

Helbert Rondon, MD, MS, FACP, FASN, FNKF
@NephroMD
Followers
6,693
Following
968
Media
441
Statuses
5,633
Nephrologist @UPMC l Professor of Medicine @PittDeptofMed l Fellowship PD @Pittrenal | Tweets/retweets are my own #Hyponatremia
Pittsburgh, PA
Joined April 2009
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
Fenerbahçe
• 635770 Tweets
#RafahOnFire
• 374417 Tweets
Memorial Day
• 180011 Tweets
Şampiyon Galatasaray
• 126671 Tweets
#GazzeKanGölü
• 109264 Tweets
Admin
• 99258 Tweets
#مجزره_رفح
• 78172 Tweets
Ali Koç
• 63306 Tweets
خيام النازحين
• 53408 Tweets
Allah'ım
• 49412 Tweets
İsrail
• 45373 Tweets
#رفح_الان
• 35072 Tweets
Fermin
• 34801 Tweets
Ankaragücü
• 33759 Tweets
Ronaldinho
• 27994 Tweets
Ludmilla
• 25667 Tweets
Ergin Ataman
• 24137 Tweets
Trabzon
• 22771 Tweets
Ya Kahhar
• 20347 Tweets
Larson
• 18845 Tweets
ドラクエの日
• 17903 Tweets
Amaral
• 13202 Tweets
東京都知事選
• 12596 Tweets
Ya Rabbi
• 12394 Tweets
Moisés
• 10913 Tweets
Rodrigues
• 10008 Tweets





















🤯Nonsense. Who is the medical consultant for these TV shows?
133
155
2K
Do you want to hear sodium joke ? Na!
Do you want to hear a potassium joke?
K!
31
297
1K
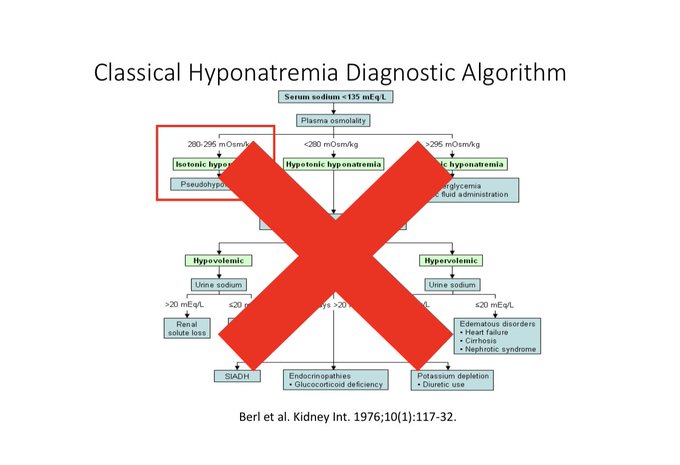
Understand the physiology to forget the algorithm
1
89
435
Potassium replacement should be considered when correcting hyponatremia, especially severe (<120 mEq/L). The rule of thumb is 1 mEq of KCl is approx. equal to 2 mL of 3% saline. KCl solution should be concentrated. We use 20 mEq/50 mL formulation (400 mM vs. 513 mM of 3% saline).
4
85
368
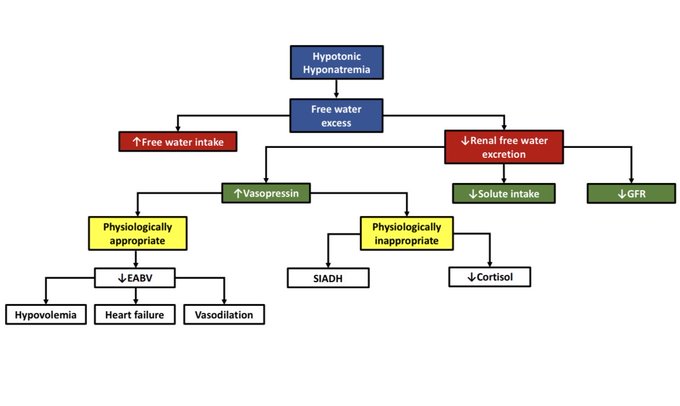
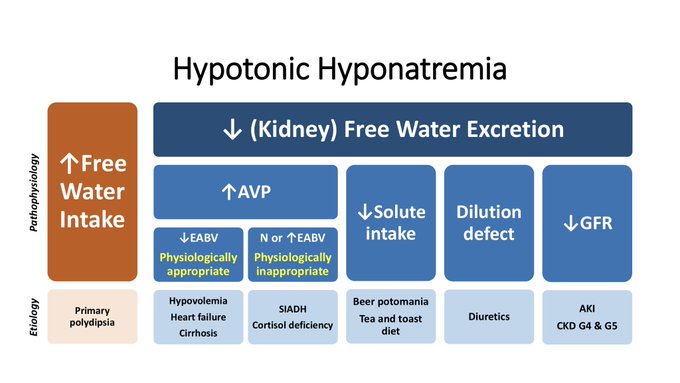
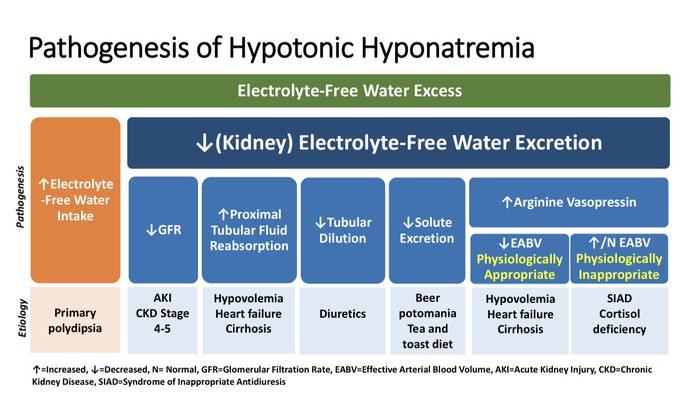
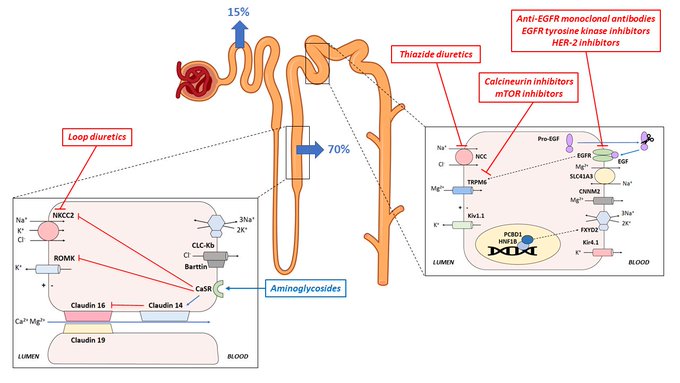
Updating my pathophysiology of hyponatremia slide for a talk. Thanks
@swissnephro
for the art inspiration.
8
78
367
1/A former fellow sent me a text this afternoon “Hello. Covering service. Patient presented with PNa of 111 with pre renal azotemia. Bicarb 6. Currently on bicarb gtt and volume resuscitation. PNa 12 h later is 126. ICU doc says latest evidence says no risk of ODS per NEJM.”
14
117
272
Annual Frailey lecture by Lisa Satlin.
7
19
263
Syndrome of Inappropriate Antidiuresis: From Pathophysiology to Management | Endocrine Reviews | Oxford Academic

0
73
210
Time for a
#tweetorial
on “Desalination” in SIADH. Why normal saline (NaCl 0.9%) makes the
#hyponatremia
from SIADH worse?
11
86
198
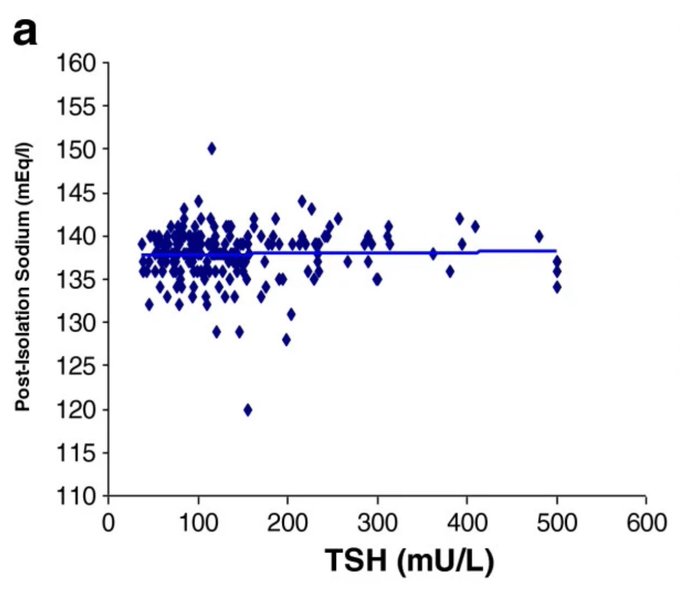
Who says hypothyroidism causes hyponatremia?
5
46
200
Time for another
#tweetorial
on fluid restriction in
#hyponatremia
from SIADH. Is there a way to predict which patients with SIADH will respond to fluid restriction?
8
86
198
Before Twitter goes into cardiac arrest, remember: hyponatremia …no algorithms, just physiology
5
24
170
Our manuscript “Hyponatremia Demystified: Integrating Physiology to Shape Clinical Practice” in collaboration w/
@ChristCrain
@bdubNephro
@priti899
is now available online
@ackdonline
@PITTRenal
@pittkidneyctr
@ClinNeuroEndo
@MDACC_RenalSec
#hyponatremia
9
58
176
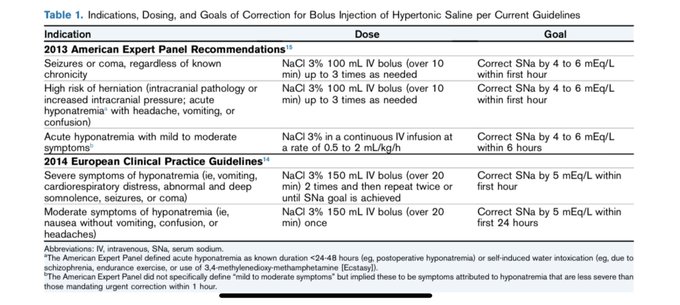
NaCl 3% bolus therapy as emergency treatment for severe hyponatremia: Comparison of 100 ml versus 250 ml. | The Journal of Clinical Endocrinology & Metabolism | Oxford Academic

4
53
178
I developed video lectures as a part of a
#FlippedClassroom
on
#hyponatremia
for our IM residents. I am going to be posting one of those videos every week. This is Lecture
#1
: Basic Physiology of Sodium/ECF Volume Homeostasis.

12
61
164
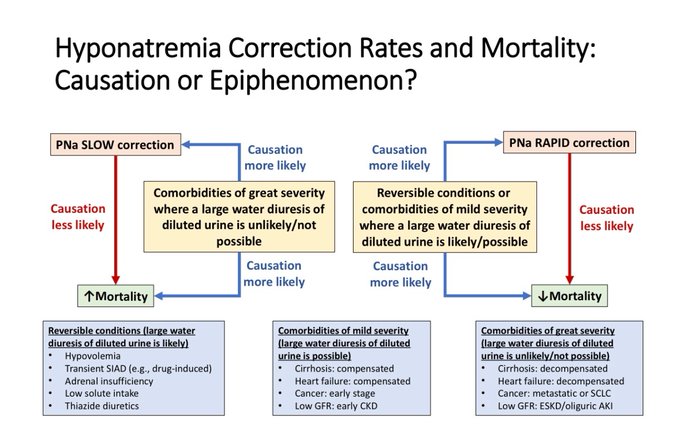
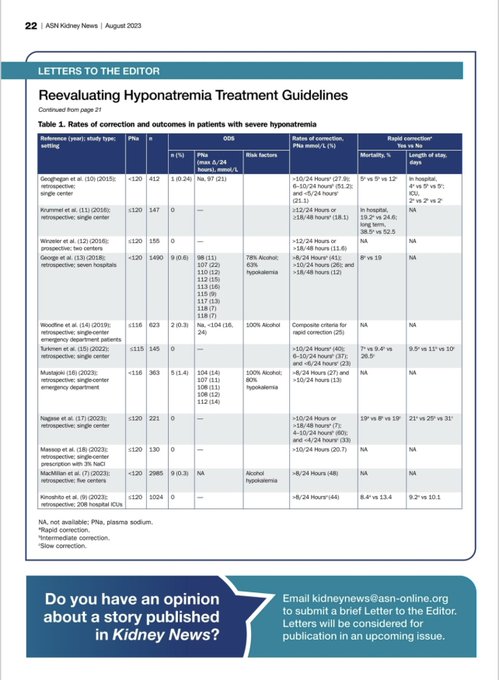
It is implausible that a few mmol/L change in PNa is responsible for fatalities. It is far more likely that underlying comorbidities and their severity is responsible for mortality observed.
#hyponatremia
4
55
159
My review on
@CJASN
on “Therapeutic Relowering of Plasma Sodium after Overly Rapid Correction of Hyponatremia: What is the Evidence?”
#hyponatremia
is now available:
6
63
147
My fellows gave me this gift. Love it! Thanks
@AravindCheruku1
@kkalra_22
@siddverma96
@ripudamanmunjal
@drnawras1986
@IvyM808
7
3
148
@AvrahamCooperMD
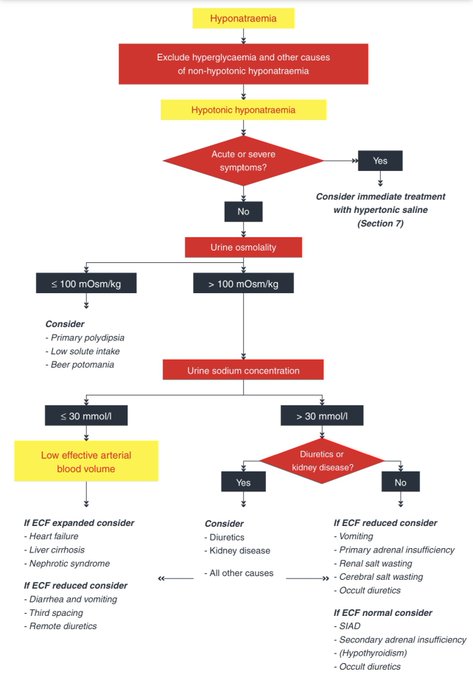
This is the traditional algorithm that hopefully most physicians are moving away from. Recommend instead a physiological approach as shown in the 2014 European practice guidelines.
5
27
142
@MunerMohamed1
There is no way this patient is not volume depleted from glucosuria-induced osmotic diuresis but with much more urinary water than sodium losses. His corrected Na is actually 187 and his total body K is in the tank. I would start with LR + KCl
3
2
140
The Safety of Intravenous Peripheral Administration of 3% Hypertonic Saline: A Systematic Review and Meta-analysis - ScienceDirect
7
40
129
24 specialists from 20 institutions across 🌎 just published a review in
@CJASN
urging caution & adherence to
#hyponatremia
correction guidelines. Motivated by concerns over uncritical acceptance of a recent study & its editorial

7
51
119
1/ I find the over reliance on the Adrogue-Madias (AM) formula to predict SNa changes after infusion of a specific IV fluid astounding.
#hyponatremia
tweetorial
2
51
117
Hypertonic Saline for Hyponatremia – AJKD Blog

3
37
112
First official day as Nephrology Fellowship Program Director
@PITTRenal
. Will do our best to continue the legacy of
@jamierj2
. Big shoes to fill!
15
4
110
1/How do kidneys excrete acid? Kidneys get rid of acid mainly via the excretion of NH4+ and titrable acids. But what would happen if the main way to get rid of acid would be via free H+ excretion?
4
36
110
Running a clinical trial is 20% science and 80% logistics
5
8
109
Honored and excited to become part of the editorial board of
@CJASN
. Thanks
@rajmehrotra1122
for the opportunity.
16
3
105
Who killed Bruce Lee? The hyponatraemia hypothesis | Clinical Kidney Journal | Oxford Academic
1
39
96
Balanced Multielectrolyte Solution versus Saline in Critically Ill Adults | NEJM

4
26
96
How do you correct hyponatremia?
Luis Fonsi: “Despacito”
Fohgat: “Slow ride, take it easy”
The Supremes: “You can’t hurry Na, you just have to wait”
2
12
97
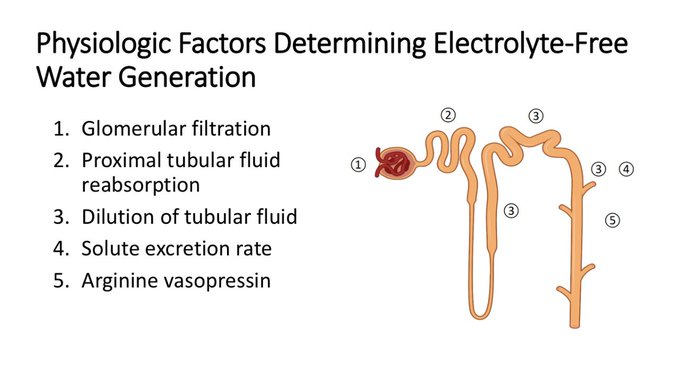
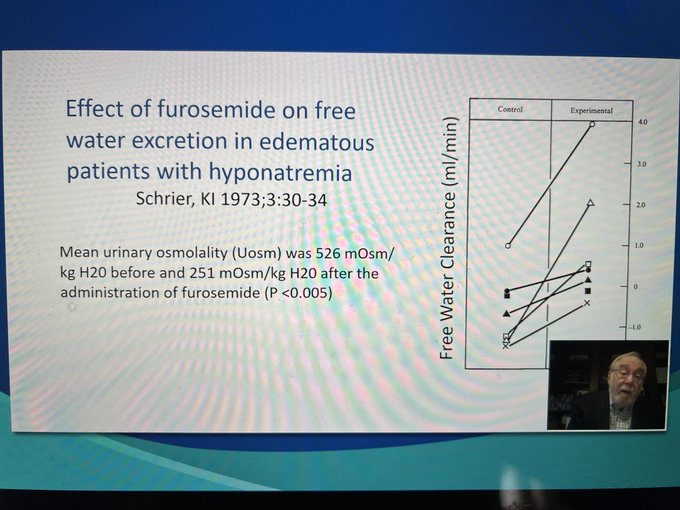
Determinants of Electrolyte-Free Water Generation
2
22
97
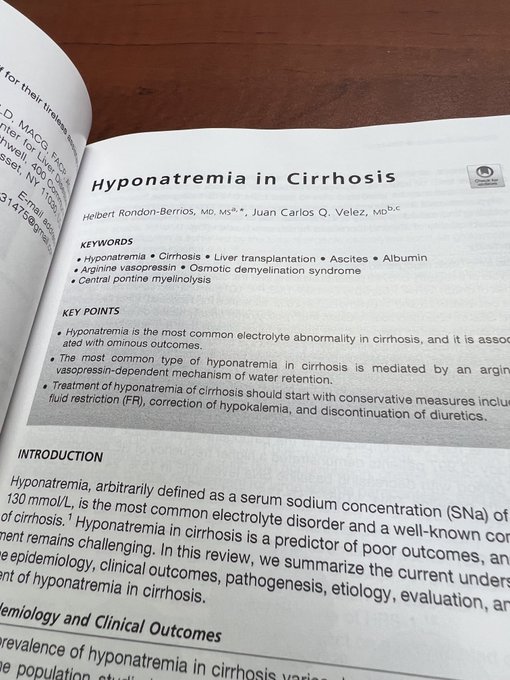
Happy to share that our review of “
#Hyponatremia
in Cirrhosis” in collaboration with all-things-liver aficionado
@VelezNephHepato
published in Clinics in Liver Disease is now available online
#livertwitter
8
42
97
I succesfully defended my thesis this morning and earned a Master of Science degree in Medical Education
16
6
87
How do you treat patients with hypernatremia and hypervolemia?
No H20 bc of hypervolemia
87
Water
289
Water plus a diuretic
1165
Other (explain)
170
27
21
91
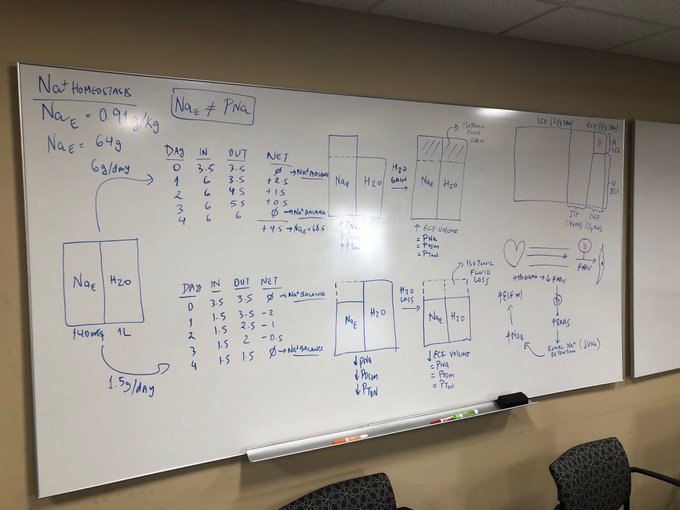
Preparing the board for a chalk talk on hyponatremia (part 1).
7
8
88
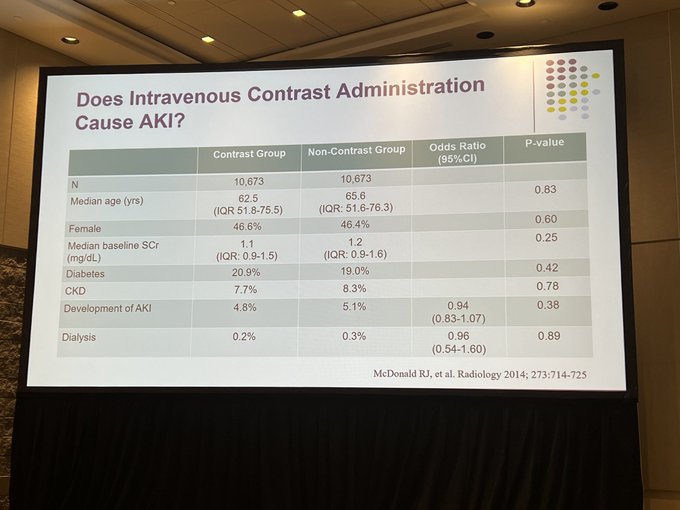
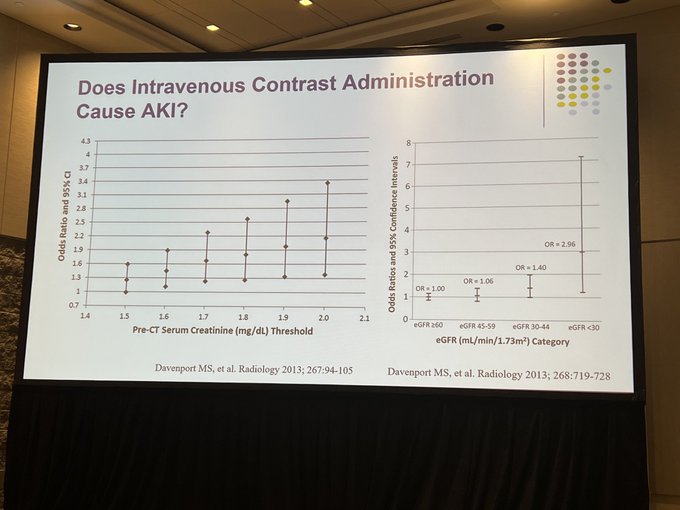
Does contrast associated AKI exist? risk is less these days but, yes, it does
@PaulPalevsky
#KidneyWk
3
24
88
SA-PO1035- Leaving a urine sample for a week, and at a room temperature does not alter the microscopic findings in urine sediments. Important findings from
@serenellaavelez
and
@VelezNephHepato
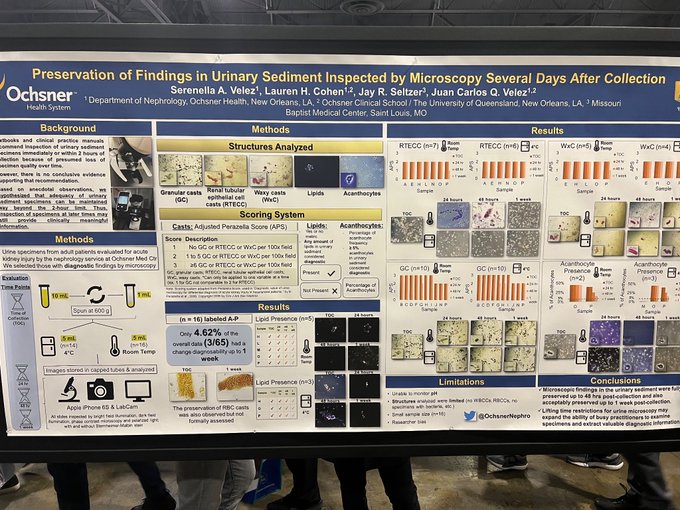
7
25
92
My 3rd video lecture of the
#ElectrolyteClub
series on
#hyponatremia
. Lecture 3: Pathophysiology and Etiology of Hypotonic Hyponatremia - Part 1.

1
21
83
Our new study "Osmotic Demyelination Syndrome Following Correction of Hyponatremia by ≤10 mEq/L per day" in collaboration with Richard Sterns and my former fellow , Srijan Tandukar
@Tandukar702
@PITTrenal
is now available in
@ASNKidney360
#hyponatremia
1
32
81
Today I saw my 4th case of severe symptomatic hypocalcemia from denosumab used to to treat osteoporosis in a patient with advanced CKD.
15
12
83
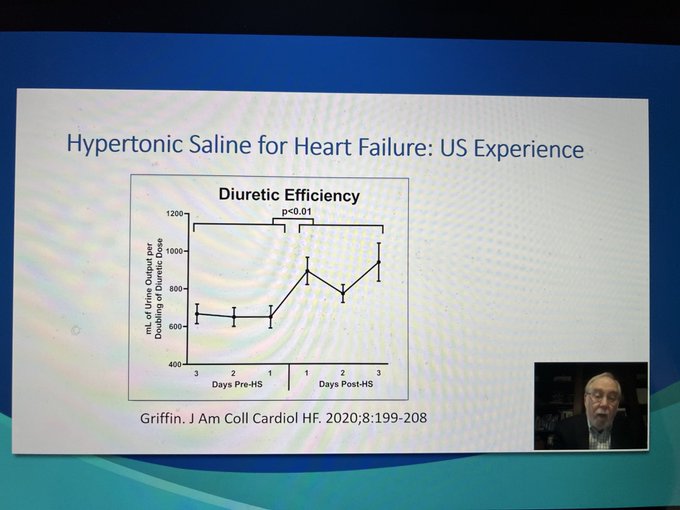
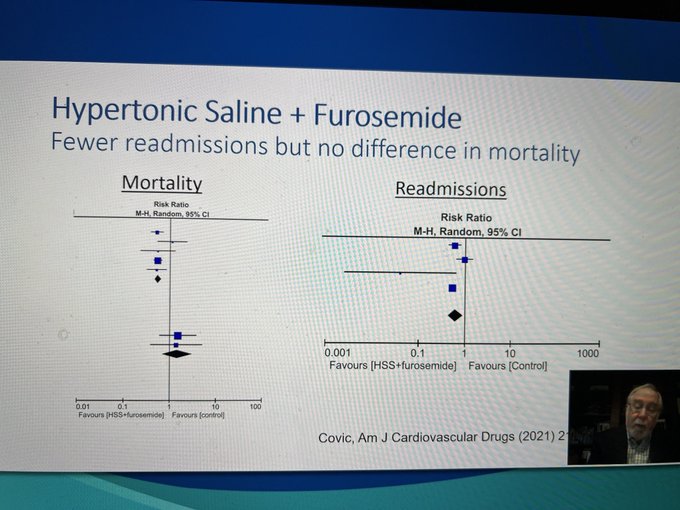
Hypertonic saline and furosemide seem to be an effective therapy for hyponatremia in diuretic resistance heart failure - Richard Sterns
#KidneyWk
@ASNKidney
3
9
82
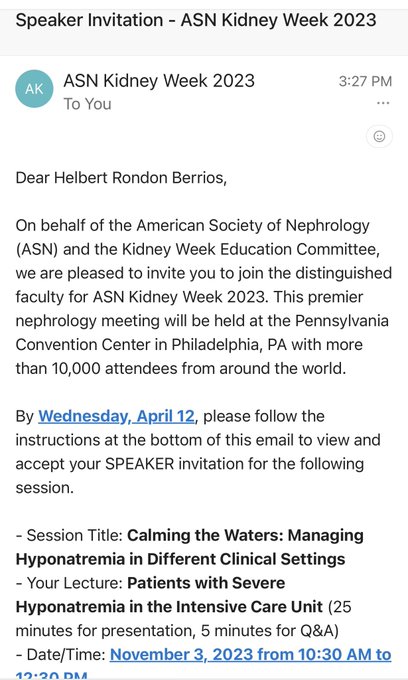
Our review on “Diagnostic and Therapeutic Strategies to Severe Hyponatremia in the Intensive Care Unit” is now available online at the Journal of Intensive Care Medicine
#hyponatremia

3
25
87
Starting my vacation to
@peru
🇵🇪to visit
#machupicchu
. Packing the obligatory reading materials for the flight.
11
9
76
Oral Urea Supplementation in the Treatment of Acute Hyponatremia among Hospitalized Adults: A Systematic Review - PubMed

4
21
75
Serum sodium (SNa) rapid correction (even when adjusted for glucose) in hypertonic states such as DKA or NKHS is not an issue. In this setting, Plasma tonicity (PTon) goes from high to low, not the opposite, as is the case in rapid correction of hypotonic hyponatremia.
4
8
76
Rate of Correction and All-Cause Mortality in Patients With Severe Hypernatremia | Nephrology | JAMA Network Open | JAMA Network

2
23
78
Effect of Protein Supplementation on Plasma Sodium Levels in the Syndrome of Inappropriate Antidiuresis - a Monocentric Open-Label Proof-of-Concept Study - the TREASURE Study | European Journal of Endocrinology | Oxford Academic

3
22
74
Approach to the Patient: Hyponatremia and the Syndrome of Inappropriate Antidiuresis (SIAD) | The Journal of Clinical Endocrinology & Metabolism | Oxford Academic
1
27
72
Furosemide works essentially as a “vasopressin antagonist” - Richard Sterns
#KidneyWk
@ASNKidney
1
22
70
Our latest review of "Hyponatremia in the Cancer Patient" published in the October issue of
@Kidney_Int
@bdubNephro
@kdjhaveri

2
25
67
Treating SIADH with only salt tabs 2 g/day

4
15
69
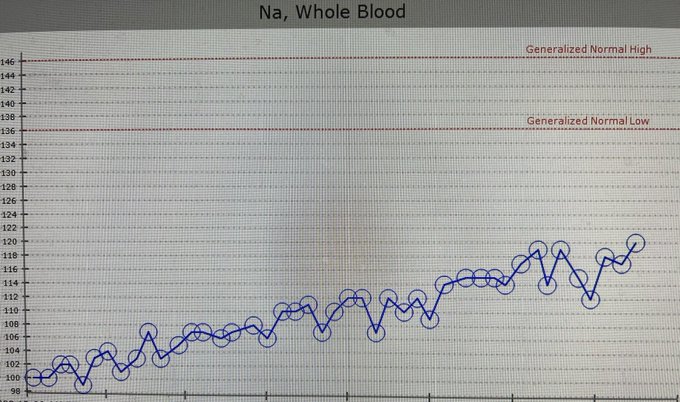
The Proactive approach does not disappoint when managing 2-digit hyponatremia
4
8
68
Urea for the Syndrome of Inappropriate Secretion of Antidiuretic Hormone

2
25
69
1/All the formulas that predict serum sodium (SNa) changes are simply mathematical manipulations of the Edelman equation. Let’s derive the Adrogue-Madias formula
3
16
65
Our recent review on “Hypomagnesemia in the cancer patient” just published in
@ASNKidney360
@bdubNephro
@kdjhaveri

This Review Article by Biruh T. Workeneh, Nupur N. Uppal,
@kdjhaveri
and
@NephroMD
summarizes magnesium physiology and highlights the mechanisms underlying magnesium disturbances due to cancer and cancer treatment.
@MDAndersonNews
@HofNorthwellDOM
@UPMC
0
30
81
2
19
67
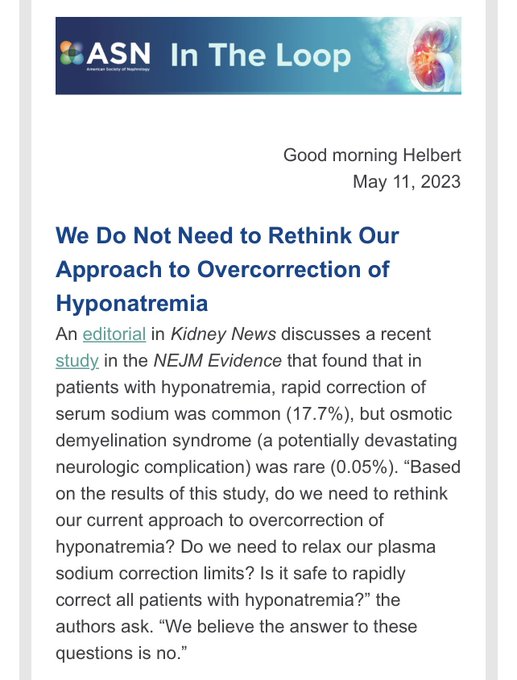
3/That is why Rick Sterns and I decided to write an editorial about this paper for
@KidneyNews


1
9
64
@Maximal_Change
@EM_RESUS
Yes! One of the common mistakes of management of hyperkalemia is that providers give 1 amp of calcium gluconate and then they forget about the wide QRS. You have to keep giving calcium every 5 min with until QRS narrows.
1
15
61
14/We developed a therapeutic approach to SIADH with fluid restriction and urea using these parameters:
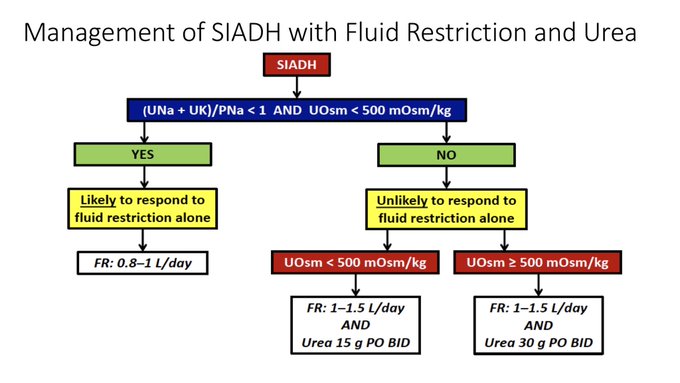
2
22
65
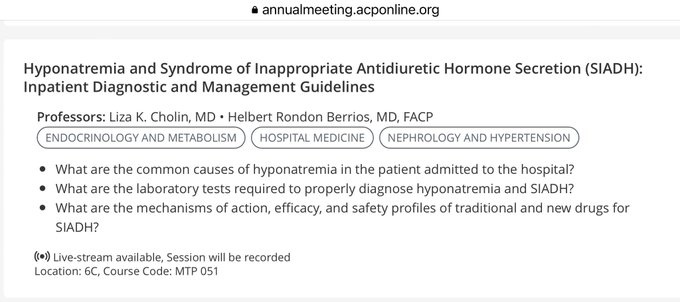
Honored to be invited to speak on
#hyponatremia
and SIAD at the 2023 American College of Physicians
@ACPinternists
national meeting in San Diego in April.
#ACP2023
3
3
66
A nice review on the Pathophysiology of Metabolic Alkalosis
0
20
61
I thought I heard them all but I was just asked to dialyze an ESRD pt (with no indication for it) after cerebral angiogram to “prevent contrast encephalopathy”
8
6
61
Osmotic Demyelination Syndrome in Patients Hospitalized with Hyponatremia | NEJM Evidence

3
18
62
Use of hypertonic saline 3% via peripheral IV approved by hospital P&T committee. Checked ✔️
3
7
59
@ganti_anita
@PittGIM
@CaseyMcQuadeMD
@mgsimonson1
This is actually my slide and I use it to show that this algorithm is awful and should not be used
9
0
62
Second video of the
#ElectrolyteClub
series on
#hyponatremia
. Lecture
#2
: Basic Physiology of Water/Plasma Tonicity Homeostasis.

4
24
56
"The mediocre teacher tells. The good teacher explains. The superior teacher demonstrates. The great teacher inspires."- William Arthur Ward
1
20
57
Thanks to
@ASNKidney
and the
#KidneyWk
program committee for the invitation to speak on
#hyponatremia
in Philly this November. Looking forward to the discussion and another fantastic meeting.
4
0
60
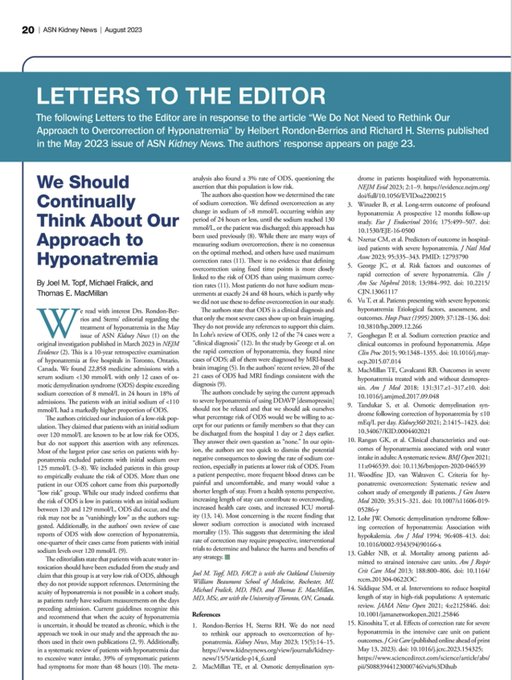
Two letters (and our response) about our
@KidneyNews
May issue commentary on the controversial study regarding ODS in
#hyponatremia
are now available online.


1
23
61
Out paper of “Hyponatremia in the cancer patient” with
@bdubNephro
and
@kdjhaveri
is now available online
3
9
57
Why are you admitting patients with plasma sodium of 113 mEq/L to the regular floor rather than to the ICU?


2
10
55
Clinical efficacy of urea treatment in syndrome of inappropriate antidiuretic hormone secretion | Scientific Reports

3
14
58
Nice review on the fictitious CSW.
1
12
55
Our review in collaboration with Richard Sterns titled "Hypertonic Saline for Hyponatremia: Meeting Goals and Avoiding Harm" is now available
@AJKDonline
#hyponatremia
4
24
56
A good and succinct review on
#hyponatremia
in the last issue of NephSAP on Electrolytes and Acid Base Disorders However, sad to see they are still recommending the classic diagnostic algorithm using volume assessment
3
10
55
Happy New Year 2019 to all except those who title their hyponatremia and hypernatremia lectures as “sodium disorders”
1
9
55
@kidney_boy
Ha! the problem is that Google university medical school is not graduating enough doctors to combat this epidemic
0
5
41
Congratulations to our 2021 graduating class of renal fellows!

2
1
52

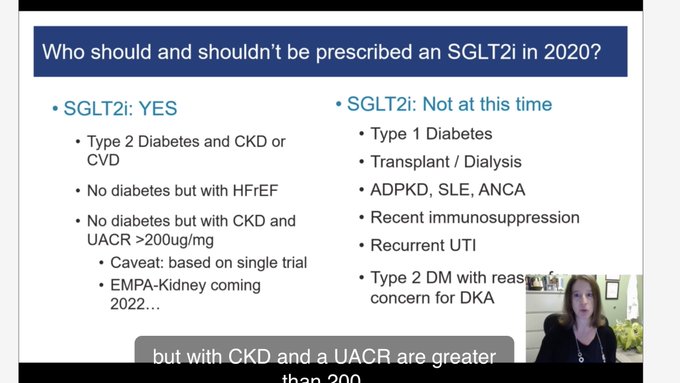
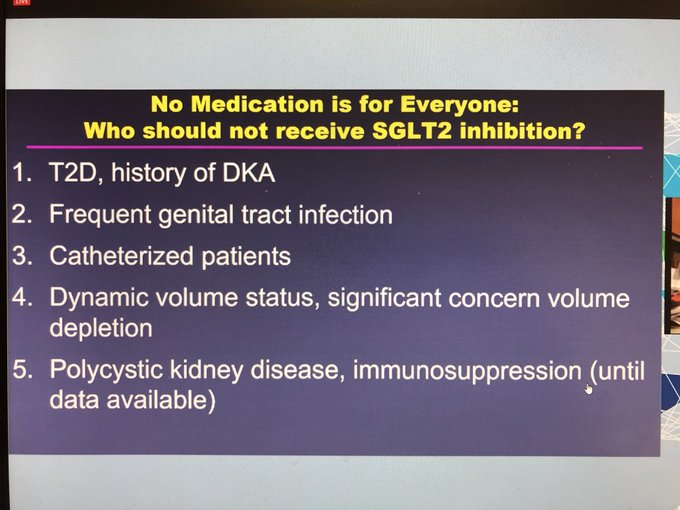
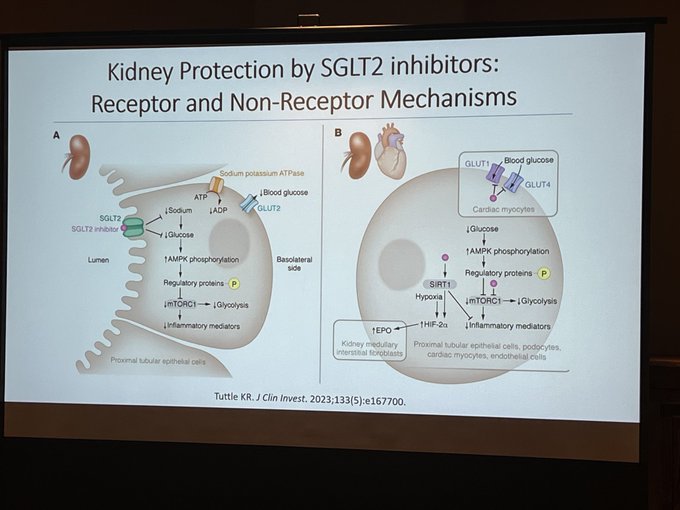
A Profile of SGLT-2 inhibitors in Hyponatremia: The Evidence to Date - ScienceDirect
1
23
53
Our manuscript on "Serum Sodium Trajectory during AKI and Mortality Risk" in collaboration with
@JonathanNefro
@kianoushbk
and other colleagues is now available online
@JournalofNeph
4
12
51
Pre-conference course on Fluid, Electrolytes and Acid-Base disorders completed - Faculty: Biff Palmer Susie Hu
@NephRodby
#NKFClinicals

2
4
52
Lecture
#5
of the
#ElectrolyteClub
series on
#hyponatremia
: "Pathophysiology and Etiology of Hypotonic Hyponatremia - Part 3"

0
11
50
I was reading the review by Bartter and Schwartz from 1967 () where they described their original diagnostic criteria for SIADH and found this interesting paragraph:
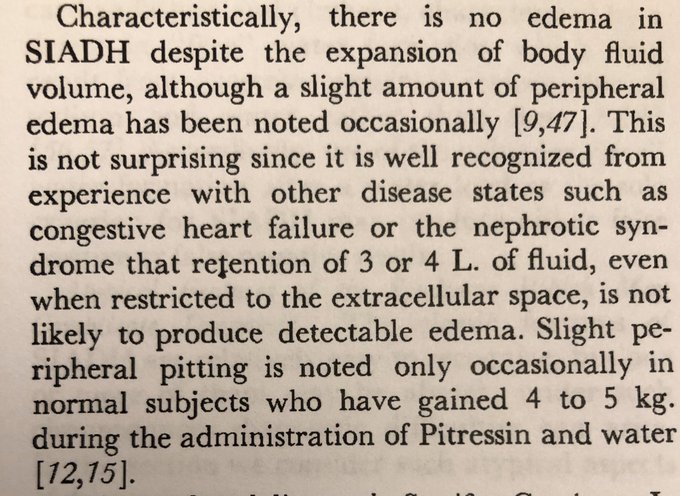
3
12
49