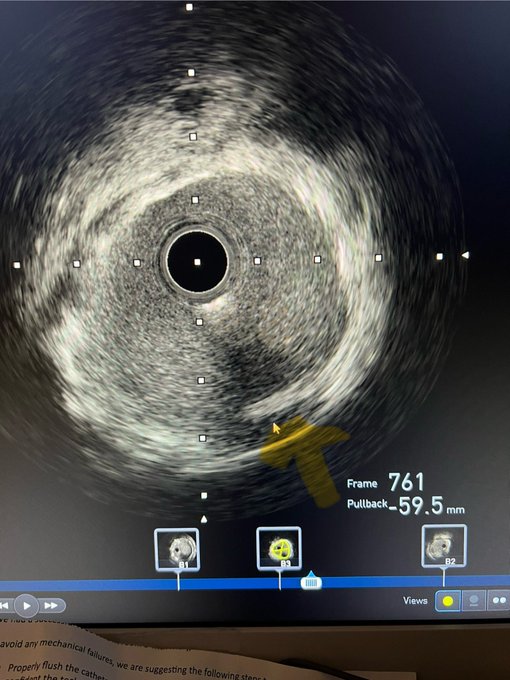
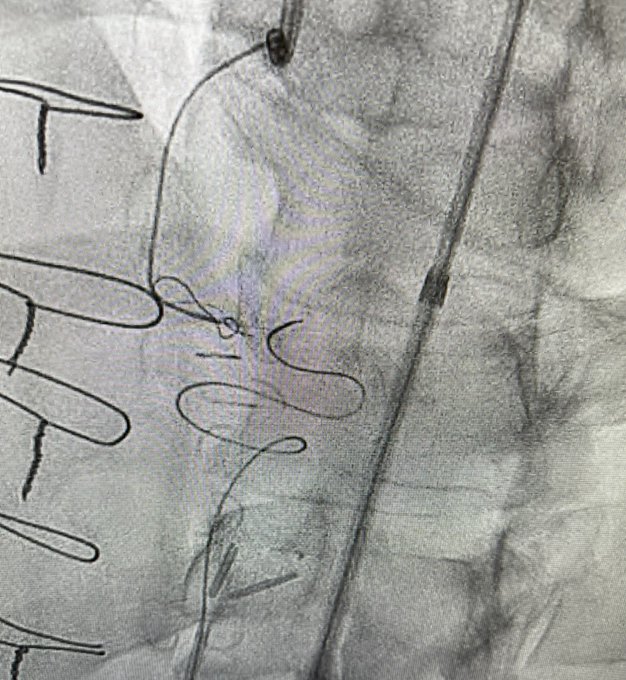
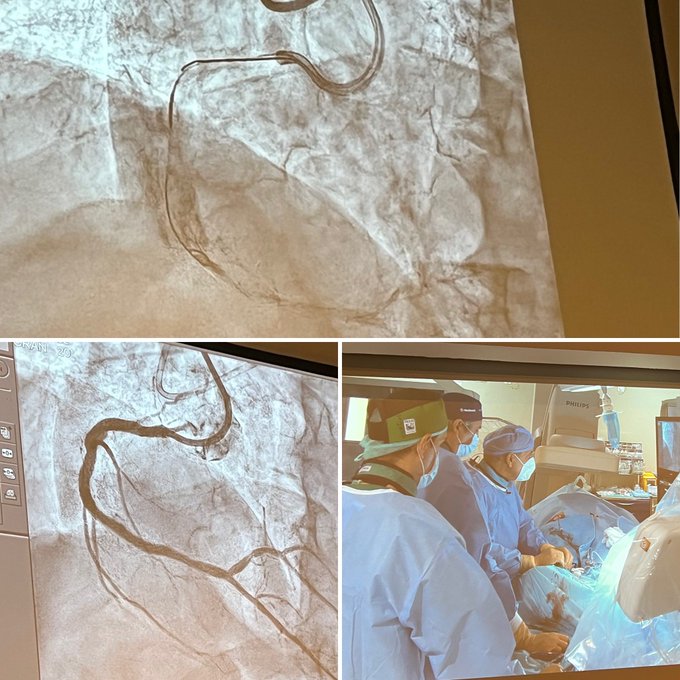
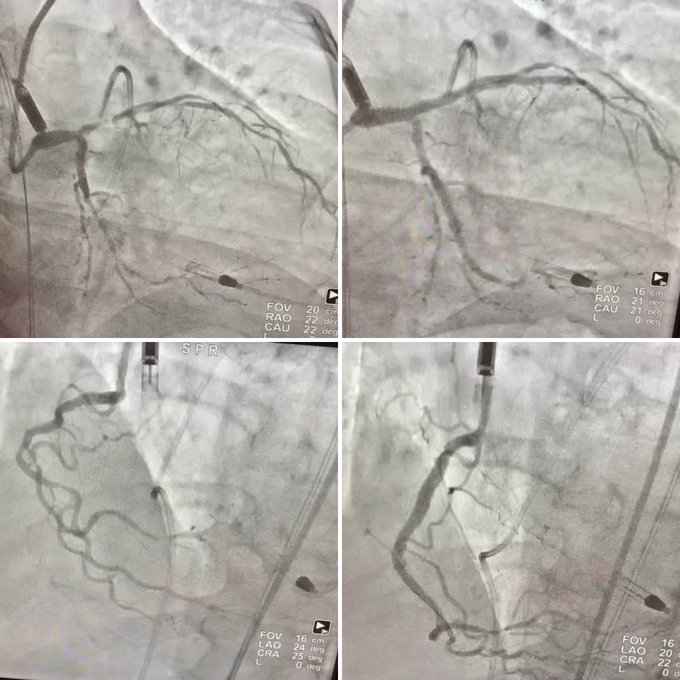
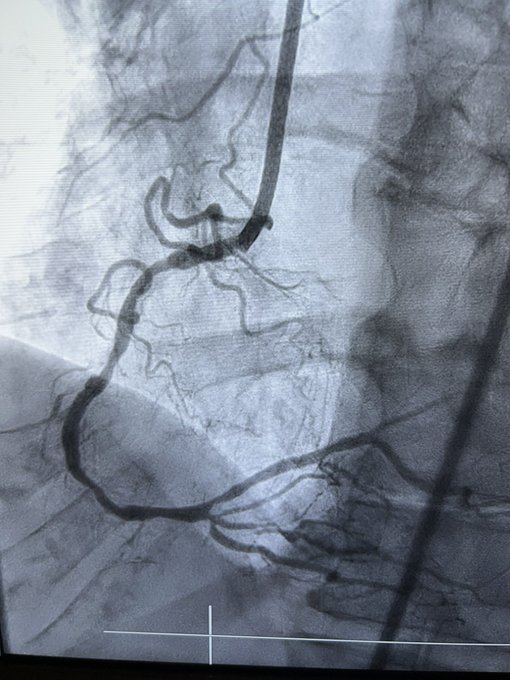
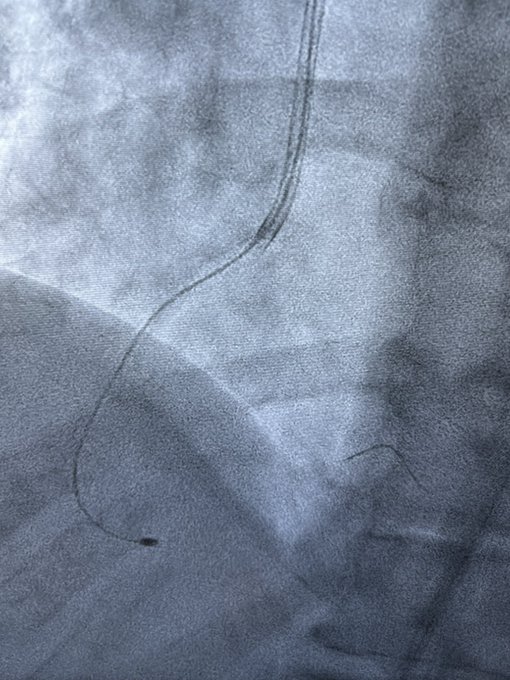
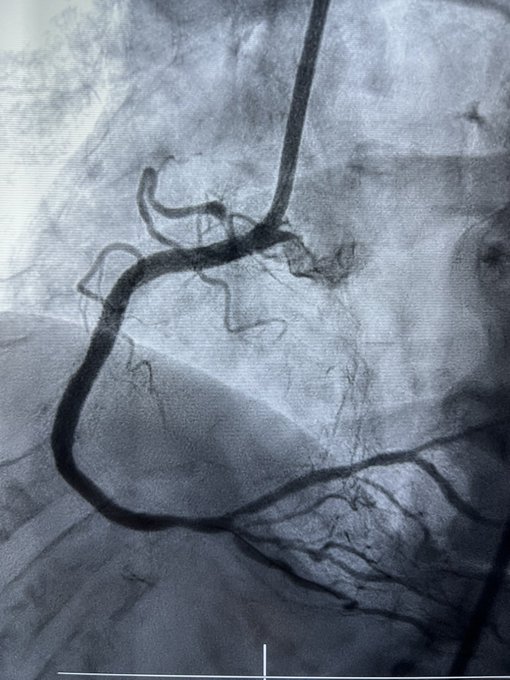
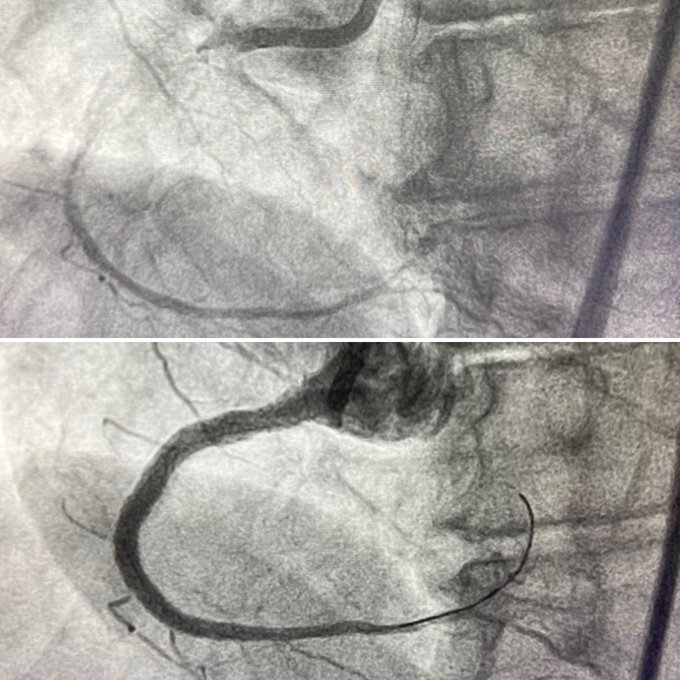
What’s going on,
#fellows
? Sudden
#hypotension
during RCA
#CTO
#PCI
while positioning a stent at the RCA ostium. (Hint: it was not a perforation)
@PCRonline
@ACCinTouch
@SCAI
@CtoEuro
@ABeneduceMD
@FrnMoroniMD
@ikutkutMD
@Babarkahn1
@VCUHealthHeart
@AbbateAntonio
@abouzaki_md
16
44
155
New randomized evidence suggests that epinephrine might be better than adenosine to correct slow flow/no reflow in ACS (higher rate of final TIMI 3 flow and lower cTFC, trend towards better MBG).
What is your experience with the treatment of no reflow?

14
56
151
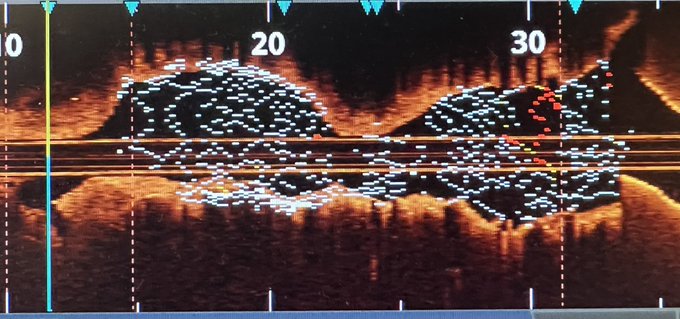
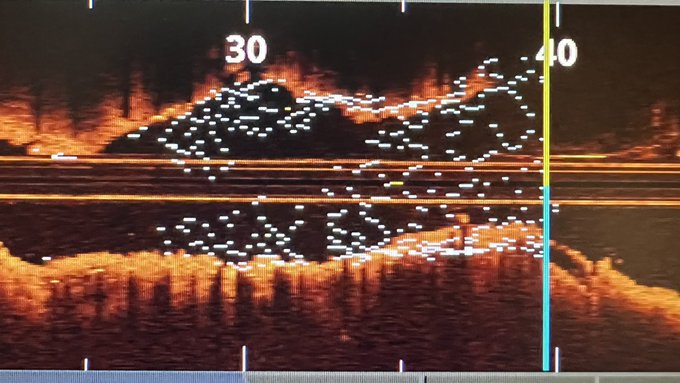
One of those days… 🙄 3-layer ISR ⌛️ in the LM (post CABG). 6 minutes of drilling. MSA went from 1.6 to 6.6 mm2 in the end. Performed entirely by fellows
@JTiwanaMD
&
@KovachMd
.
@UWMedHeart
@UWCathLab

19
22
150
Confused with minicrush, DK-crush, DK-nano-crush, etc?
Sweat no more.
Soon available on
@EuroInterventio
@PCRonline
@BifurcationClub
@latambifclub
@AmBifClub
@AppBifurcation
@FrnMoroniMD
@yeh_james3
@rickytiago
@AntoniousAttall
@aspergian1
@evandrofilhobr
@SripalBangalore
2
35
149
That was not an easy one. 👇🏻
Impenetrable proximal cap 🪨, nothing would go. Septal 🏄🏻♂️ with Fielder XT-R gets through a tortuous one. Reverse 🛒 could be performed after grenadoplasty + drilling 💎 in the extraplaque space. Tip of Gladius Mongo left trapped in Ca. 🫠
@UWMedHeart
16
14
145

6
33
141
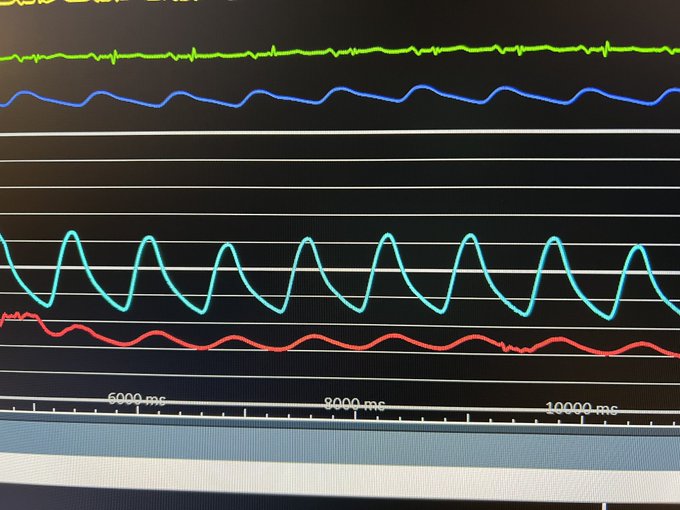
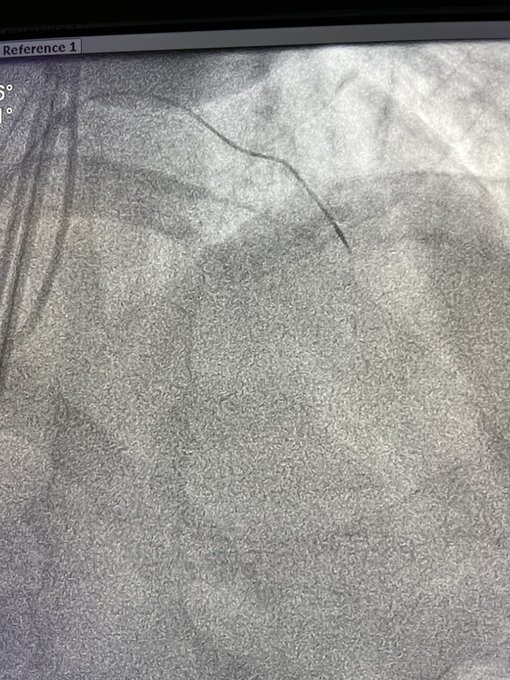
Little Xmas 🎄 trick for
#CTO
#PCI
.
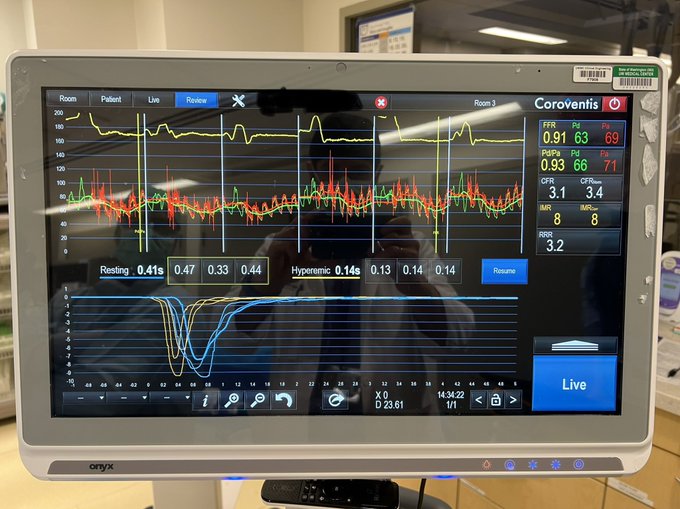
You crossed the CTO and wonder if you’re in the true lumen? Just transduce the pressure from the microcatheter! In this case, the red pulsatile tracing confirms that we are in the true lumen 💯%.
@RezMasoomi
@UWMedHeart
9
22
139
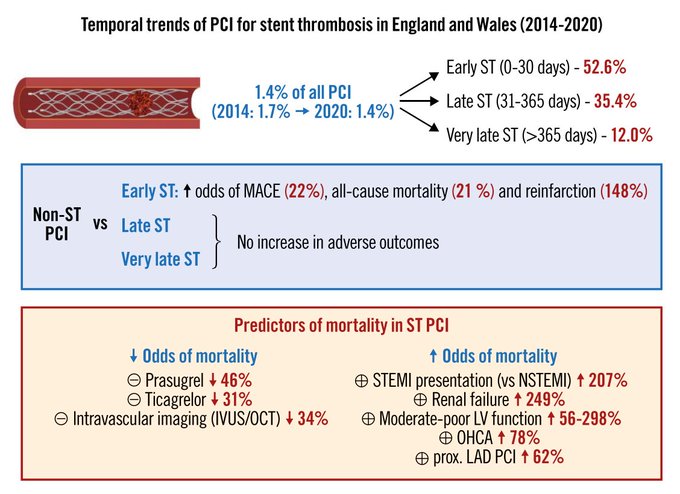
Not using intravascular imaging (
#IVUS
or
#OCT
) during
#PCI
for
#stentthrombosis
is an independent predictor of DEATH💀.
Serious conversations to be held with non-imagers in ST...
Great job
@mmamas1973
1
57
131
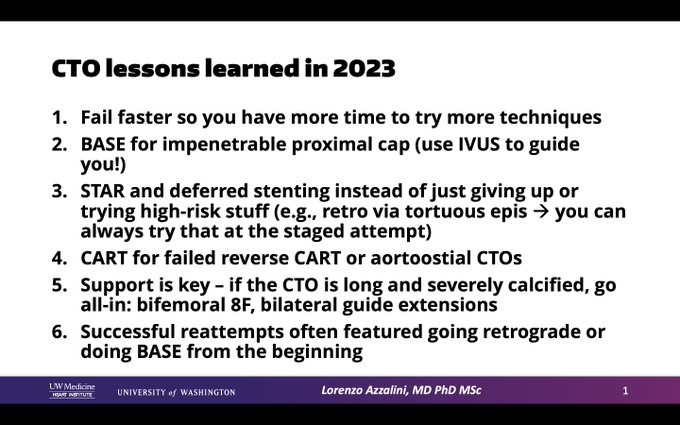
End-of-year professional thoughts 🤔.
Among many other things, I looked at all my 2023
#CTO
#PCI
failures to identify points of improvement and learn lessons from subsequent successful reattempts.
#blackboxthinking
And you, what are you doing to get better in 2024?
6
30
130
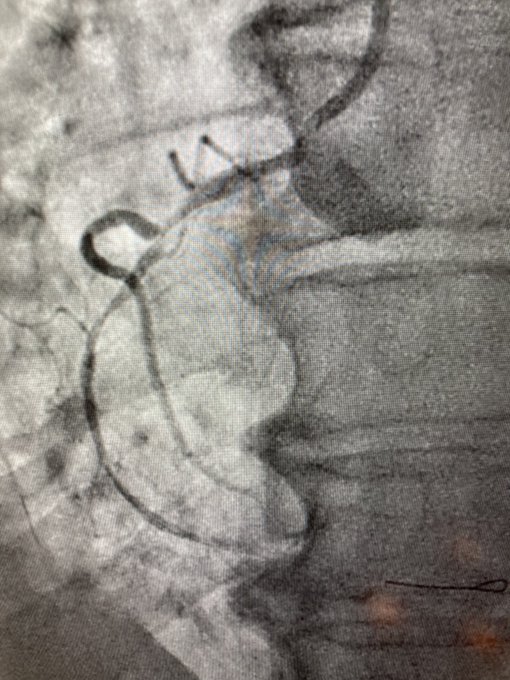
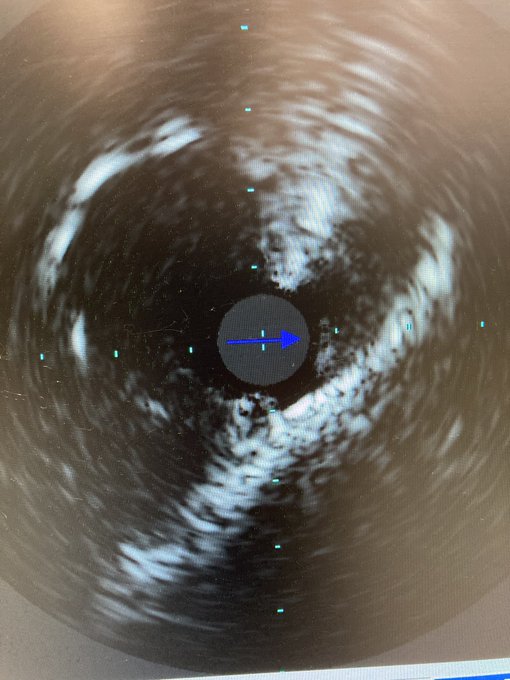
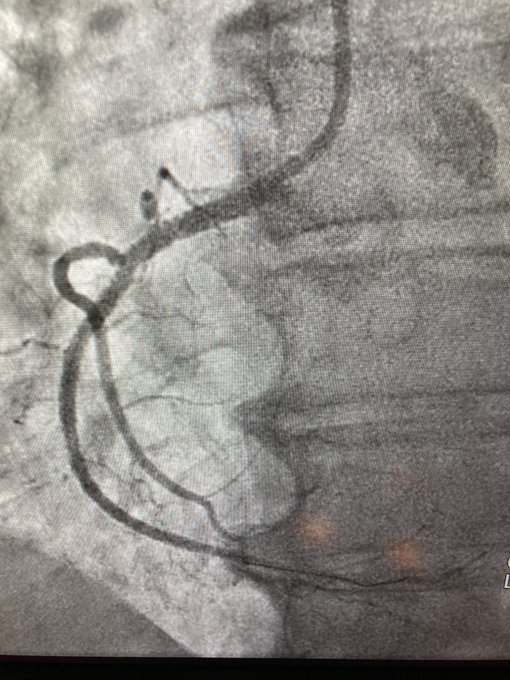
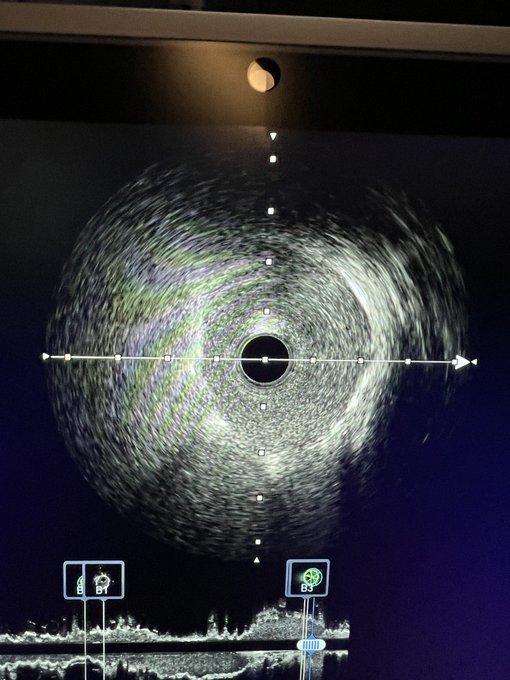
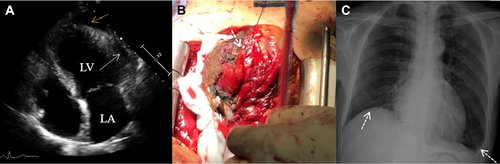
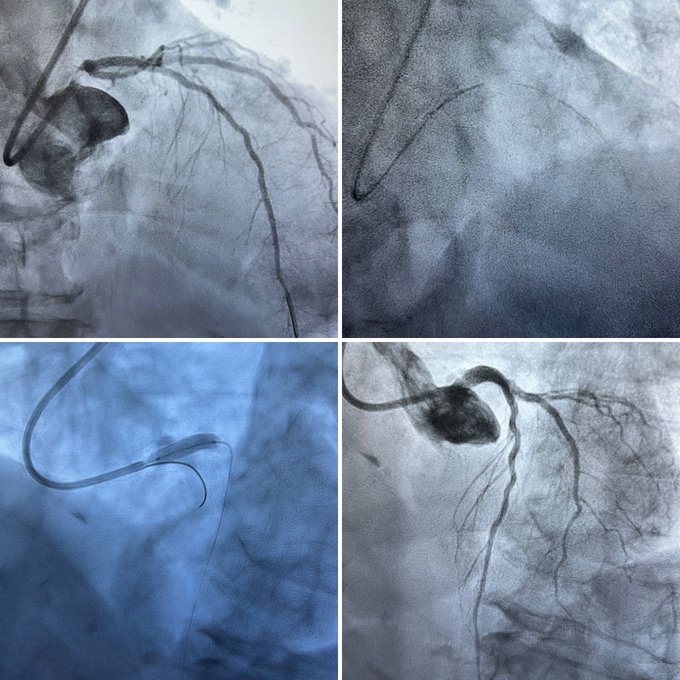
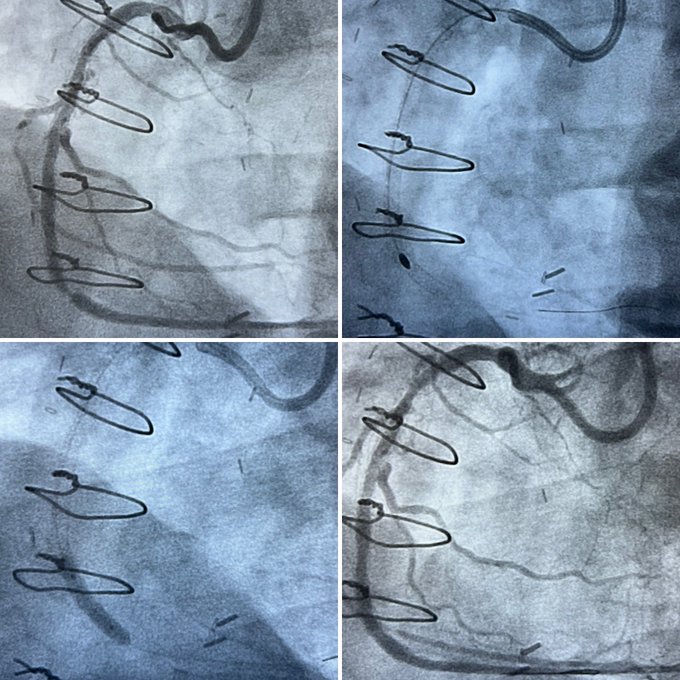
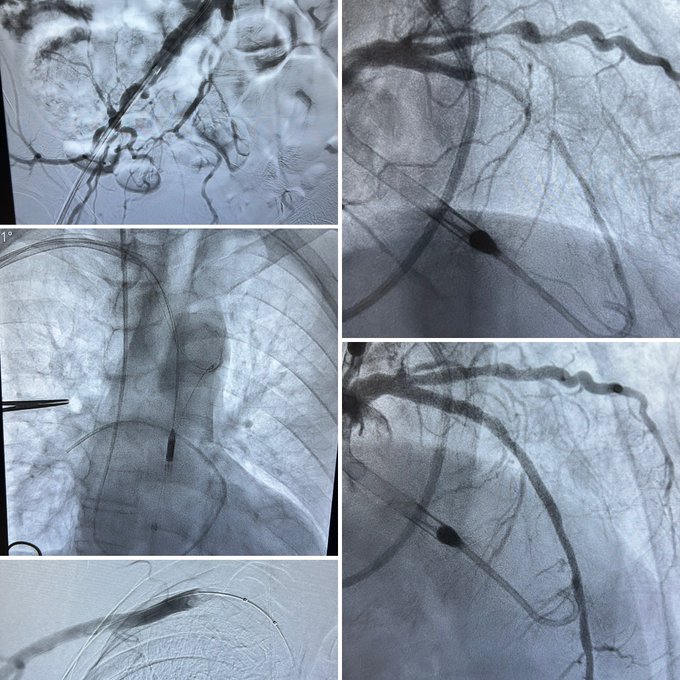
Inferior ischemia and dynamic ECG changes (with chest pain) due to an aneurysmal right sinus of Valsalva compressing the proximal RCA against the sternum.
Always learning and experiencing something new
@UWMedHeart
…
10
36
131
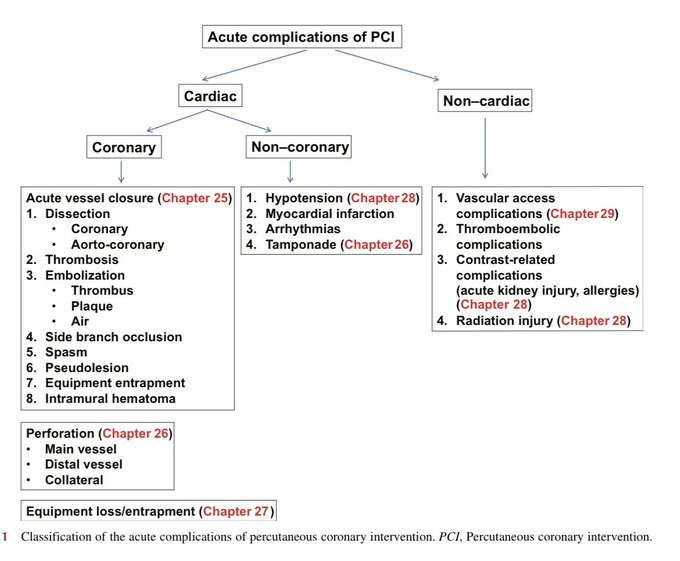
Let's talk about complications of
#PCI
.
What was:
1) The last complication you experienced?
2) The one that you experienced the most?
3) The one you fear the most?
@rickytiago
@AntoniousAttall
@ShariqShamimMD
@mmamas1973
@HadyLichaaMD
@evandrofilhobr
@OjedaOjeda18
@mirvatalasnag
33
43
128
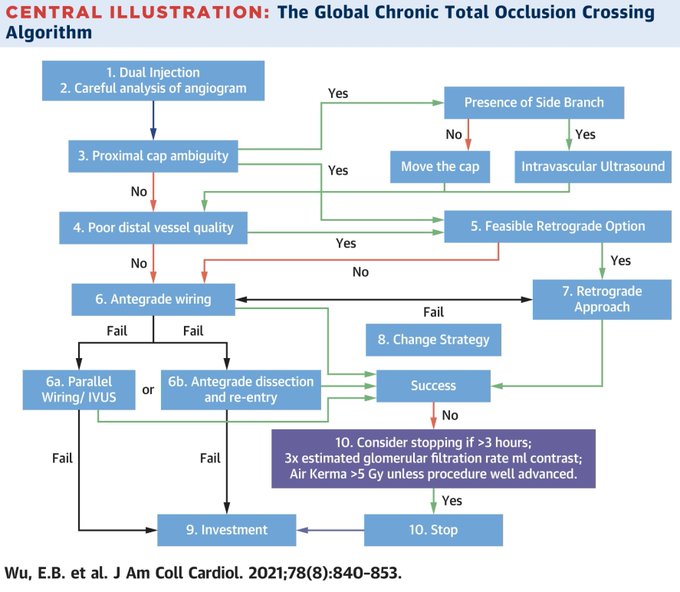
Another milestone in
#CTO
#PCI
: Global Chronic Total Occlusion Crossing Algorithm:
@JACCJournals
State-of-the-Art Review
1
44
127
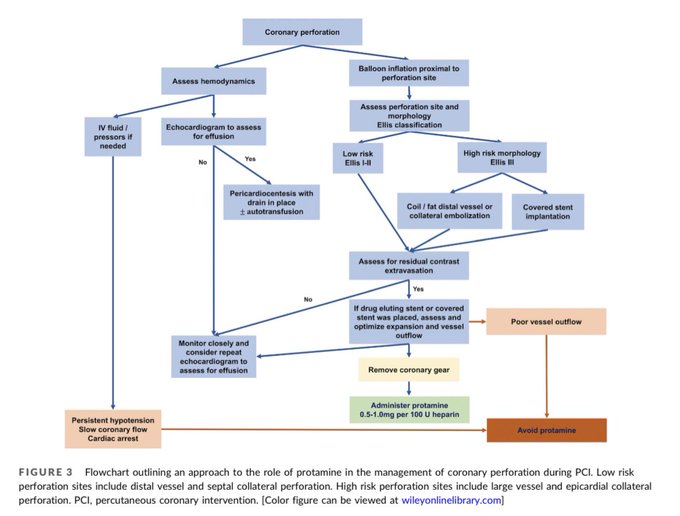
The contemporary role of protamine in the cath lab
Very thorough review by super🌟
@BarbaraADanek
from
@uwashfellows
@UWMedHeart
Safe and useful (most of the times), but use only if: 1) all gear is out; 2) no (residual) effusion; 3) there’s good outflow. Avoid if covered stents.
2
51
124
This job will never stop surprising us. Inferior STEMI with massive thrombus resistant to: Penumbra CatRX, POBA, marination with tPA via inflated OTW 🎈, ASA+ticagrelor+eptifibatide, stenting. TIMI 0 flow at the end. 24 h eptifibatide + 48 h heparin. Relook: all perfectly open 😮
14
23
122
Would you open the LAD antegradely or via the LIMA? We chose the latter (long distance to drill & lack of dedicated material if antegradely). Advanced the burr slowly with no Dyna through mild tortuosity in LIMA. Still, LIMA got dissected, but were able to quickly fix everything.
36
22
122
WHY? How can some people drop stents in (3+9=12 in this case!) without
#imagefirst
, particularly in the setting of ISR? Now we have a tough
#ISR
#CTO
. Required Astato 20 to cross.
#IVUS
showed (guess what) massive underexpansion. +1 DES on PDA, DEB on pRCA.Will it remain open? 🤞🏼
15
14
120
What a tough
#retrograde
#CTO
#PCI
performed by
@DrBillLombardi
and
@JTiwanaMD
today
@UWCathLab
@UWMedHeart
— E-CART, Carlino, CART, snaring, ostial flash, coiling of SVG.
13
21
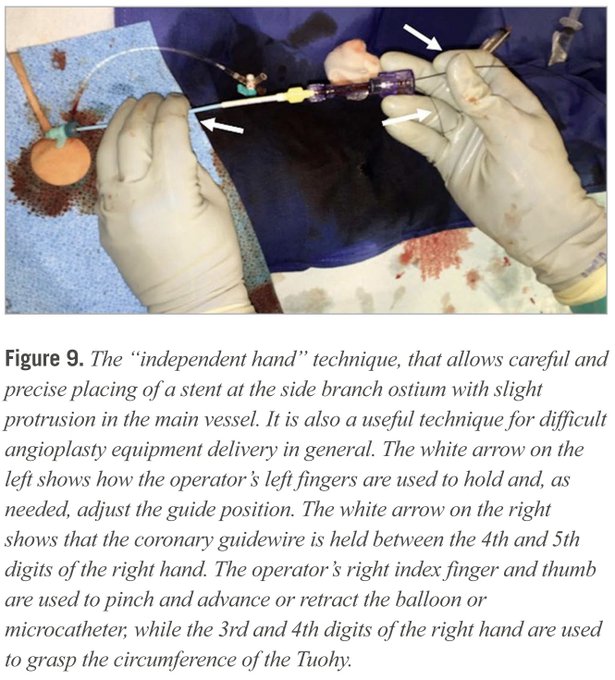
118
Never stop learning. Tips & tricks for difficult PCI equipment delivery: the "independent hand" technique by
@esbrilakis
. Great
@EuroInterventio
paper on
#DKcrush
troubleshooting.
@PCRonline
@BifurcationClub
@AmBifClub
@alaide_chief
@BURZOTTA_F
@GoranEBC
2
30
116
7
14
113
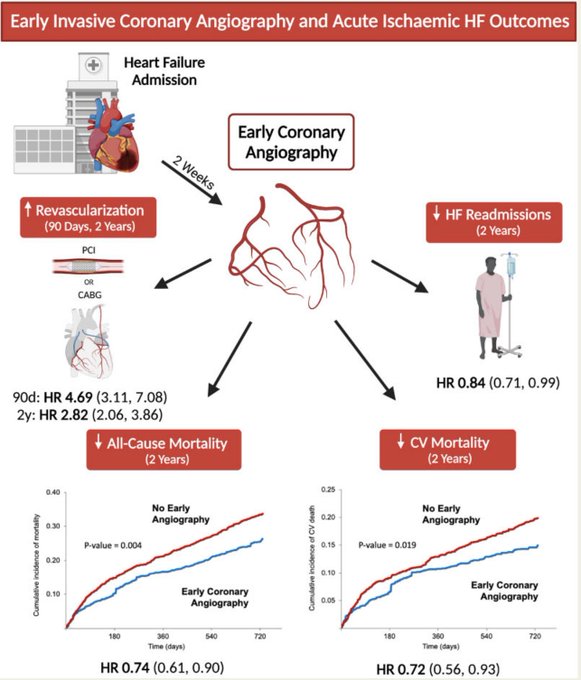
Early
#coronary
#angiography
after
#HF
admission suggestive of possible
#ischemic
etiology is associated with lower mortality at 2 years, which is mediated by
#revascularization
.
Get those coronaries open!
7
35
115

8
2
112
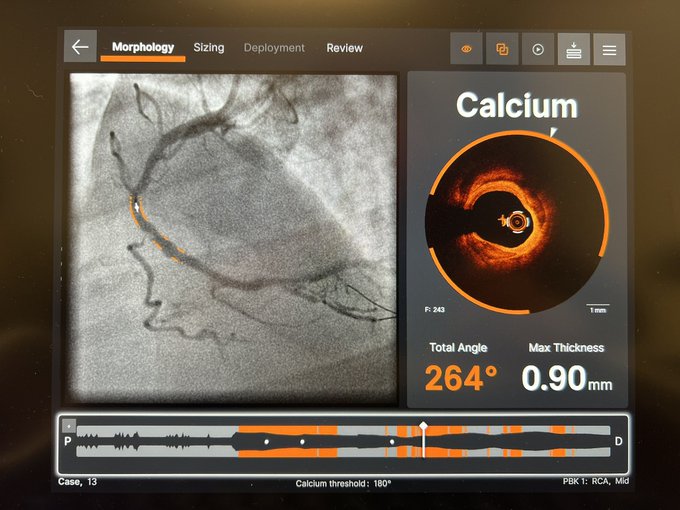
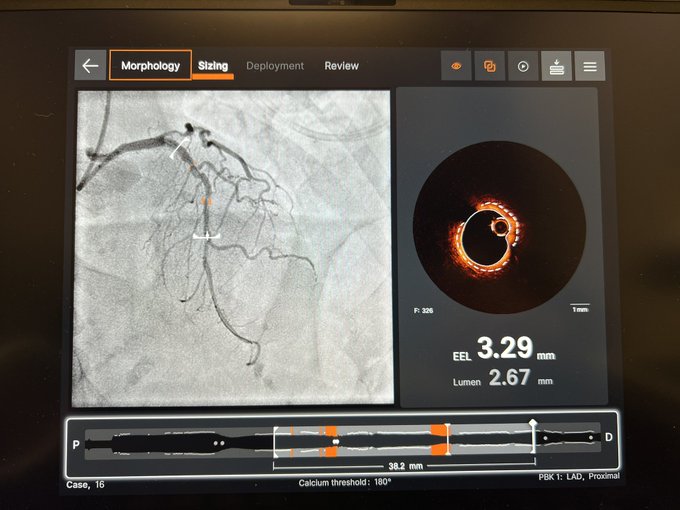
Sneak peek at the future of
#OCT
, with
#AI
-powered
#calcium
detection. It now shouldn’t take >30 seconds to plan a PCI.
#Ultreon
by
@AbbottCardio


13
13
109
These are our fellows: this time
@Doscondos
solving a Medina 1-1-1 LM bifurcation with
@csi360
orbital atherectomy on both branches, then IVUS-guided DK-crush. In 71 minutes.
@UWMedHeart
@uwashfellows
💪🏼
@UWCathLab
13
20
109
Ever drilled a septal to go retrograde?
J-CTO 5, prior failed SPM. Uncrossable after surfing invisible septal. 1.5 mm burr + POBA of septal. Tip in into guide, then rendezvous into PDA to send ante wire up the LAD for added support (couldn’t externalize R350 [100 cm guide]).
21
19
105
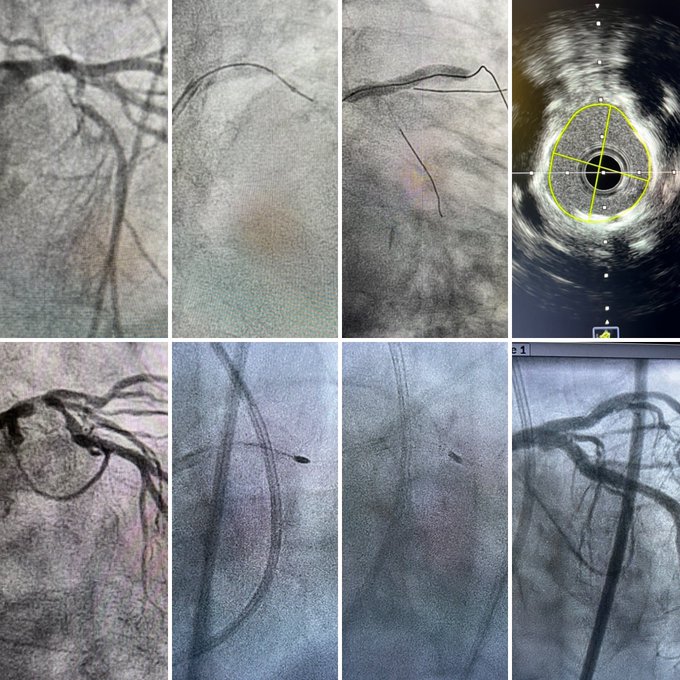
Tweetorial on myocardial bridging (
#MB
) in
#CTO
#PCI
.
1) MBs are present in ~40% of LAD CTO PCIs and in ~25% of LAD non-CTO PCIs.
Brilliant study published today in
@JACCJournals
:
7
21
103
Knuckled BMW (buddy) got jailed behind stent and entangled at its edge while pulling. Had to dilate behind stent with 0.85 mm 🎈, advance a Turnpike LP, and pull — voilà! Stent was redilated and a new stent placed distally (distal strut looked bad on IVUS). With
@HussienHeshmat
9
12
98
Congrats to our awesome IC and
#CHIP
fellows (
@JTiwanaMD
@thinkmdkane
) who just did 1) zero-contrast
#PCI
with
#orbital
#atherectomy
& 2) left main
#rotational
#atherectomy
&
#DKcrush
, while I was sitting in the control room. Your future is bright!
@UWCathLab
@uwashfellows
3
4
99
Congratulations to my mentor
@DrBillLombardi
on being recognized with the
@crfheart
Hartzler Career Award for his mentorship and clinical excellence. You impacted so many people’s careers and patients’ lives. Your legacy will be everlasting, Bill. I’m proud of you!
#TCT2023



1
12
100
#Rotational
#atherectomy
to clean up an embolized microcatheter tip.
#CHIP
#PCI
Nice little trick -- with
@rickytiago
and
@esbrilakis
10
27
98
Flush ostial RCA
#CTO
. Multiple SVG failures. Patient with eGFR 25. Very challenging AW with Pilot 200 over CoraForce. Orbital
#atherectomy
+
#IVL
. Coiling of SVG (competitive flow). 25 ml of contrast. Brilliantly performed by
@JTiwanaMD
.
@UWCathLab
@UWMedHeart
💪🏼
12
14
97
36 yo male presenting with chest pain and dyspnea on moderate exertion for 1 week. Normal ECG. Troponin 4.78 ng/ml. Echo: LVEF 50%, anteroseptal and apical akinesis. Diagnosis?
@JTiwanaMD
@UWCathLab
@uwashfellows
@UWCardiology
@UWMedHeart
28
21
96
Has anyone ever seen this before?
Months after STAR-based recanalization of an LAD
#CTO
, we found this two-lumen structure: both lumens (false and true) exhibited the black circular line that represents the EEL.
Great case by
@thinkmdkane
@UWMedHeart
12
28
96
#percax
#Impella
left main
#rotatripsy
and provisional stenting live at
#SPCI2023
— first case of
#IVL
on the 🏝️
Great interaction with the moderators
@rickytiago
and
@AjayKirtane
Thanks, SPCI, for the opportunity to educate the audience and help your patient.
1
18
90
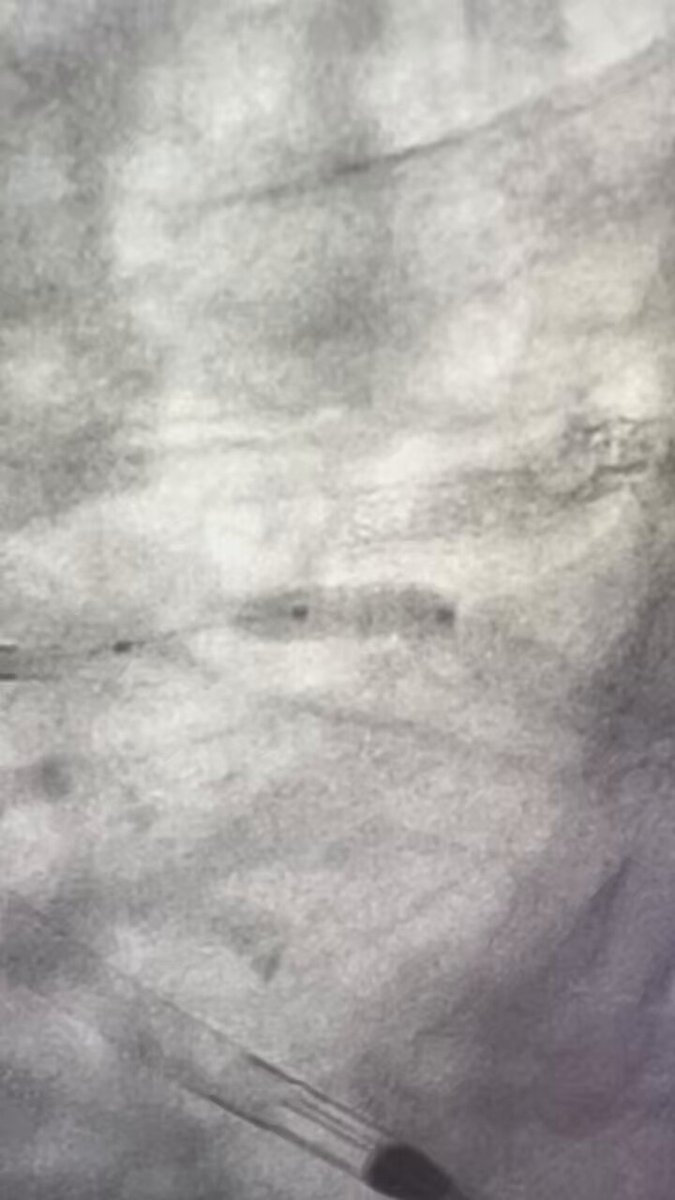
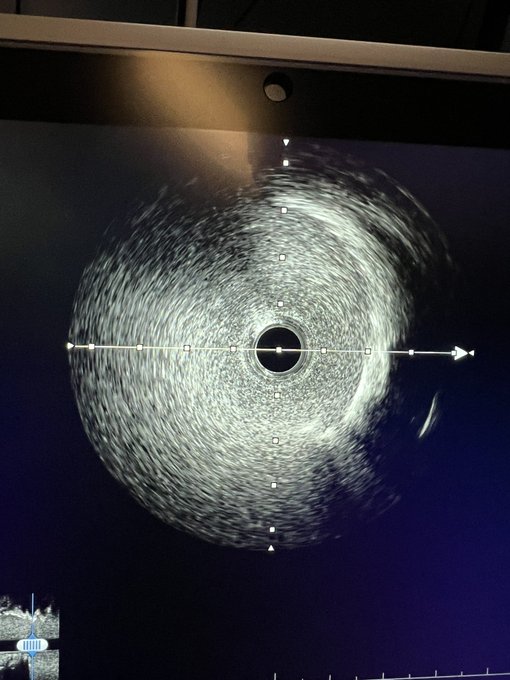
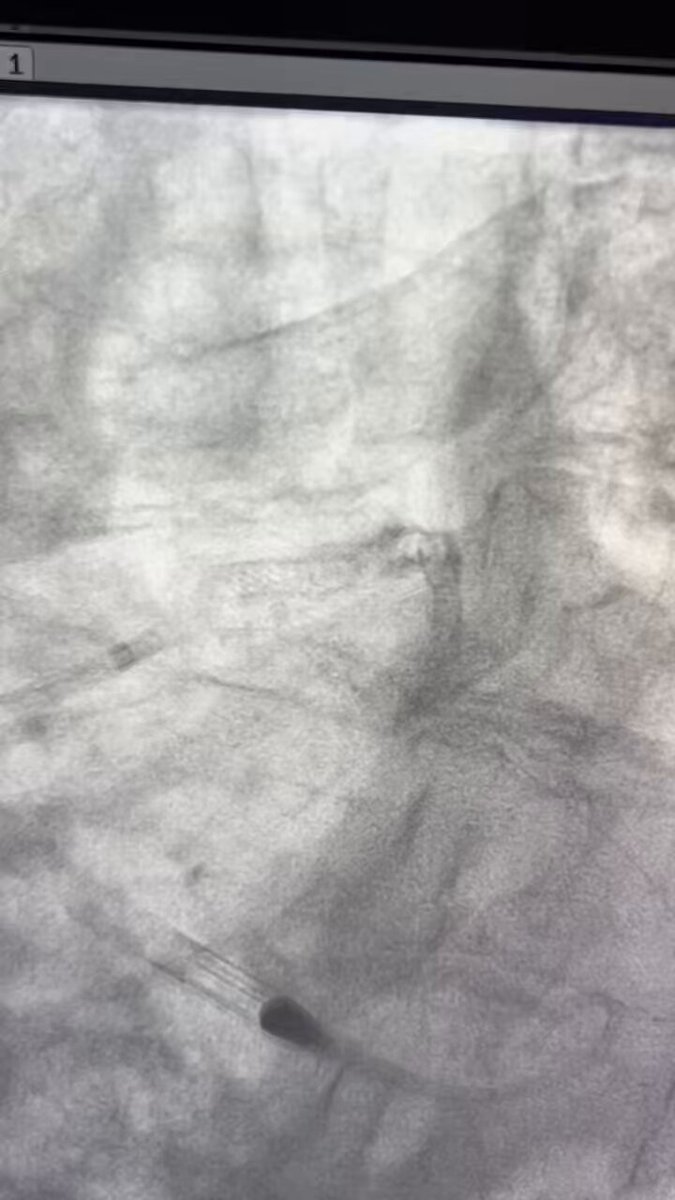
Cutting 🔪 balloon 🎈 to fenestrate 🪟 subintimal hematoma 🩸 in the distal vessel after
#CTO
#PCI
.
Once again,
#IVUS
informs the best management.
The vessel will heal.
@RezMasoomi
10
14
91
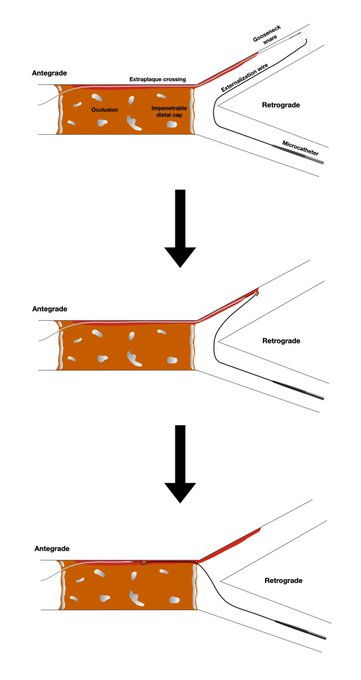
One more tool for difficult
#retrograde
#CTO
#PCI
Intracoronary
#snaring
of the retrograde wire: a novel method to solve compartment mismatch in complex retrograde CTO PCI
Cool case published by
@SMoscardelliMD
@Doscondos
@DrBillLombardi
@ccijournal
3
21
89
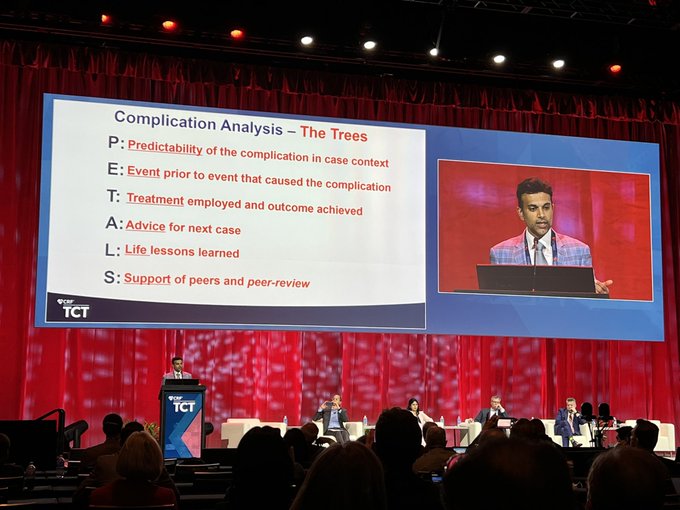
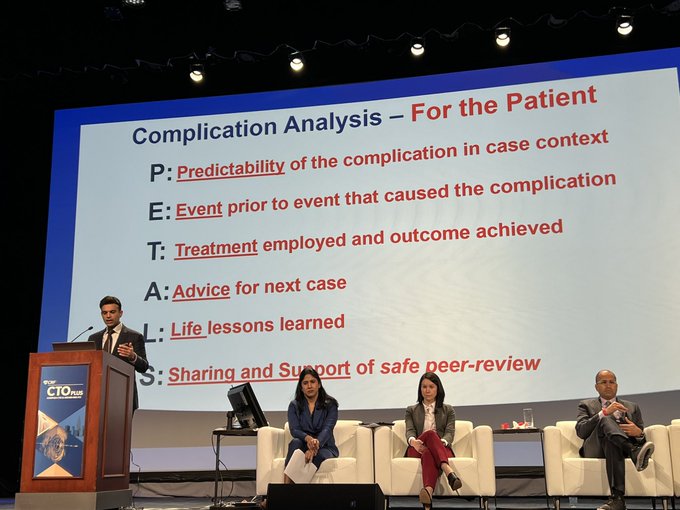
Outstanding and humbling lecture on how to improve and learn from complications during complex
#PCI
by
@SanjogKalra
. Structured approach to make every complication truly matter and decrease the likelihood of recurrence. Great ✊🏼 teamwork and personal growth at
#TCT2021
.

2
12
86

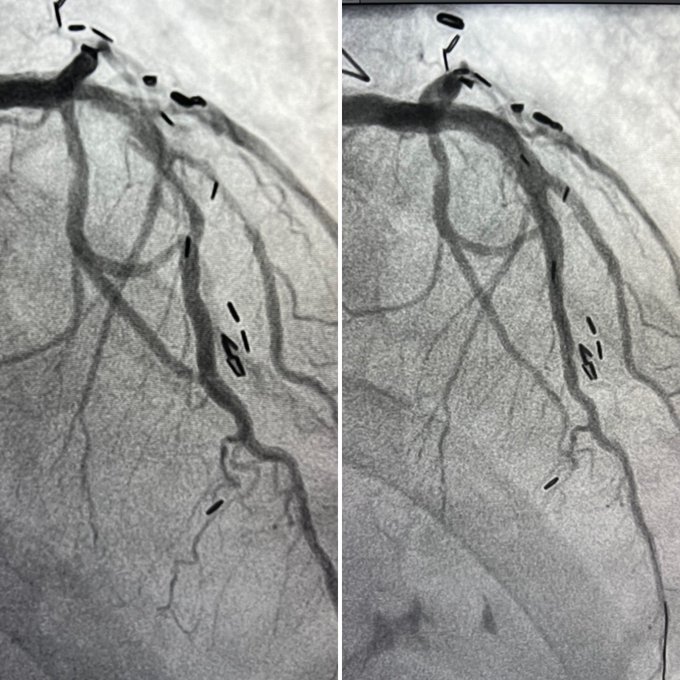
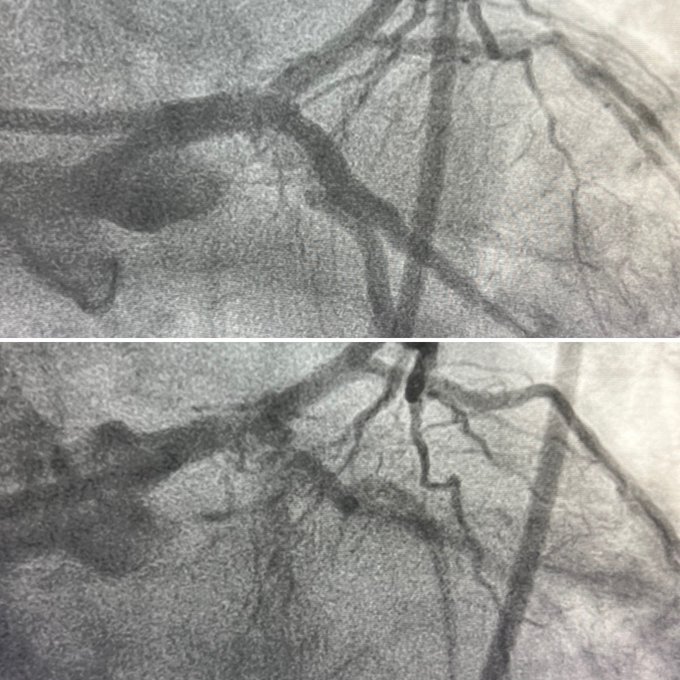
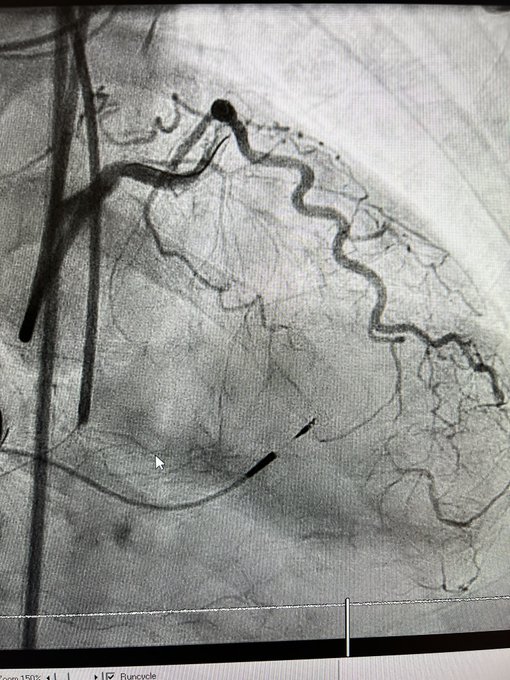
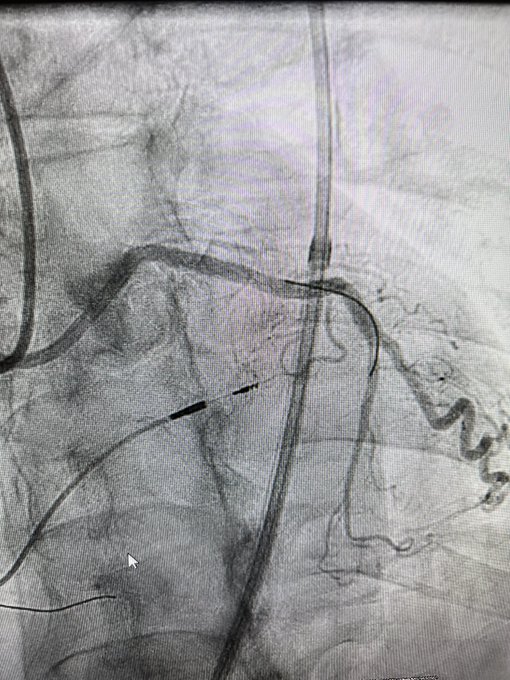
Double LAD CTO before and after LIMA. Impenetrable prox cap, BASE power knuckle, retro via LIMA, failed rCART, successful CART, antegrade wire subintimal at second CTO, retro via ipsilateral epicardials from D1, rCART and retro wire into antegrade guide, tip in, 3 DES.
@UWMedHeart
15
10
86
A great part of being a great operator is being a good person. Pearls of wisdom and must/read 📚 by
@DrBillLombardi
with visiting interventionalists
@UWMedHeart

3
8
86

5
22
85
@jamiemccabeMD
@DrBillLombardi
@KateKearney4
Thanks
@jamiemccabeMD
. I’m super excited to be joining such a stellar team at
@UWCathLab
, and honored to become part of an inspiring group of professionals who strive to provide the best care to the patients in the WWAMI region.
@UWMedHeart
@UWCardiology
20
4
85
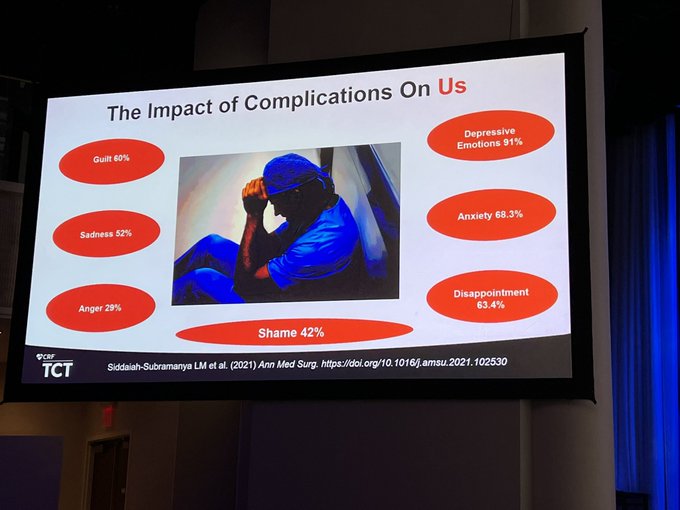
Emotionally and professionally enriching session on the psychological aspects of complications on physicians at
#CTO2022
. Thanks for candidly sharing your experience
@SanjogKalra
— a true leader in complex PCI and great physician.
@crfheart

2
9
84
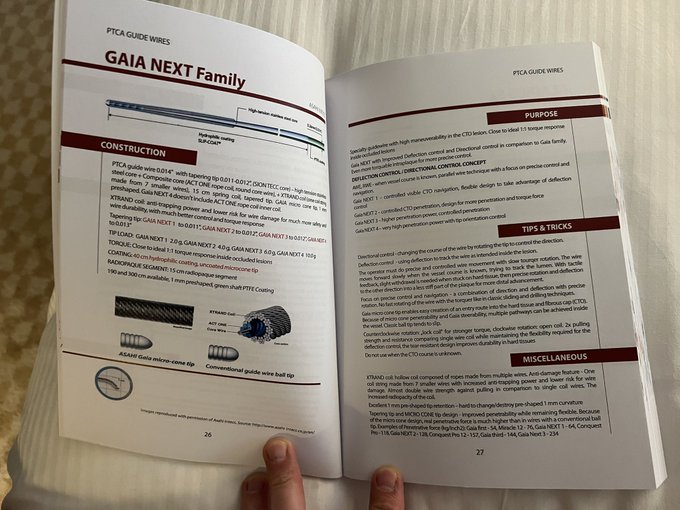
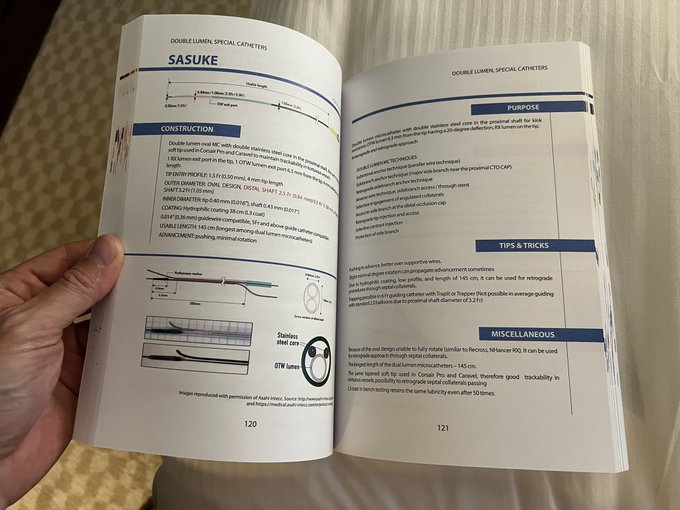
I just put my hands on this bad boy — congrats
@KovacicMihajlo
, a great resource for the
#CTO
geek. Everything ready for
#MLCTO
in Nice, French Riviera 🏖 🇫🇷 😎
@RinfretStephane
@KambisMashayek1
@Avranctotrip

5
11
80
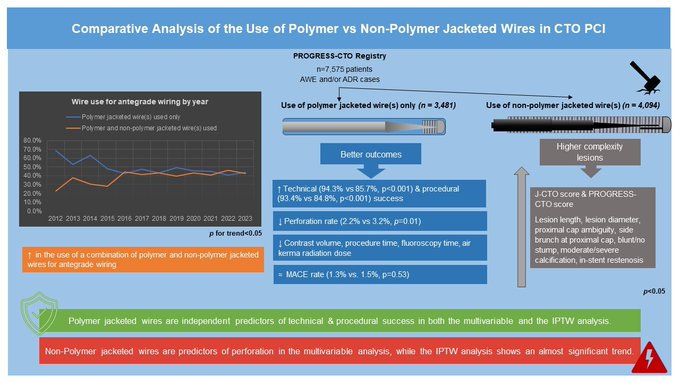
When feasible, avoidance of non-polymer-jacketed wires (PJWs) can improve
#CTO
#PCI
outcomes.
Antegrade procedures in which PJWs were exclusively used had ⬆️ technical success and ⬇️ perforation rates.
@m1chaella_alex
@esbrilakis
@MHIF_Heart
@UWMedHeart
6
21
82
Non-culprit proximal LAD lesion during NSTEMI. RFR 0.95. What should we do?
22
13
80
Seattle,
@UWMedHeart
and
@crfheart
welcome you all to this week long marathon: Fellows/Early Career Interventionalist Boot Camp,
#CompCourse2023
, and
#CTOHybridEvent
.
It’s gonna be great! 😃⭐️💥☀️🎯🌇🏔️🌲⛵️
@DrBillLombardi
@jamiemccabeMD
@ajaykirtane
@KateKearney4
@CJChungMD

3
8
80
Previously failed LAD
#CTO
with non-interv collaterals (J-CTO 3). Masterfully crossed with LAST with Gladius by
@JTiwanaMD
after Pilot 200 knuckle. However, it is a scarcely reproducible technique (we were ready for Stingray). Then usual
#IVL
and DK crush business.
@UWMedHeart
5
14
80
After the live case, it’s business as usual at
@UWMedHeart
— Challenging RCA
#CTO
(J-CTO 4; pt referred from >2000 miles away) extending into PLB. PDA dissected during prior attempt. Knuckle into PLB, Stingray stick’n’drive, then rescue PDA via septals, reverse CART. ✅
7
10
77
It was amazing to share
#CTO
experiences & skills with
@ignamatsant
at his
#VallAcademy
in Valladolid 🇪🇸. 2 days, 7 complex CTOs (ADR, retro, IVL), 8 🇪🇸 interventionalists eager to up their CTO game. Next stop: Córdoba!

0
5
78
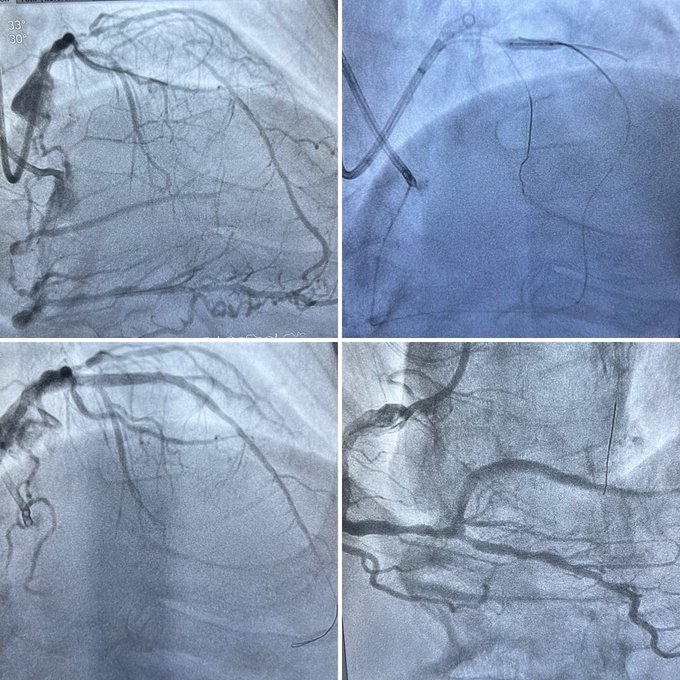
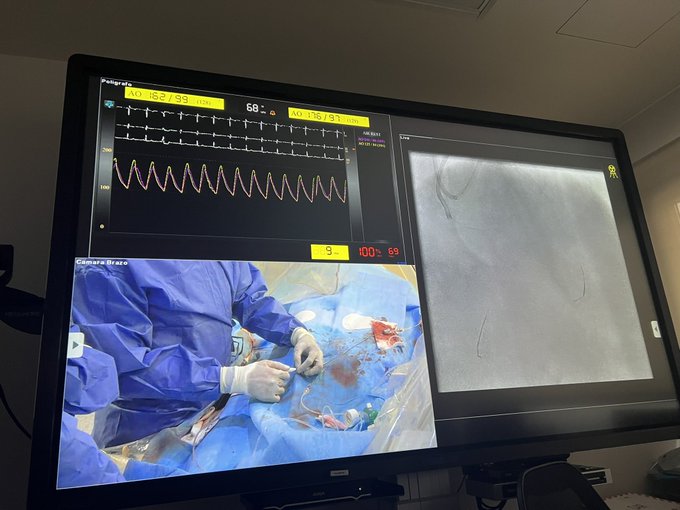
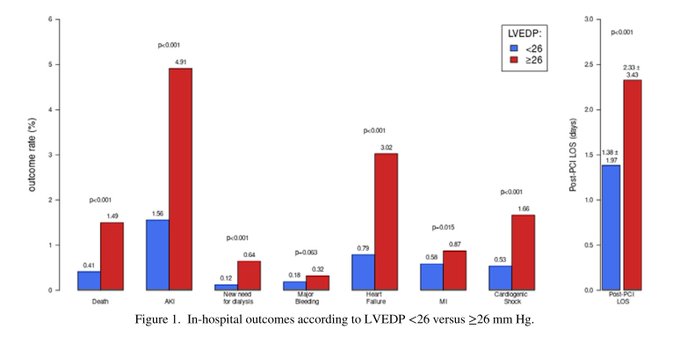
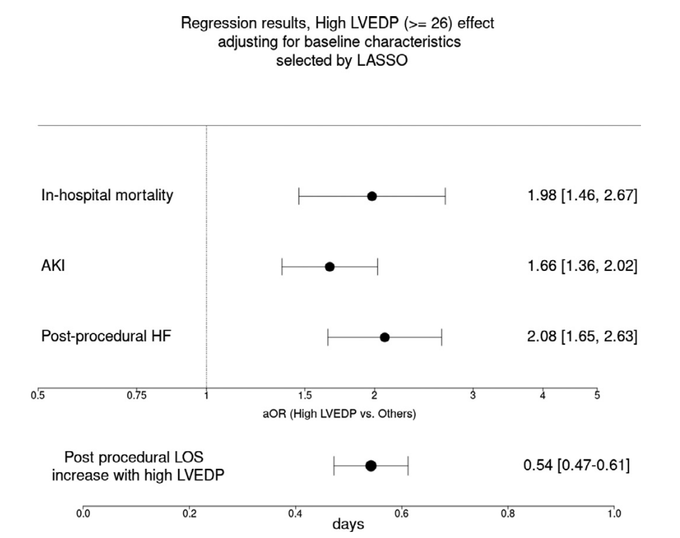
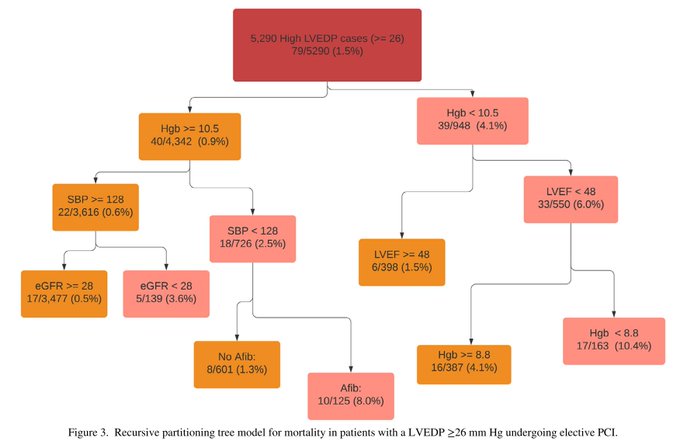
1/3 of pts undergoing elective/urgent PCI have ⬆️
#LVEDP
➡️ higher-risk profile. Death was 2x ⬆️ in pts with LVEDP >18 mmHg. LVEDP was an independent predictor of death, AKI, new HF and longer stay.
@BMC2_
@TCTMD
@UWMedHeart
@UWCardiology
@SCAI
@ACCinTouch
7
18
76
3
18
76
We should stop using death as a (primary) endpoint in
#CTO
#PCI
studies. If PCI in all-comers doesn't improve survival, why should that be the case for CTO patients?
Read the editorial written with
@RezMasoomi
for
#JAHA
.
5
18
75
Previously failed RCA
#CTO
(J-CTO 3), AW first, but extraplaque. Pilot 200 knuckle, STRAW at landing zone (15 ml of 🩸 out!), then Stingray
#ADR
with CP12 (distal visualization with MC in ipsilateral collateral). Great case with
@marcelohr60
@crisguedesb
& F. Hanna in Floripa 🇧🇷
4
7
75
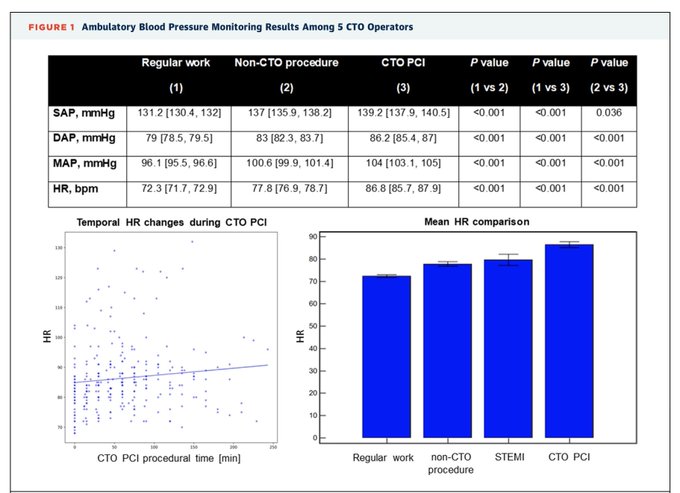
This stuff is stressful, and this is the proof:
#CTO
#PCI
Congrats
@OpolskiMP
for shedding light on this aspect
3
23
74
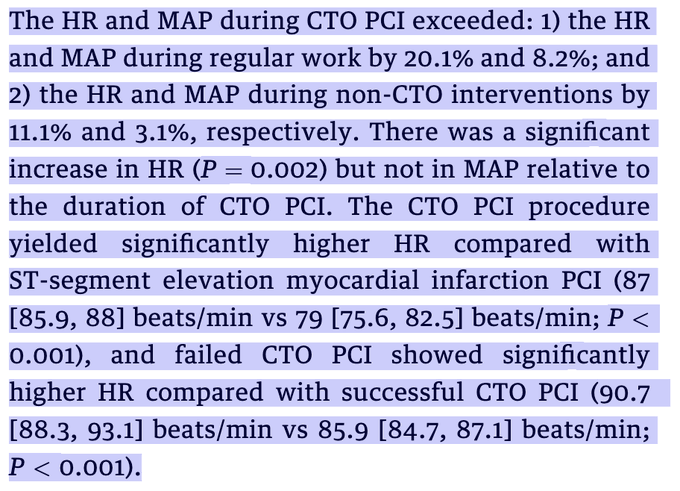
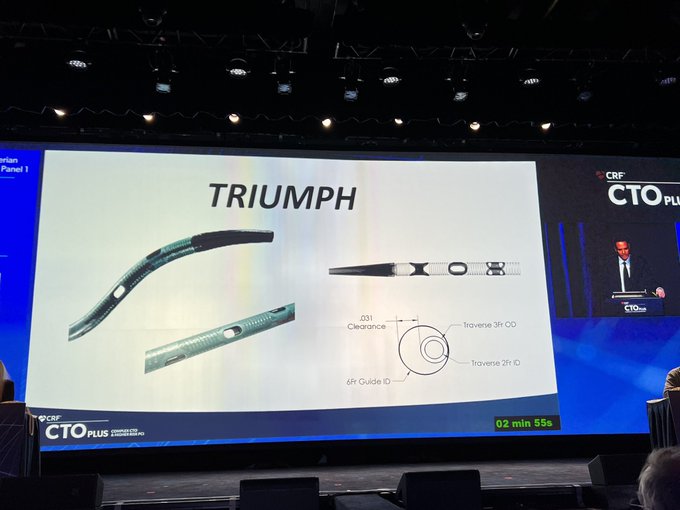
Is the new Triumph device by
@wjn_md
@TeleflexCardiol
going to solve all our
#ADR
problems? Time will tell.
#CTO2023
@crfheart

3
11
72
Have you ever seen a stent more expanded than this? Probably only an adventitial fibroblast between the metal and the pericardium… 😬
11
12
73
Who doesn’t love the floating wire technique to ‘nail the ostium’ of the RCA or LM? 😃 It just works all the times! I learnt if from
@RinfretStephane
, and you?

14
5
72
Orbital
#atherectomy
@csi360
is a valuable option to treat recalcitrant, multilayer
#ISR
due to stent underexpansion. Here, where laser, cutting balloon and IVL had previously failed, OA allowed to reach a reasonable MSA, after ~7 minutes of orbiting (10 long runs).
8
18
73
When you need to cover the (aorto)ostium,
@OstialFLASH
can help.
Here, independent ostium of LCx from aorta, which had to be covered. Stent protrudes in the aorta. Ostial Flash is inflated: mid marker 1 mm inside stent, ball inflates and flares the stent. 👌🏼 🔝 result!
3
15
72
Great addition to the
#CTO
operator armamentarium: PROGRESS-CTO complication scores by
@esbrilakis
and
@BahadirSimsekMD
, published by
@JACCJournals
. You can also read my editorial putting the paper in context.
Article:
Editorial:
3
25
70
Who doesn’t like to work in a place like this?
@UWMedHeart
@UWCardiology
@uwashfellows
@UW
@UWCathLab
@DrBillLombardi
@KateKearney4
@jamiemccabeMD
@CJChungMD

7
3
70
Always satisfying to find out 🤔 what’s the cause of patients’ symptoms, particularly when the reason is uncommon. This middle-aged 🧑 had angina unresponsive to beta-blockers & ranolazine. Severe vasospasm on Ach testing. Normal microvascular function. 💊 changed to verapamil ✅

3
7
69
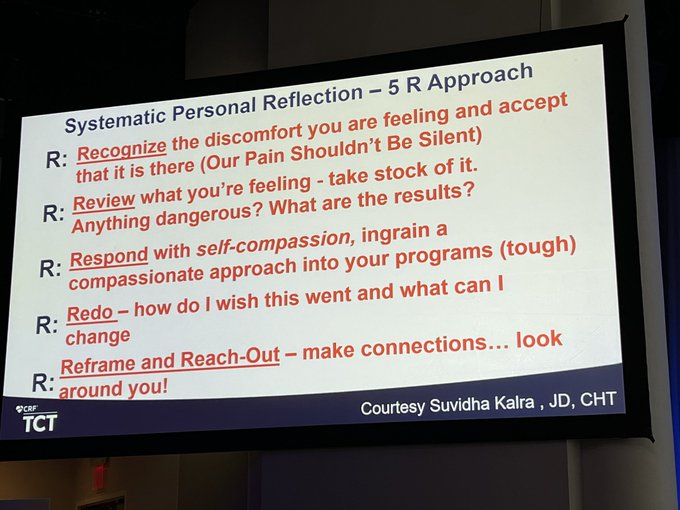
Difficult conversations, occasions for professional and human growth, and emotional moments at
#CTO2024
with
@DrAmirKaki
and
@cardiofrizz
— thanks for being vulnerable and let us learn from your darkest moments.
🙌🏼🤜🏼🤛🏼
@crfheart

1
8
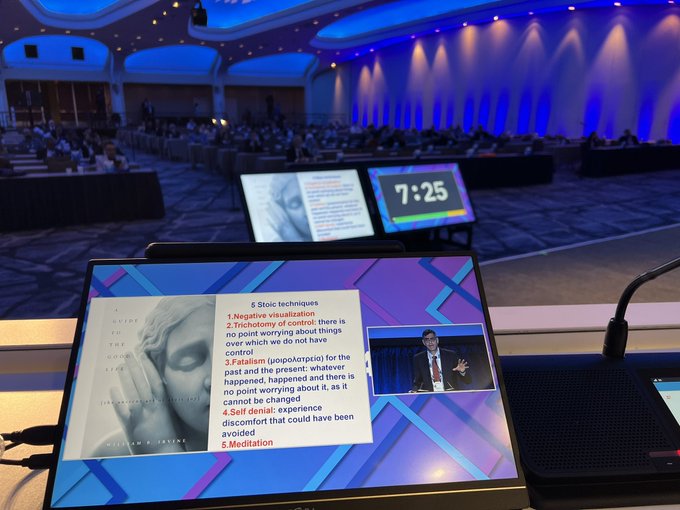
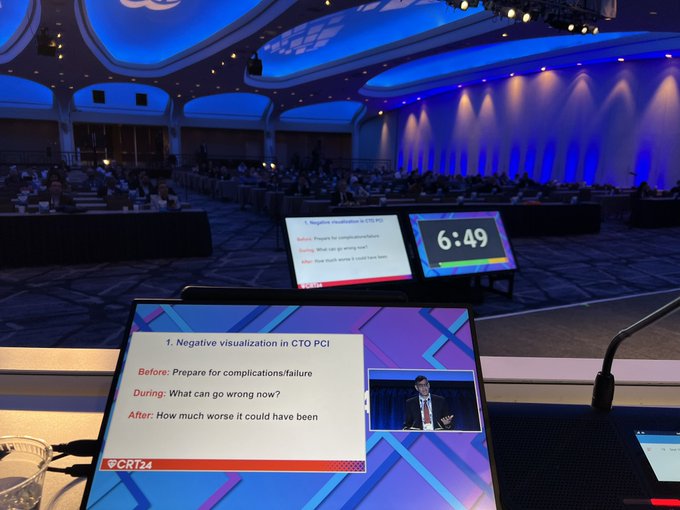
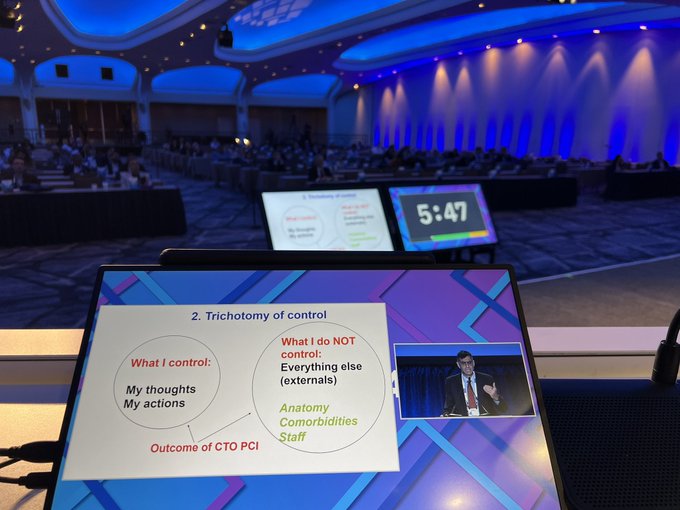
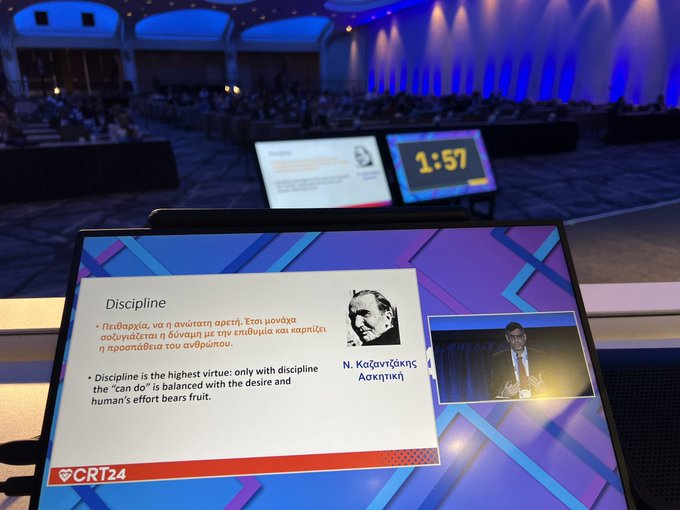
69
Some of us have realized that it’s not only about the technical
#CTO
skills, while also (and foremost) about the mental preparation and leadership skills. Great talk by
@esbrilakis
#CRT2024
@CRT_meeting
Stay tuned for our upcoming article on the topic.
@DrBillLombardi
2
9
69
Pleased to share that our review ‘Contemporary issues in
#CTO
#PCI
’ is the second most read paper published by JACC CV Interventions
@JACCJournals
in 2022.
@rickytiago
@esbrilakis
@DKarmpaliotis
@KambisMashayek1
@RinfretStephane
@wjn_md
@MauroCarlino3
2
12
67
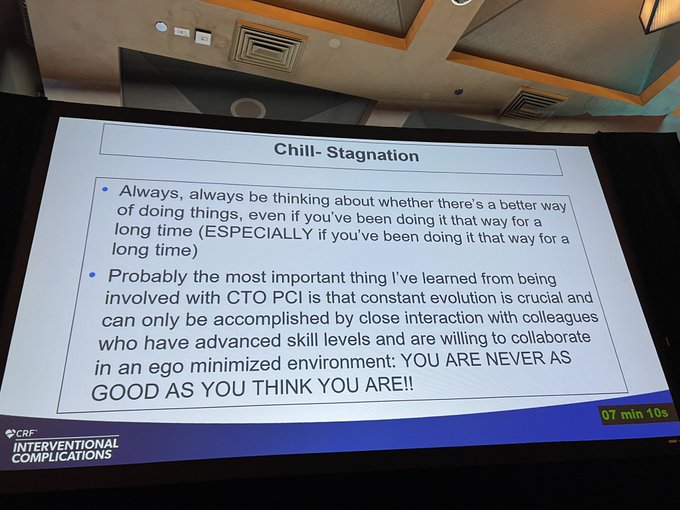
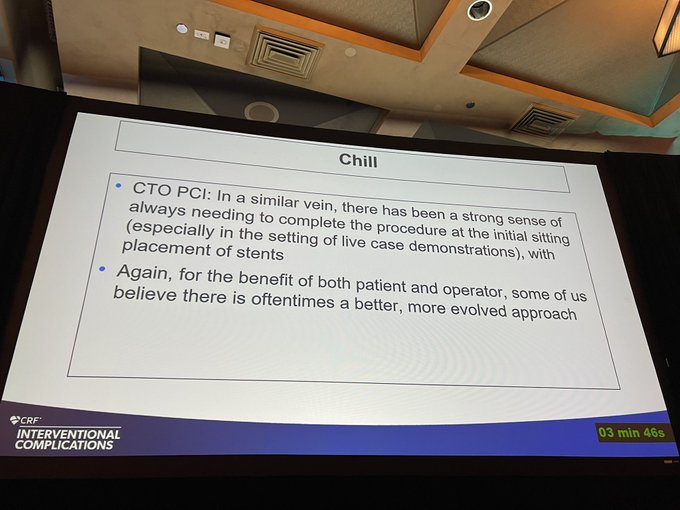
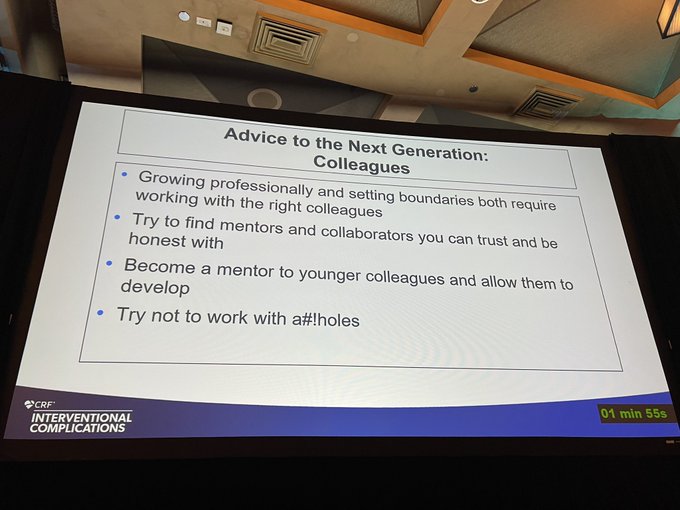
Advice to the next generation at
#CompCourse2023
— ‘what l wish I had done sooner, better, different’
1/4 Mike Wyman — ‘Chill’
7
17
68
What an interesting read.
State-of-the-art, imaging- and physiology-guided
#PCI
optimization.
The way to go.
2
17
67
We’ve been treating an avalanche of flush ostial LAD CTOs recently (5-6 in a month)
@UWMedHeart
. Here, angulated microcatheters like
@TeleflexCardiol
Supercross 120 are key. A couple of examples: 1) Pilot 200 > Gladius Mongo; 2) Gaia Next 3 > Hornet 14. What’s your practice?
3
4
66
Learned a lot at the
#CTO
Academy at
#CRT2022
@CRT_meeting
yesterday. Let’s come back today at 2 pm for more!
@ArasiMaran
@KateKearney4
@SanjogKalra
@A_B_Hall
@esbrilakis
@RinfretStephane
@kevinjamescroce
@FaroucJaffer
@wjn_md

0
10
67
Great experience at the 13th Puerto Rican 🇵🇷 Interventional Cardiology 🫀Society meeting. Successful live case of a complex LAD
#CTO
#PCI
(J-CTO 3) with my friend
@rickytiago
— entirely true-to-true crossing with
#IVUS
guided prox cap puncture and navigation!
0
9
67
1
22
67
As previously stated: get comfortable being uncomfortable. Pushing knuckles against a severely calcified CTO is unsettling. But sometimes it must be done. And it works!
@DrBillLombardi
pushes us all to the limit. 😨💪🏼😃
What a unique experience at
@UWMedHeart
#CTO
Hybrid Event!
1
4
65
What’s happening here?
(Hint: it’s a
#CTO
#PCI
).
@DrBillLombardi
@KateKearney4
@UWMedHeart
@UWCathLab
14
4
63
The most unique ER. Do you know where it is? (that’s an easy one 😉)

14
2
62
What I learnt from my first
#CTO
mentor,
@MauroCarlino3
, is that it’s hard to go against the mainstream belief system. Knuckles and intraCTO contrast injections. Damn the naysayers. Challenge the dogma. 💪🏼
#OMG2022
@ Cordoba 🇪🇸
@MPAOSS
@OjedaOjeda18
0
7
64
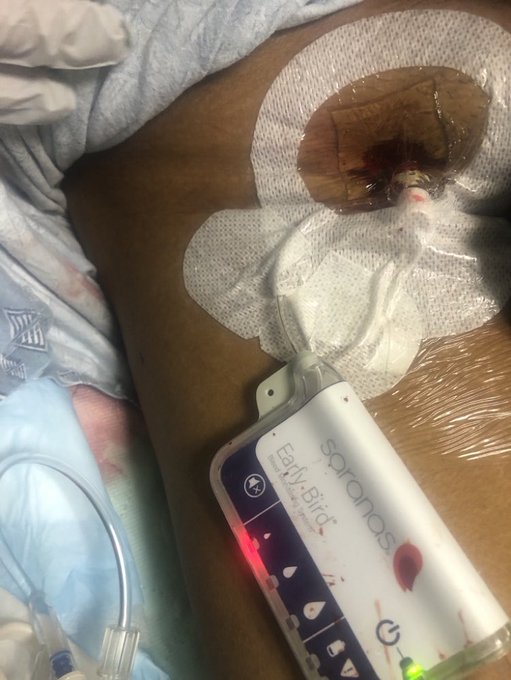
This how we do high-risk
#PCI
with
@abiomedimpella
#Impella
@VCUHealthHeart
: Heart Team discussion, US&fluoro-guided access, RHC &
#imagefirst
in 100%, no angio restriction, aim at
#completerevasc
, final fem angio+
@SaranasInc
Early 🐦 to watch for bleeding. Discharge on POD 1-2.
10
9
64
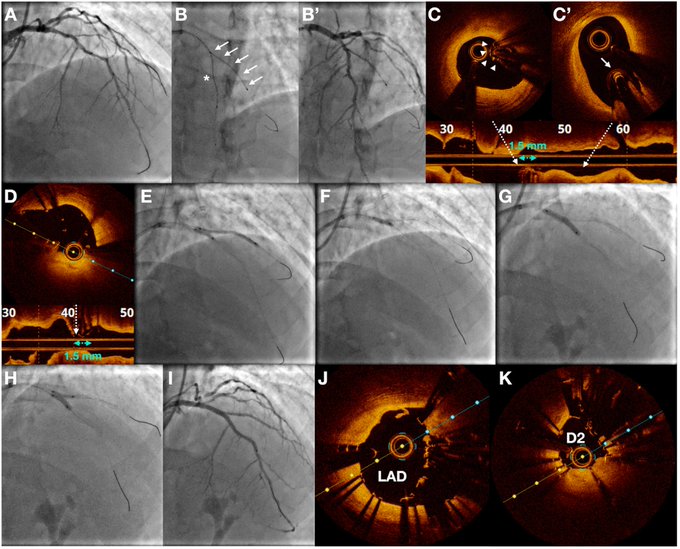
DK
#nanocrush
for
#bifurcation
#PCI
guided by live
#OCT
imaging
Novel application of OCT to guide precise stent positioning during DK nano-crush: simultaneous OCT on MB to locate proximal SB stent edge.
Great teamwork
@FrnMoroniMD
@ziadalinyc
@DrAllenJ
3
12
60
Coronary perforation, subepicardial hematoma, and tamponade after
#CTO
PCI.
Perforation caused the initial lesion to expand by a self-propagating mechanism: hematoma avulsed the capillaries that fueled its expansion through a tear into the epicardium.
1
10
63

Another day taking care of complex pts
@UWMedHeart
. Ostial LM treated with
#orbital
#atherectomy
. Recalcitrant 2-layer RCA
#ISR
fixed with
#rotational
#atherectomy
& brachytherapy. ‘No option’ MV CAD with LAD CTO & LVEF 30% received
#completerevasc
with
#percax
#Impella
.
3
4
62




Great team of women in intervention
#WIC
@WomenAs1
performing a complex case
@UWCathLab
@UWMedHeart
— great job
@JTiwanaMD
, Dr. Pristera & Molly

1
11
60
4 complex cases done by 4:30 pm
@UWMedHeart
:
1) multivessel
#PCI
(with OM
#CTO
)
2) RCA
#CTO
#PCI
with orbital
#atherectomy
3) LAD-D1 orbital
#atherectomy
and DK crush
4) LM-LCx orbital
#atherectomy
and provisional
All patients doing well and happy. Strong 💪🏼 teamwork.

2
4
60
Indirect ‘suggestion’ that
#ultrasound
-guided
#femoral
access alone doesn’t reduce minor/major
#bleeding
compared with fluoroscopy guidance. You also need
#micropuncture
kit.

10
18
57
Very active 90 yo with CCS 3 angina and LAD
#CTO
. LAD opened, angina goes away. Patient was very happy that he got his QoL back, when I saw him in clinic. Sometimes, age is just a number!
@UWMedHeart
@agtruesdell

5
10
59
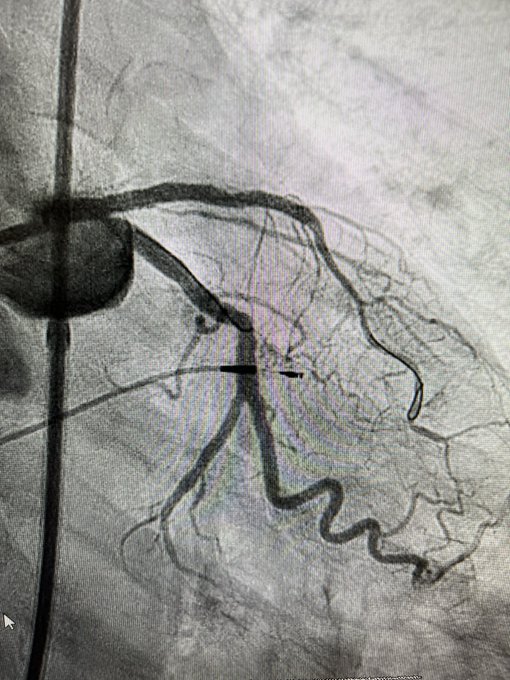
How to use subintimal tracking and re-entry (STAR) to seal
#perforations
during
#CTO
#PCI
.
Congrats to
@JTiwanaMD
for leading this project, together with
@thinkmdkane
and
@KateKearney4
. Another 🌟 for
@UWMedHeart
.
@CRMjournal
1
18
59