
John Cramer, MD
@Jdcramer
Followers
270
Following
254
Media
6
Statuses
233
Assistant Professor at Wayne State University. Head & Neck Oncologic Surgeon. Health services, quality improvement & outcomes researcher. All opinions my own.
Detroit, MI
Joined June 2009
New AJCC9V staging for HPV+ OPC refines nodal classification by incorporating ENE. Modest improvement—but we still face a disconnect between pathologic and clinical staging systems. #HNSCC #HPV #AJCC.
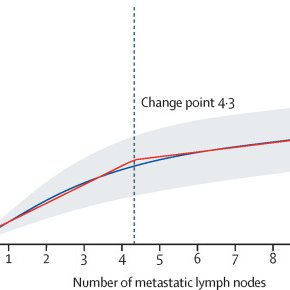
thelancet.com
The AJCC9V HPV-positive oropharyngeal carcinoma staging classification confers an improved schema for guiding prognostication and management compared to AJCC8E. Incorporating ENE and correcting...
1
0
1
RT @AAOHNS: In our latest Voices of #Otolaryngology episode, Amanda Dilger, MD, and Neelima Tummala, MD, share game-changing sustainability….
0
1
0
RT @rbryanbell: Boom!💥 @FDA approves neoadjuvant and adjuvant pembrolizumab for resectable locally advanced head and neck squamous cell c….

fda.gov
On June 12, 2025, the Food and Drug Administration approved pembrolizumab (Keytruda, Merck) for adults with resectable locally advanced head and neck squamous c
0
21
0

What changed in E3311 long-term data?. ✔️Transoral surgery + 50 Gy = durable control in intermediate-risk HPV+ OPC. ✔️No OS or PFS difference by smoking or subsite.⚠️Observation alone in N1? Late recurrences → risky. 🔑Pathologic risk-based adjuvant therapy works.
3
3
5
RT @rbryanbell: Great to be @ASCO for yet another plenary session featuring HNSCC. NIVOPOSTOP is POSITIVE! Exciting advance & option for hi….
0
1
0
RT @AHNSinfo: This #WorldNoTobaccoDay, learn how quitting can lower your risk of cancer in the mouth, throat & voice box: .
0
12
0
RT @DrMLChua: Very powerful and insightful discussion by Prof Kevin Harrington @royalmarsden on KN-630 and C-POST. The slides speak volumes….
0
11
0
Adjuvant cemiplimab improves DFS in high-risk cSCC (HR 0.32). Among the strongest DFS signals I've seen. Starting ICI after RT may be key—avoids immune suppression. OS flat, likely due to high crossover. 🔗
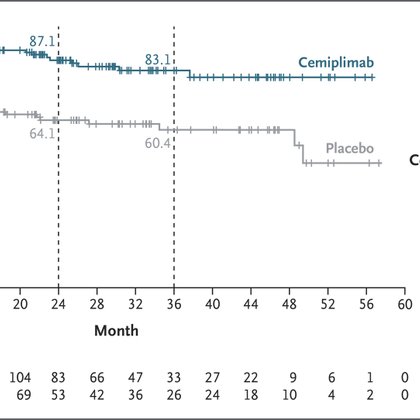
nejm.org
Patients who have cutaneous squamous-cell carcinoma with high-risk features are at risk for recurrence after definitive local therapy. The benefit of systemic adjuvant therapy options has not been ...
0
0
1
RT @CJTsaiMDPhD: #ASCO25 KEYNOTE-630. 📒Adjuvant pembro after surgery and PORT for up to 9 cycles in high-risk locally advanced cutaneous sq….
0
11
0
RT @CJTsaiMDPhD: On the contrary, adjuvant cemiplimab improved DFS in a similar population of cSCC after surgery and PORT. @DrNeilGross @M….
0
4
0
RT @VSandulache2025: Proposal: for new oncology drugs or regimens for which clinical trial data conflict or are limited the FDA should offe….
0
2
0
RT @PBlanchardMD: SBRT (6*6Gy) is a new treatment option for small oral cavity cancers (T1-2) at risk of local recurrence after resection (….
0
56
0
4/ Surgical pathways + perioperative ICI seem to better leverage immune recovery.• Tumor debulking.• Less treatment-induced immunosuppression.• A window to target micrometastatic disease.Timing is critical — surgery plus ICI may be the winning sequence.
0
0
1
3/ Similar patterns across cancers:. ✅NSCLC: CheckMate-816 (neoadj nivolumab + surgery) → EFS benefit. ✅Esophageal: CheckMate-577 (adjuv nivolumab after surgery) → DFS improvement. 🚫CRT + ICI (lung, bladder, esophageal) → mostly disappointing.
1
0
0
2/ Surgical pathways remove the bulk tumor and much of the immunosuppressive microenvironment. In contrast, concurrent CRT + ICI is less effective: CRT causes lymphopenia and T-cell dysfunction.
1
0
0