
Tom
@sleepy__doc
Followers
1,657
Following
161
Media
44
Statuses
265
Professional account. Geriatrician with an interest in delirium, OncoGeris, MedEd, LGBT health and sauvignon blanc. Kindness is our biggest strength.
London, England
Joined December 2020
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
Cohen
• 182726 Tweets
$GME
• 118464 Tweets
MY LOVE IS LIKE
• 61352 Tweets
Aziz Yıldırım
• 55815 Tweets
GameStop
• 55023 Tweets
Ali Koç
• 44458 Tweets
Roaring Kitty
• 33719 Tweets
Vance
• 30845 Tweets
gracie
• 30676 Tweets
Square Enix
• 24299 Tweets
Atiku
• 23086 Tweets
$AMC
• 20585 Tweets
Ravens
• 19914 Tweets
सुशील मोदी
• 19234 Tweets
TREASURE IS COMING
• 15223 Tweets
Tuberville
• 15071 Tweets
Tyson
• 14801 Tweets
McDavid
• 14755 Tweets
Carlos Vives
• 13859 Tweets
DIAMOND HANDS
• 12903 Tweets
Vitor Roque
• 11907 Tweets
GPT-4o
• 10514 Tweets


















Pinned Tweet

As a northerner in a southern hospital I had absolutely no idea when to prescribe this medication
66
47
2K
Last night I admitted a patient with SVT (rate 150) and when the nurses did his covid swab he cardioverted 😭😭😭
308
687
11K
Sometimes the worst part of being a dr is that no matter how stressed/close to tears/overworked you feel, you still need to display the happy-to-help joviality of a frankie and benny’s waitress. What an effort
35
50
892
This is for a mandatory exam we have to self fund that is an MCQ and I assume therefore computer marked. It’s daylight robbery tbh.

34
72
764
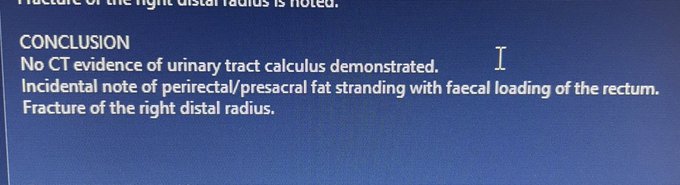
We moan about the NHS but I sent a patient for a CT KUB today and the only positive finding on the scan was (accurately) a fractured right distal radius
23
12
569
@Mybrainisbrian
He had an incredibly fast heart rate due to an underlying arrhythmia and when the nurse did the swab, he converted out of the arrhythmia to a normal heart rate (have a look at valsalva manoeuvres)
10
11
397
“…and we used to have prescribe all their doses for the weekend and chase an INR on the Sunday if we were the F1 on call and write their discharge doses in a little yellow book and we’d never even heard of a NOAC!’

10
23
374
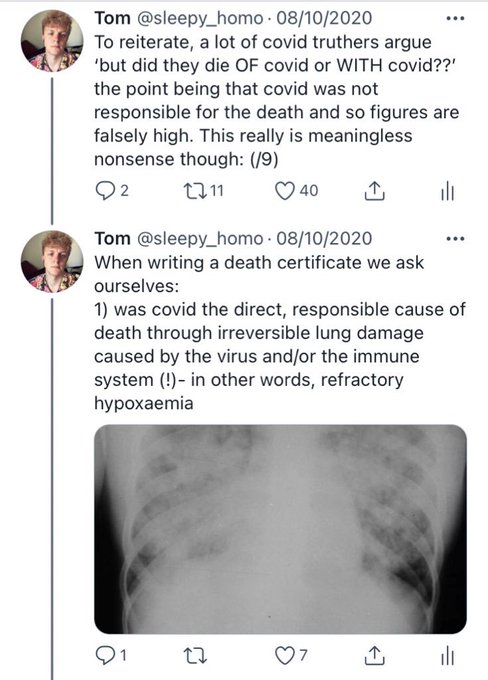
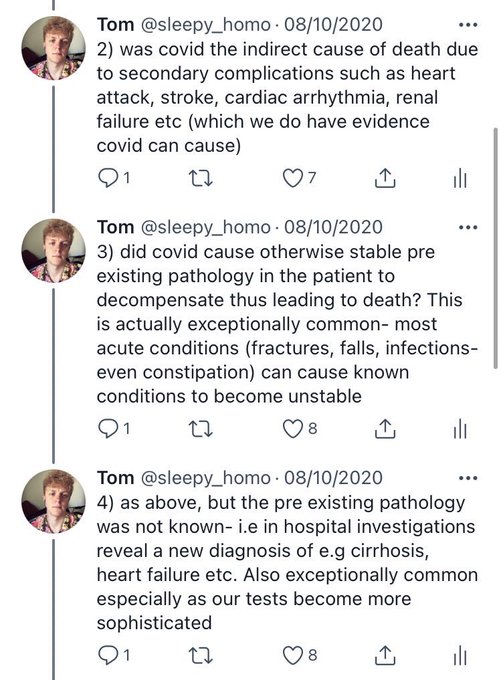
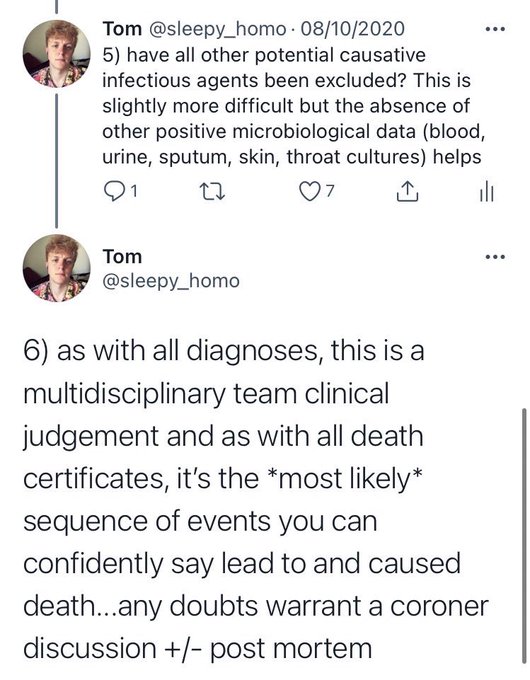
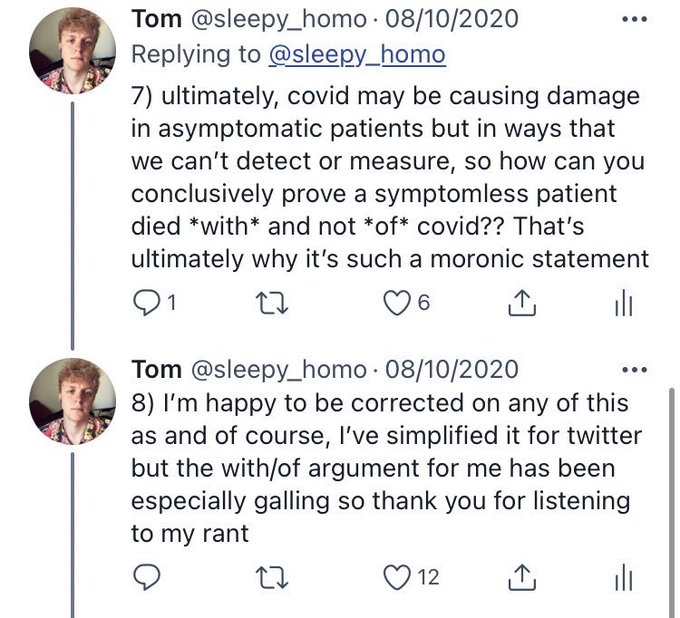
If anyone is finding themselves frustrated by ‘but did they die WITH or OF covid????’ feel free to use this argument I’ve constructed here
7
69
308
Love being a doctor, it’s what I’ve always wanted to do but honestly working for the NHS you’ve gotta ask yourself…at what cost
16
18
284
Thinking about the time some jnr drs presented an audit at grand round on successfully improving inhaler use in IPs and at the end a consultant put his hand up to tell them he’d calculated their results weren’t statistically significant
16
3
276
@Beska
See also:
- no thanks for the 99 times I do discuss escalation at 4am
- ‘disappointing’ is such a profoundly shitty verdict
- diagnostic uncertainty in view of frailty syndrome presentation and sensory/cognitive impairment
I could go on 😤
3
0
192
Watching an obstetrician operate during an emergency is insane, their concentration is unmatched. You could walk into theatre on an elephant and they wouldn’t notice
10
3
184
Imagine being given 4 months to complete a complex, mandatory tick box exercise, someone suggests presenting it at GR for an extra point at interview and some professor elects to humiliate you in front of your entire cohort of colleagues. I’d be raging
0
1
153
Lol I did a 13 hour med reg night shift at £60/h as an emergency to help a friend and after tax, NI and student loan I managed to earn £374.70 what a joke
11
6
106
@BitBullish
Their heart didn’t stop, it just stopped beating in that very rapid rhythm meaning we didn’t have to give any medication 😊
0
1
91

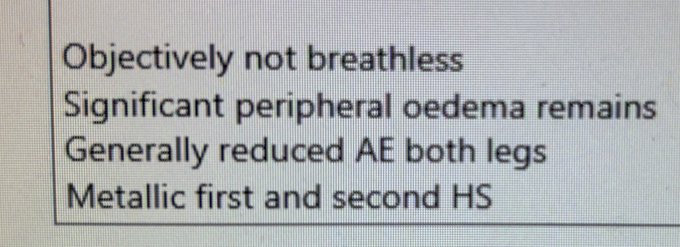
Do you ever read your own notes and wonder what the hell you were thinking?? Apparently this patient’s legs weren’t breathing well
10
3
84
@gfreeman2012
Reverted from a very rapid heart rhythm due to an underlying rhythm disorder, to a ‘normal’ heart rhythm, which is a process that usually requires medications
5
2
61
I’d be interested to know if you think a dangly earring is appropriate to wear to work as a doctor?

77
3
59
@ollieburtonmed
Why? It’s humiliating and patronising. Appreciate you weren’t there to witness it but it was so needless
1
0
53
I feel like the most consistent theme of my medical career is elderly ladies asking me where I got my perm 😭😭😭
6
0
50
In hindsight, expecting F1s to be in charge of list management, having to come to the wars early to ensure it’s updated and accurate, is/was insane
10
0
49
I’m using MRCP pt 2 questions to revise atm bc the Geriatrics SCE exam contains quite a bit of gen med (and bc why not) and I can’t believe this shit is still flying around
17
2
49
Passed it though 😎
This is for a mandatory exam we have to self fund that is an MCQ and I assume therefore computer marked. It’s daylight robbery tbh.
34
72
764
4
0
48
@czbikerchick
Yes! From the rapid and potentially life threatening SVT, back to a normal, safer, slower heart rate
3
0
39
Don’t get me wrong the money is nice but is it really worth the stress of being the senior medic on site, the sleep disturbance, the effects on my health, the lack of sunlight??
1
0
40
Friends and families of my patients.
I know you’re angry
I know you feel let down
I know you’re making sacrifices
But NHS staff can’t be the emotional punching bags for these frustrations.
I have no control over vaccines, lockdowns or restrictions.
And I’m trying my best.
1
7
39
Just to clarify I was in the theatre for less than 30s bang in the middle of a MOH and crash CS. I’m a med reg. Let’s not over complicate this. It was a brief observation of a clinical situation that I’m not used to. We don’t need your feedback
0
0
37
@Faezalamodi
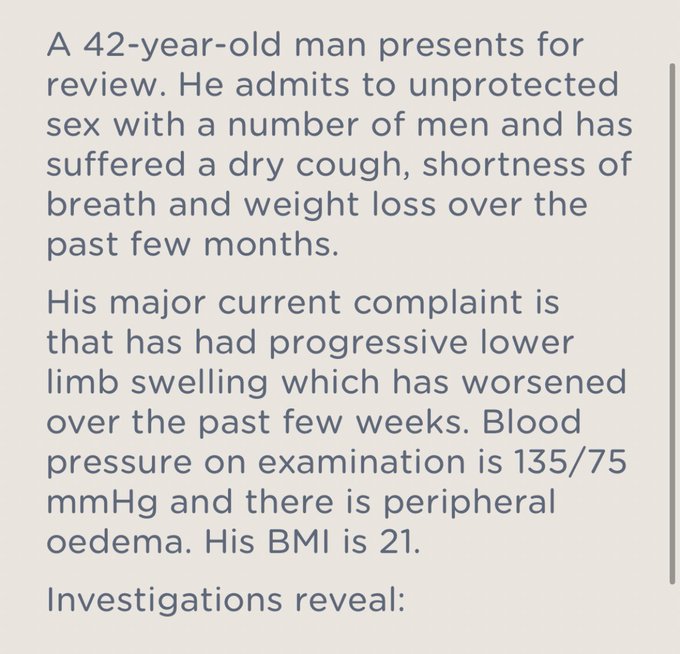
Actually for me, why can’t the vignette be ‘a 42 yo man who was recently diagnosed as HIV +ve…’ bc then a) we’re not making diagnostic assumptions based only on demographics which can reinforce biases and narrow clinical judgement but also b) it’s irrelevant detail
4
0
28

My death certificate will only say one thing and it’ll be 1a) acid reflux
1
4
27
Teaching at med school: this is how this works
Teaching after med school: this is not, in fact, how anything works and everything you know is wrong
3
2
23
Hard pill- the pandemic has made some drs difficult to work with, because they are absolutely, unequivocally burnt out but we don’t create a culture where this can be a) admitted or b) managed so instead of having time off they soldier on, becoming increasingly irritable and rude
2
3
21
Can we call neuro to see if they want the mri. Ok can we call radiology to vet the mri. Ok can we call the coordinator to book the mri. Ok can we call the radiographers to do the mri. Ok can we call the family to consent for the mri. Ok the mri is broken. Ok can we call neuro to
1
1
20
I see it’s that time of the year where we have to do reams and reams of frustrating paperwork in our own personal time for the next rotating hospital bc HR departments have an inexplicable ability to communicate or create a centralised database
2
3
19
Completely unexplained insomnia last night. Woke up at 00.30 after 1h sleep, then was awake until about 6. Alarm goes off at 6.40. I’ve taken the day off work for obvious reasons but I feel completely fraudulent. I’ll be back tomorrow but insomnia truly is hell
7
0
19
I’m on wk 3 at my new trust and my 1hr 20min commute for an 8.30 start is absolutely killing me. I’m not a morning person anyway but I’m constantly knackered, not what I need for the 9h shifts. Not sure I can do this for 12 months. Genuinely don’t know what to do ☹️
7
0
19
@_B_e_t_h_B_
@darylthedevine
I’ve been a waiter in a high end pub and it was sometimes *worse* than being a dr because it’s as phys/mentally exhausting but has an unfavourable power balance (customer is always right) which is why I reject the ‘unskilled work’ rhetoric re. minimum wages
2
0
17
Todays NHS bullshit is sponsored by My patient wasn’t discharged because in the notes we wrote ‘recovered from sepsis, home today’ instead of ‘MFFD’.
3
0
16
I really hate the new Geris specialty CiPs. Two of them aren’t even pure Geris (Stroke and Movement Disorders), one isn’t hospital based and one is continence. What happened to frailty? Memory disorders? Palliative care and ACP?
4
0
15
Doing QIPs doesn’t make me a better doctor, it makes me a compliant trainee
0
0
15
Who bleeps for advice at 12.30 honestly I’m elbow deep in the salad bar and waiting for my costa soy latte
0
0
15
It’s happening all over again.
“Previously f+w…loss of taste with cough…RR 35 and HR 125…bilateral infiltrates with lymphopaenia…pO2 5.2 on NRB…”
I’m tired.
0
0
14
>90 yo patient a/w fits. CT head- 3 metastatic lesions. PMH: Mod-Sev dementia, CFS 6, not suitable for SACT, for BSC. O/e massive, tender hepatomegaly, CXR nil obvious. Qu: do you perform CT CAP before d/c to NH with Comm Pall Care?
5
4
13
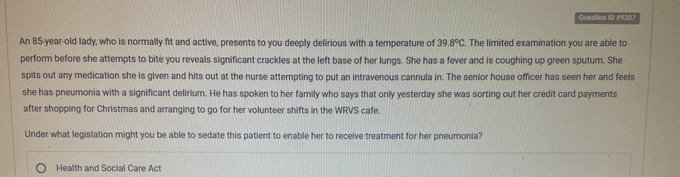
I love when the consultants who write exam questions produce a full Enid Blyton style autobiography for their imaginary patients like I need to know where this lady was doing her Xmas shopping. Was it John Lewis? Was it TK Maxx?? We’ll never know
2
1
13
I have a feeling a lot more hospitals are actually in a severe crisis but feel it’s easier to let healthcare professionals continue to struggle than it is to publicly admit it
0
0
13
Today’s other frustration is why are we calling a nonagenarian being admitted with suicidality during a period of bereavement a ‘social admission’
0
0
13
“Patient is full recovered from the acute illness and is clinically appropriate for discharge home with no further medical or therapy input required”
“OK but we need you to write MO or she can’t go”
1
0
12
I really feel like if an older person falls, but it’s due to acute pathology like heart failure or sepsis we should instead call it ‘collapse’ to avoid tick box medicine. Why are you doing a 24h tape on a 90 year old with Klebsiella bacteraemia???
2
1
11
One of my old consultants shares a name with a historian who writes books about the sex lives of peasants (I’m not joking) and they’ve used my consultant’s photo in an online review of one of her books, instead of the author’s 💀💀💀
0
0
12
People who get mad at healthcare professionals who don’t take food/leftovers to work as a cost saving idea sometimes underestimate both the lack of, and restrictions on, food storage and heating in NHS wards. Also the microwaves are always filthy
0
1
11
Discovering one of the ear pieces on my stethoscope is broken might explain why everyone I’ve examined for the last two weeks has had ‘reduced air entry throughout both lung fields’
0
0
10
Why is there such a reluctance to use Diltiazem or Verapamil for control of AFRVR? Treatment seems to be either BB or Dig, such that we almost seem to become deskilled at using CCBs acutely
8
2
11
Are your sickle cell patients crying in pain because they’re drug seeking or have you assumed they’re drug seeking so they’re now crying in pain?
0
0
11
This is apparently how long I’ve been timing a patient’s respiratory rate at work

1
0
11

I’ve had a tax rebate almost every year of being of a dr and I think it’s because when I was an F3, my new hospital thought I was a locum ophthalmology consultant
1
0
9
@LouiseHogh
@sleepy_doc
Kingston is still at the top of my list for me to come be a consultant at so as long as the pigeons have moved on I’ll be applying!
0
0
10
@DrKidneyAsh
Agreed, the temptation to just see them is pretty strong but it’s never safe especially if you’re the take reg
1
0
10
Nothing is gonna get my med reg blood boiling more than someone referring 3 patients at the same time at 7.15am
0
0
10
Why are there always national shortages of medications?? IV Paracetamol, Salbutamol, Bumetanide…is it the B word 😬
2
2
10

Broadly speaking a good dr is:
☑️ clinically proficient
☑️ kind and compassionate to patients
☑️ kind and compassionate to (all) colleagues
I will not think highly of you until you’re all three, no matter how many letters follow your name
0
0
9
Is there anything more stressful than receiving a new rota? On call on induction week, working Xmas *and* NY once again, on call during weddings, planned visits home, an hour commute for an 8.30 start/17.30 finish…
0
0
9
I’ve injured my foot recently but it seems to be getting better so today I’m going to try TWOC (trial without crutch)
2
0
8
@DrHelenOram
It’s from the Pastest MRCP part 2 question bank, I downloaded the app yesterday and was one of the first questions to come up! But I passed part 2 in 2015/6 and I remember similar questions appearing then
1
1
7
Today will be the 5th Take shift I’ve done in the last 7 days because of a rather short sighted swap. 65 hours of answering bleeps

0
1
8
My next hospital is my last training hospital and until I find out where that is I feel like planning my life for the next 12-18 months is on hold
0
0
8
Delirium can be so strangely diagnoses. You can have a patient in MOF 2nd to severe sepsis and it’s delirium ?cause but someone else has 1+ of leucs and all of a sudden it’s 2nd to UTI? It’s strange how these (questionable) associations stick
1
0
8
@wparrysmith
Just to clarify I was in the theatre for less than 30s bang in the middle of a MOH and crash CS. I’m a med reg. Let’s not over complicate this. It was a brief observation of a clinical situation that I’m not used to.
2
0
8
I was at a seminar on Thursday and a female Geris Cons asked a qu about frailty and the speaker said ‘perhaps you could tell us what frailty is first?’ and an unknown man in the audience interrupted, told a story about frailty and didn’t even answer the question
0
0
8

Seeing many pts whose NOK report declining cognition coinciding with lockdown starting; perhaps subclinical cognitive impairment now becoming apparent due to loss of social support, exacerbated by loneliness and temporal disorientation?
3
2
7
I finished nights on Friday and yet today bc of sleep patterns I’ve been up since 3.30. Insane how, were it not for annual leave id be back at work today, expected to do my usual clinical duties
0
0
7
When it’s “We’d like you to kindly review this patient” and they’ve already been in hospital for 67 days

0
0
7
Getting apologies from ED drs who believe their referrals for elderly patients are ‘bad’. But any acute condition can exacerbate frailty- it doesn’t have to be overwhelming illness. If it’s safer to admit for therapy and symptom control then surely that’s a very *good* referral?
1
0
7
Naming wards after fun things always sounds like a good idea until you’re ringing the cardiology reg in a medical emergency like ‘Hi, is this Hotdog A? I’m ringing from Jane Austen B about a patient on the Microwave Unit’
0
0
7
At
#Dementias2024
National Conference today, will attempt to tweet some things of interest. Currently hearing about new potential pharmacological therapies in the research pipeline for treatment of Alzheimer’s dementia (thought to be ~28!)
0
1
6

