
Caspian Kuma Folmsbee MD
@FolmsbeeMD
Followers
303
Following
829
Media
79
Statuses
1K
internist - primary care - assistant professor | - (Salary 233k + RVU bonus) - no other COI
Joined June 2009
Living thread of lessons learned after attempting primary care academic medicine since 2013--🧵
3
5
21
Agree about poor sens and spec but improving it requires dedicated independent feedback which is not done nor practical. Also, HPI >>> PE, especially with continuity care.

If the physical exam were a lab or image test, we’d never order it. Not sensitive or specific enough. Yet there are those that hold onto these quaint ideas about the exam. And I do an exam. Focused. I won’t be counting moles or look at your pubic hair distribution. But. For
0
0
1
Thanks for the source. The score increase makes sense, I would assume there would corresponding decrease in competitiveness in derm.

Actually, economists have modeled this. The answer is, USMLE scores for internal medicine residents would increase by around 0.5 standard deviations.
0
0
1
Since everyone always talking about low compensation for primary care, what would happen if overnight, primary care got a 200K raise cross the board? @jbcarmody
3
0
12
This sounds fine in theory but does the primary lit even exist for this granular of data? In my experience the biggest issue with LR model for diagnosis is the lack of well done primary diagnostic lit

WRONG WAY: use likelihood ratios derived from binary cutoffs of continuous test results (ie D-dimer >500) CORRECT WAY: use interval likelihood ratios (e.g 500-750)
1
0
1
I don’t know. Reads more like ad copy for a company. I’m bullish on AI like you are but chart summary is not a bottleneck for me. Not to mention GIGO.
Amazing Disruptive Beyond value add
1
0
0
Which emphasizes the need to reexamine our cancer screening programs to focus on clinically significant cancer and not on all cancer.

We will face a shortage of oncologists as projected cancer cases rise and number of oncologists decreasing relative to demand. 25% of oncologists are 64y and older. Number of oncologists currently on pace to meet only 29% of demand in next 12 years. Gaps will widen.
0
0
1
This data will be out of date in six months. Orlistat and Natr-Bupr are not even worth it.

Newly published treatment algorithm for the pharmacologic treatment of obesity and its complications, from the European Association for the Study of Obesity (EASO) ⚕️ Semaglutide and tirzepatide are recommended as first line to treat obesity AND to treat underlying
0
0
0
My prior is high though that average physician is unable to appraise and apply to patient care safely and given the poor overall quality of trials, it is perhaps better for them to focus on knowing guidelines practically speaking
Guidelines are neither scripture or always evidence-based, and slow to updating Think of all the harm by waiting not to adopt good evidence
0
0
2

Ok. Rule 1 of @X -> listen to @AndrewFoy82 he’s one of the strongest thinkers in all of cardiology

I disagree with my friend's take. These aren't patients who would've been included in the clinical trials. There are reasons to be concerned about safety in these vulnerable patients. IMO good use of observational study design and potentially V important findings. Hypothesis
2
4
27
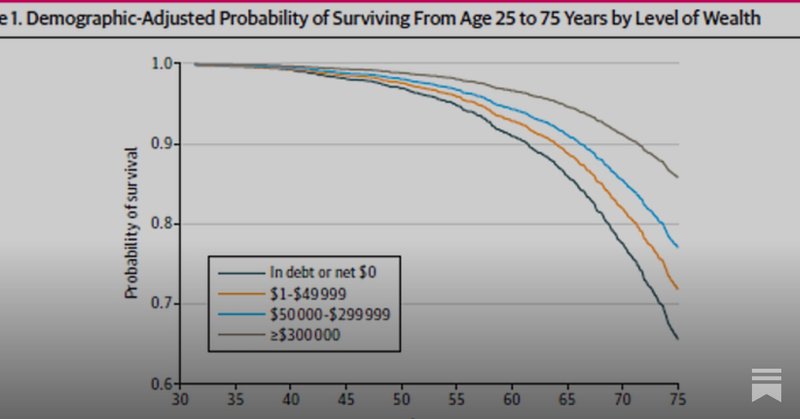
This just confirms that primary care medicine needs to get out of the “longevity” field. Just let health coaches get paid by affluent people if they want.

I host Dr. Patel founder of LV8 https://t.co/cIsr6kLDcp who proposes “Medicine 3.0” an approach that maximizes “health span” & maybe longevity? Can we move primary care from reactive to proactive? Hear what Anand has to say & join the conversation. Link: https://t.co/bW0SboKepZ
0
0
0
🧐🙄😢

Clinicians can enhance patient understanding by using numerical data instead of verbal probabilities, consistent denominators, absolute risk comparisons, and clear context for unfamiliar data types. https://t.co/KiransABeb
0
0
1
90% specificity and 41% sensitivity is terrible for a widely implemented screening test.

The white paper from Apple on the Apple Watch hypertension feature indicates solid specificity, as expected. This is at the expense of sensitivity, which generally makes sense. I agree with prioritizing flagging putative hypertension diagnoses where there is greater confidence.
1
0
0
@adamcifu Sensible Medicine Post https://t.co/oCknwVkFuo
sensible-med.com
Ten topics that do not need to be studied
0
0
0
Shout out to @adamcifu for referencing this paper in his sensible medicine post. I read it! (Both posts below) https://t.co/cgcomI5agF
https://t.co/X2MgyIAGfs
sensible-med.com
Ten topics that do not need to be studied
1
0
1
Strongly agree. This is the way.

Thought provoking piece in BMJ. Should we spend less time on primary prevention to spend more time to treat the sick. Would love to know the thoughts of sensible medicine @adamcifu
@drjohnm
https://t.co/KN6Dle2SCt
0
0
0
Hypermedicalization of life. Majority of patients will ignore, a minority will swallowed up by the medical nemesis.
0
0
0
Now compare it with spironolactone.

Finerenone Across the Spectrum of Kidney Risk in Heart Failure: The FINEARTS-HF Trial Finerenone appears to consistently improve clinical outcomes, HF-related health status, and albuminuria across a broad spectrum of kidney risk in patients with HF with mildly reduced or
0
0
0
Clearly AQUATIC author priors thought there would be benefit given 25% RRR assumption for analysis. Maybe we need an M&M on COMPASS and others.
0
0
0
Drug A works vs placebo Drug B works vs placebo Drug A+B works vs placebo. What exactly did we learn? https://t.co/OQxlLCfsWn
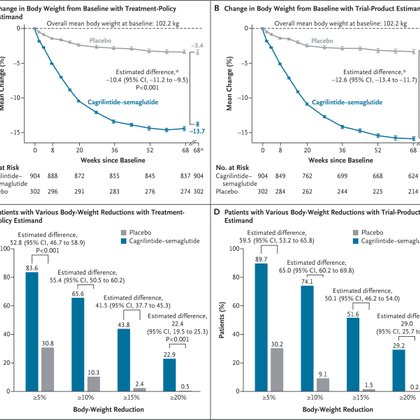
nejm.org
Cagrilintide and semaglutide have each been shown to induce weight loss as monotherapies. Data are needed on the coadministration of cagrilintide and semaglutide (called CagriSema) for weight manag...
0
0
0