
Sara Jane Cromer
@sjcromermd
Followers
84
Following
239
Media
2
Statuses
77
Endocrinologist working to achieve equitable healthcare for people with type 2 diabetes
Joined October 2020
#ADA2024 excellent session on the future of GWAS for diabetes! Amazing work by @miriam_udler is so popular that she needs two microphones!
0
0
7
While we work to overcome barriers to trial enrollment for Black, Hispanic, and Other race or ethnicity individuals, we must also work to ensure they receive equitable care within trials - examining our own biases and working to overcome the ongoing effects of structural racism.
0
0
1
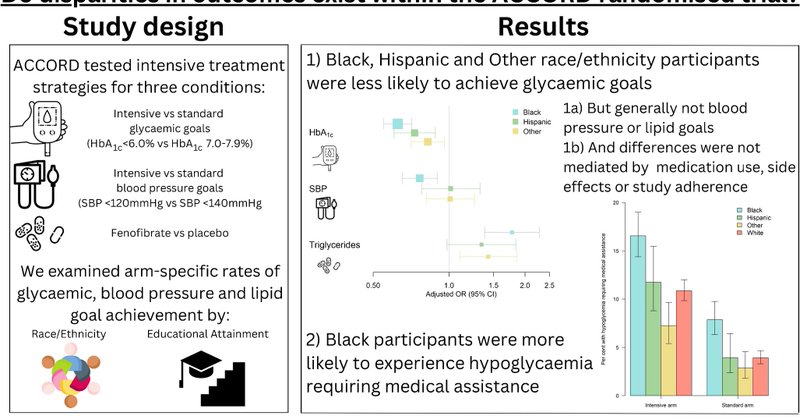
Altogether, we learned: 1. Disparities in treatment goal achievement exist even within RCTs, more so with more intensive interventions. 2. These may be partially mediated by implicit bias or other factors contributing to different implementation of trial protocols.
1
0
1
However, insulin dose and # of oral meds each partially mediated (10-20%) the association between race and glycemic goal achievement. As glycemic targets and frequency of monitoring/intensification of therapy were protocolized, this was a bit of a surprise.
1
0
0
Although there were differences in side effects, particularly higher hypoglycemia risk for Black participants in both arms, these mediated <5% of the differences in glycemic goal achievement. Visit attendance also mediated <5%.
1
0
0
To understand disparities in glycemic goal achievement, we looked for mediation by medication use (insulin dose, oral med use), side effects (hypoglycemia, weight gain), and adherence (visits attended).
1
0
0
Interestingly, disparities in treatment goal achievement were smaller, null, or even reversed for the less intensive blood pressure and lipid subtrials, suggesting disparities were greatest with more intensive, high-burden interventions (e.g., self-titration of insulin).
1
0
0
We found racial and ethnic difference in treatment goal achievement, despite the many resources provided by the trial. Specifically, Black, Hispanic, and Other race or ethnicity participants were less likely to achieve glycemic goals, regardless of treatment arm.
1
0
0
ACCORD enrolled people with T2D and randomly assigned them to intensive (A1c <6%) or standard (A1c 7-8%) glycemic control targets, allowing investigators to use any treatment to achieve those goals. Subtrials studied intensive systolic BP targets and fibrates, as well.
1
0
0
Within the supportive context of a clinical trial (incl. regular access to healthcare, health education, free meds), you might expect health disparities to resolve...right? Read on to see what @tthaweethai @DeborahWexler and I found in ACCORD. https://t.co/Tvhpcccv9p
link.springer.com
Diabetologia - Clinical trial participation should theoretically reduce barriers to care by ensuring medication and healthcare access. We aimed to evaluate disparities in achieving diabetes...
1
2
7
Grateful to be a part of this fantastic team of people raising awareness about disparities in bone health. Article is open access through mid-august!
0
2
6
A succinct and informative reminder that men and women have different risk factors, presentations, and experience of diabetes!

Sex and gender matter! This review highlights sex- and gender-specific clinical features of type 2 diabetes, and differences in risk factors, screening, diagnosis, complications and treatment between women and men with #T2D
https://t.co/GQwZugqA39 🔓
0
0
0
Many congratulations to Dr. Enrique Caballero-Robles - a wonderful teacher, mentor, collaborator, and patient advocate!
0
0
2
Full text here: https://t.co/bCWxQ4LLNL and many, many thanks to @miriam_udler @BurnettBowie @josep_mercader @AlisaManningPhD @cmlakhan @chiragjp @JBCole150 @Riudecanyenc and the many others who contributed to this work!
diabetesjournals.org
OBJECTIVE. Quantify the impact of genetic and socioeconomic factors on risk of type 2 diabetes (T2D) and obesity.RESEARCH DESIGN AND METHODS. Among partici
0
1
4
Public health efforts to mitigate the impact of metabolic disease should take a whole-person approach and may have benefits for people across the genetic risk spectrum. Now let's work on policies to build health equity!
1
0
1
We found similar results in populations of European ancestry in the UK biobank, as well as populations of African (both biobanks), admixed American (predominantly self-identifying as Hispanic or Other race/ethnicity; MGBB) and Central/South Asian (UKBB) ancestry.
1
0
1
Increasing socioeconomic risk associated w/higher rates of disease regardless of baseline genetics. However, additive interactions existed whereby the absolute increase in disease prevalence with worsening socioeconomic risk was much greater among those with higher genetic risk.
1
0
0
We then examined the raw prevalence of T2D and obesity across intersecting quintiles of genetic and socioeconomic risk. Those in the highest risk quintile for both factors had almost 8x T2D prevalence and 3.5x obesity prevalence compared to those in the combined lowest quintile.
1
0
0
In adjusted models including both risk factors, 1 standard deviation increase in genetic risk was associated with approximately 80% increased odds of T2D and obesity, and 1 SD increase in socioeconomic risk with 30% increased odds, with no evidence of multiplicative interactions.
1
0
0
First, because there is no established gold standard SES measure, we examined the association of area-level education, income, and employment measures, as well as more complex SES indices, with T2D and obesity - area-level education most strongly associated with disease.
1
0
0