
Sanjeev Sethi
@SethiRenalPath
Followers
14K
Following
3K
Media
474
Statuses
2K
Professor, Pathology, Mayo Clinic, MN. 💯 clinical. Renal pathology. Use X to teach, clinical info changed=protect confidentiality. Love dogs. Views are my own.
Minnesota, USA
Joined January 2018
A very happy and proud moment for me. Our son Amit started medical school at the University of Minnesota Medical School- Primary Care education at its best. @umnmedschool

60
10
630
You need to go the extra step. - Do pronase IF & IgG subtypes in MPGN cases, esp when etiology is unknown. - I wonder about idiopathic IC-MPGN, how many are IgG3 PGNMID. - I also wonder if IgG3 PGNMID are truly monotypic, as we never find the B/plasma cell clone in most cases.
3
3
22

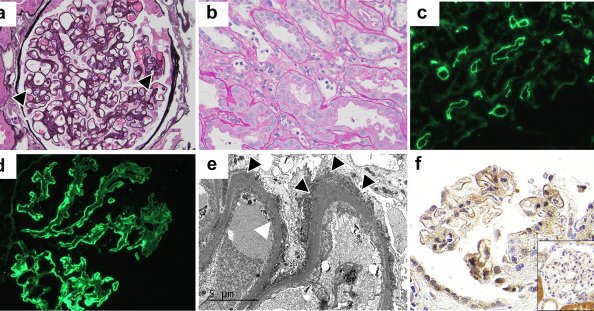
Baffling: PGNMID, monoclonal no more. I got this consult case as immune complex-MPGN. LM- MPGN pattern.IF- IgG, C3, C1q, kappa & lambda 3+. Did IgG subtypes-IgG3 3+, all others negative. EM- mottled deposits. Dx- Proliferative GN, IgG3, but ? with monoclonal IgG deposits (PGNMID)

6
32
99
Always a joy teaching around the microscope. Yesterday morning with fellows from Italy, Portugal, Brazil, Chile, and USA. I worry that teaching around the microscope will become obsolete with the advent of digital pathology.

2
7
99
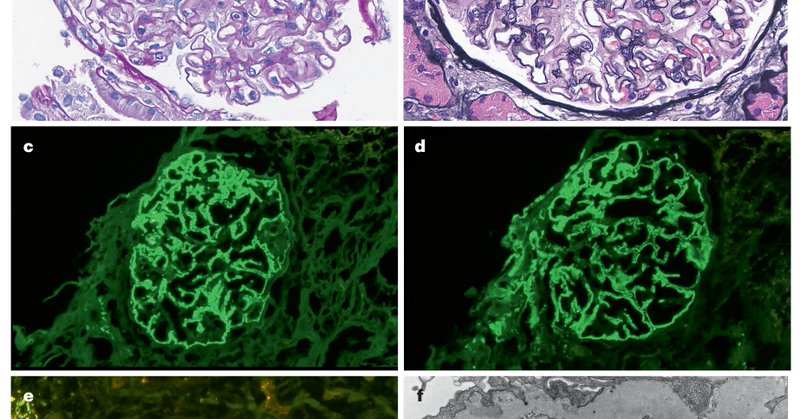
FAT1 is not increased in prior protocol biopsies until development of ABMR and MN. In control cases, FAT1 does not increase in ABMR alone if there is no MN. 2/2.
0
2
13
FAT1 is the target antigen in membranous nephropathy associated with-.1. Stem cell transplant (HSCT). 2. Antibody mediated rejection (ABMR) in allograft. In this paper we show a temporal ⬆️of FAT1 in MN with ABMR using protocol & for cause biopsies. 1/2.
kireports.org
Membranous nephropathy (MN) of the kidney allograft can represent recurrent, de novo, and very rarely, donor-derived disease. Despite its negative impact on allograft survival,1 our understanding of...
1
42
95
RT @NatRevNeph: Antigens in membranous nephropathy: discovery and clinical implications
nature.com
Nature Reviews Nephrology - Since the discovery of PLA2R, several target antigens associated with membranous nephropathy have been identified. This Review describes the distinct clinical...
0
36
0
I started working on MN antigens 7 years ago & had no idea where it would take me. My simple hunch was that a unique antigen could be detected by mass spectrometry performed on dissected MN glomeruli. Never be afraid to work on a hunch. It has been a rewarding journey. 2/2.
1
2
38
Membranous nephropathy has undergone a paradigm shift due to the discovery of unique MN antigens. MN has gone from idiopathic to ➡️ primary vs. secondary ➡️ where an antigen can be detected in ~80% of MN. This is a comprehensive review of each antigen.
nature.com
Nature Reviews Nephrology - Since the discovery of PLA2R, several target antigens associated with membranous nephropathy have been identified. This Review describes the distinct clinical...
6
89
206
Laser microdissection and mass spectrometry (LMD/MS) is a sensitive one stop methodology for detecting large number of MN antigens. 3/3.

Mayo Clinic Laboratories' new mass spectrometry assay requires just one small tissue sample to identify 13 antigens known to cause membranous nephropathy. Learn more about this one-stop test. @SethiRenalPath.
0
2
11
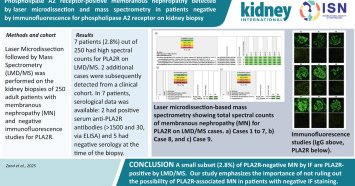
Important to realize we detected 3 cases of PLA2R + MN by LMD/MS, even though they were negative for serum anti-PLA2R antibodies. Starting point: 25 MN.12 (48%) PLA2R + MN.13 (52%) PLA2R - MN; antigen detected in 8 of 10 cases where tissue was available.2/2.
1
0
10
Membranous nephropathy (MN) antigens from a single center in Portugal. Starting point=negative serum anti-PLA2R titer cases. We detected MN antigens: 3 PLA2R, 2 NELL1, & 1 each EXT1/EXT2, HTRA1, THSD7A. Antigens correlated with underlying disease. 1/2.

kireports.org
Membranous nephropathy (MN) is a rare autoimmune disease affecting individuals of all ages, standing as the primary cause of adult nephrotic syndrome and carrying significant disease burden.1
3
29
85
RT @mayocliniclabs: Mayo Clinic Laboratories' new mass spectrometry assay requires just one small tissue sample to identify 13 antigens kno….
0
20
0


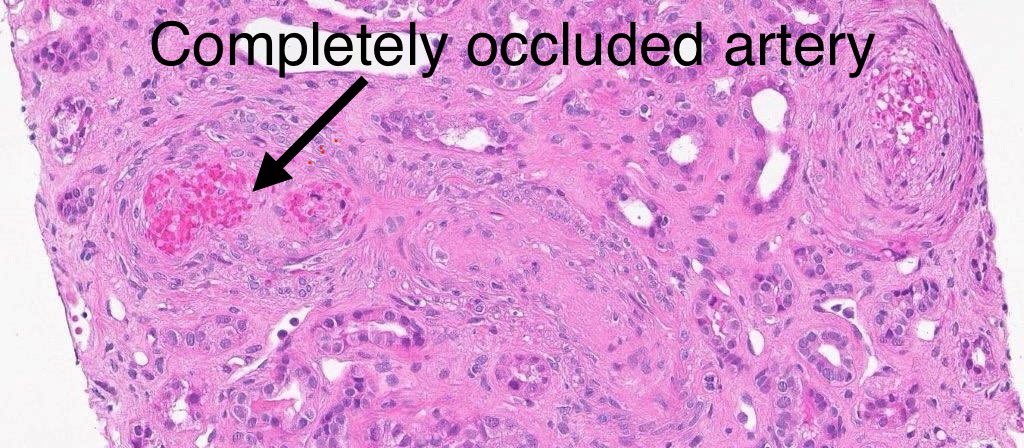
Methamphetamine abuse=severe thrombotic microangiopathy. Unfortunate weekend case 😢. Glomeruli: mesangiolysis +++ & ischemic changes .Interstitium: Hemorrhage, inflammation & scarring.Vessels: Severe sclerosis, thrombosis, schistocytes. 40-yr woman, hypertension, AKI, meth abuse



2
49
143
RT @PepaSolerR: 📣📢 “𝟏𝐫𝐬𝐭 𝐌𝐚𝐲𝐨 𝐂𝐥𝐢𝐧𝐢𝐜 - 𝐕𝐚𝐥𝐥 𝐝’𝐇𝐞𝐛𝐫𝐨𝐧 𝐍𝐄𝐏𝐇𝐑𝐎𝐋𝐎𝐆𝐘 𝐔𝐏𝐃𝐀𝐓𝐄” save the dates 5-6 Sep Barcelona 2025. Register to mundicongres@mun….
0
28
0
Sorry I accidentally deleted the original post while trying to answer some questions. I’m still a novice with X 😁. Take home message: small ~3% of PLA2R negative MN cases by routine IF are PLA2R positive by LMD/MS.
kidney-international.org
Membranous nephropathy (MN) is characterized by subepithelial deposition of immune complexes along the glomerular basement membrane. The muscle-type phospholipase A2 receptor (PLA2R) has been...
3
21
76
LMD/MS was done on PLA2R negative MN cases to find the underlying antigen for discovery of NELL1, EXT, FAT1, NDNF, etc. by our group. As a side story we found that ~3% of cases that we thought were PLA2R neg turned out to be PLA2R ➕ by LMD/MS. That is the message of our paper.
0
5
11
RT @andreaangioi: 🌍 ERA Congress 2025 – Vienna.🧠 Focus: Membranous Nephropathy. An inspiring session chaired by Ingeborg Bajema & Michael R….
0
12
0
Gian Marco- It was wonderful having you train with us. Seven months went by quickly-you were at every renal pathology sign out with me. You never missed my weekend sign out taking every opportunity to learn. Wish you all the best for your future. Safe travels to Bologna 🇮🇹

1
3
32