

Cliff Reid
@cliffreid
Followers
45K
Following
20K
Media
2K
Statuses
15K
EM/ICM/PHEM doc. LOVE learning + teaching. I work in the sky above Sydney, have the attention span of a bullet, + often have days that are like cartoons #FOAMed
https://cliffreid.substack.com
Joined March 2009
I showed a resident how to diagnose a pneumothoraces She asked 'don't you mean a pneumothorax?' I replied 'it's pleural'
197
866
9K
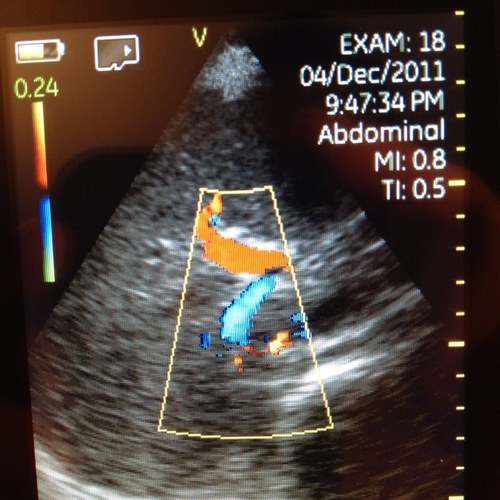
#POCUS #MedTwitter #Nephpearls Many #VExUS enthusiasts asked for a #tweetorial on image acquisition pearls. Did one b4 but time for an updated one 🧵 #1 Let's start with basics Color Doppler identifies the flow + tells the direction (blue is away & red towards the probe [BART])
34
516
1K

NEVER to sick to be retreived.. a matter of skills, experience, tools, platforms and the TEAM. #oslohems
1
3
12
A key tip in neonatal transport is to have different modalities of transport. This one with Babypod. Same level of monitoring. Faster and lighter. Les change in helicopter. A good example of retrieval method suited to the mission. #tailoredtreatment #oslohems
2
4
20

Absolutely delighted to launch @MedPodLearn. A searchable medical podcast library with educational scaffolding and tools to download all your activity. Have a look! https://t.co/1B0lvKmmAY
5
18
43

Huge #bedsidepearls on Shock via @cliffried The Art of Coupling 🧠 human ideas & 🤖 AI Big jump on knowledge dissemination
Interactive Holistic Four-Interface Shock Model based on the work of @ThinkingCC and friends thanks to @GeminiApp
https://t.co/gbhZ56T175
0
3
5

You need to echo people in thyroid storm before you beta block them or you might kill them
in thyroid storm, treating sinus tach with a beta-blocker will occasionally cause death many patients have reduced LVEF & compensatory tachycardia (borderline cardiogenic shock) beta-blockers push them over the edge what data supports B-bl in thyroid storm? why do this?
7
37
152
If you listen to podcasts then check out out my current favourite app - MedPod is a game changer in making learning stick Summarises the podcast into key concepts, pearls, pitfalls, application in practice, quiz, & reflection download for CPD! Apple: https://t.co/vcXEIvFRjR
1
12
35

Oh wow brother that’s awesome!
Interactive Holistic Four-Interface Shock Model based on the work of @ThinkingCC and friends thanks to @GeminiApp
https://t.co/gbhZ56T175
0
28
152

Come to 🌷 Amsterdam 🇳🇱 next year. 24-26 September 2026 Complex airways At Olympic Stadium Train with inspiring and skilled international airway educators Registration: https://t.co/iEOLD5imzP
@cliffreid @jducanto @AnRocad @Respitudoc @rosshofmeyr @DaveOlvera1
1
4
6
Interactive Holistic Four-Interface Shock Model based on the work of @ThinkingCC and friends thanks to @GeminiApp
https://t.co/gbhZ56T175
2
77
250

PO breaks down the haemodynamics of the arrested circulation- taking resus beyond the algorithm- PART 2 This is CPR like you’ve never heard it before @cliffreid @HawkmoonHEMS @SydneyHEMS #resus
https://t.co/zDZcq3I9qJ
https://t.co/2VZPGthmPJ
0
3
9

@loes_bruijstens @GrossiIrene @IrishEMtrainees @jducanto @cliffreid @cathaldeb @uniofgalway @ITERN_ @EMTAcommittee @Galway_CD

📢 2026 Courses are Live! 2026 Connemara Courses: 🌍 Humanitarian Medicine Course (June 12–14) EOIs: admin@galwayem.ie 🔹 Connemara Resuscitation Airway Course (Sept 3–4) EOI form: https://t.co/HiFS2LqJd0 More details & feedback: https://t.co/YIWFwqUIxY
0
2
3

@cliffreid Have you spoken to your lab? Direct selective ion measurement has been normal practice for >20 years & is how ABG machines measure it. Point is to understand the physiology treat the patient not the number
0
1
3

@cliffreid Excelent! And blood gas analizers dont suffer this artifact (direct ISE technology) so for real Na levels just check the ABG and forget the lab. For the same mechanism ICU patients with severe hypoalb could have pseudoHIPERnatremia.
0
1
8
'Pseudohyponatremia' due to hyperglycemia is REAL hyponatremia which gets better when you fix the glucose 'Pseudohyponatremia' due to elevated lipids or protein is NOT real hyponatremia. The lab tells you the sodium is low but there is no true hyponatremia I made this animated
6
27
166
Emergency Medicine Registrar teaching today: 2 hours of airway sim then 2 hrs advanced airway classroom and practical including hands on practice with airway visualisation using the aScope in our ”live cadaver lab” Like with kids - you want them to have the things you never had.
5
17
120

12
50
381

@cliffreid Best phrase I saw in BMJ this week, The fallacy of…. “Techno salvationist bullshit” @dr_mattmorgan @bmj_latest
1
6
19
1 sign that your body needs magnesium

5
206
1K