

Emir Baskovski
@baskovski
Followers
881
Following
2K
Media
103
Statuses
282
Electrophysiologist, Cardiologist @AnkaraUni
Joined June 2019
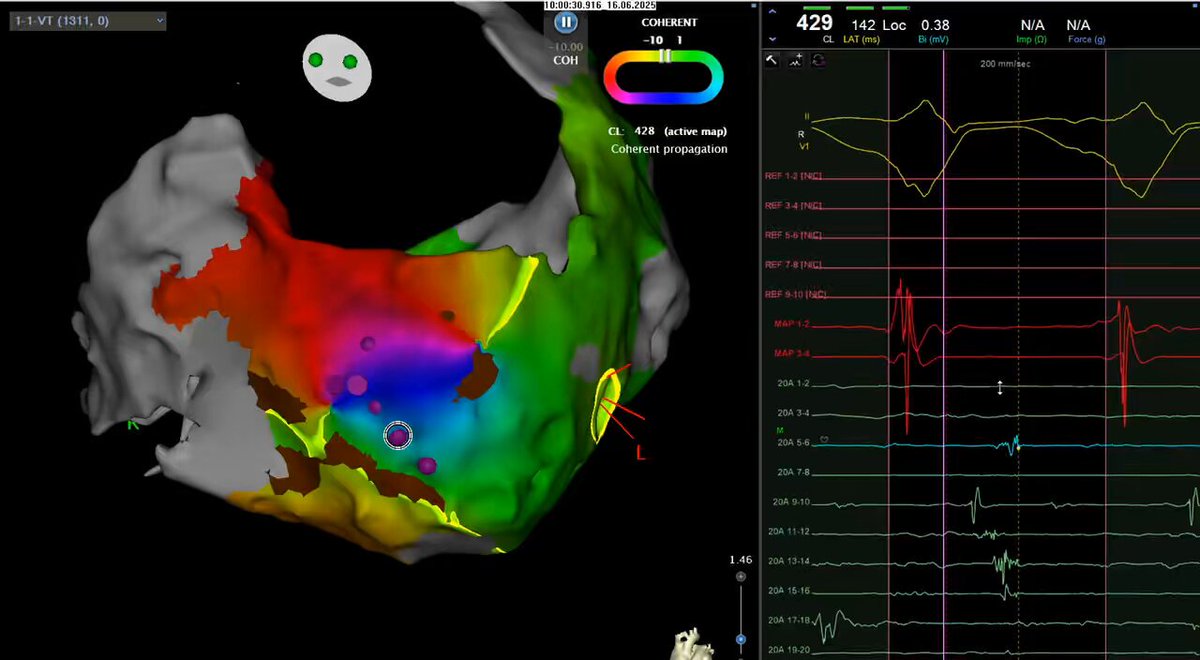
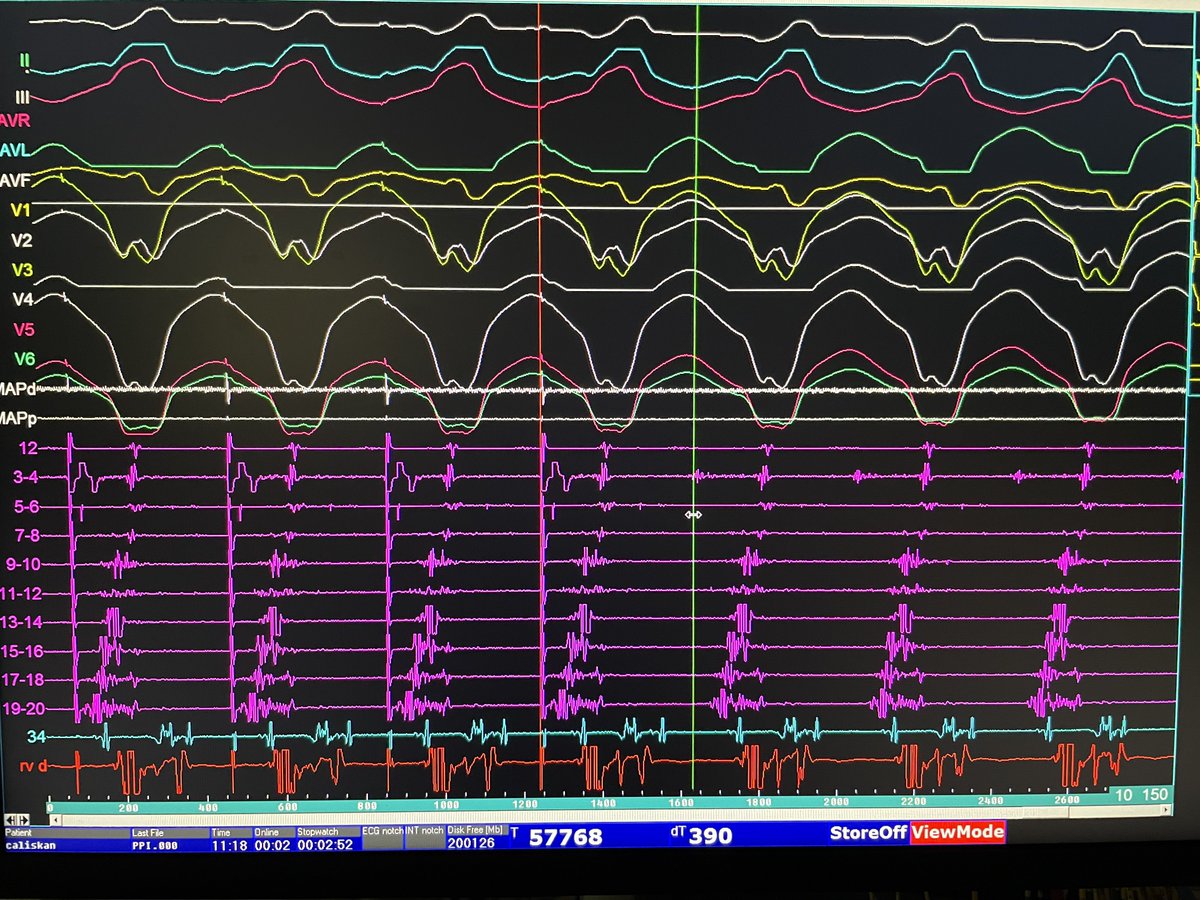
A mid-to-end diastolic EGM at distal GCV during LV summit VT in NICM.#Epeeps @timucin_alt @akyurek_omer

2
3
37
#Epeeps .Epi only mapping & #Rf in apical aneurism w endocardial thrombus precluding endo approach. #VT terminates shortly after Rf on mid isthmus. @timucin_alt @akyurek_omer
0
0
17
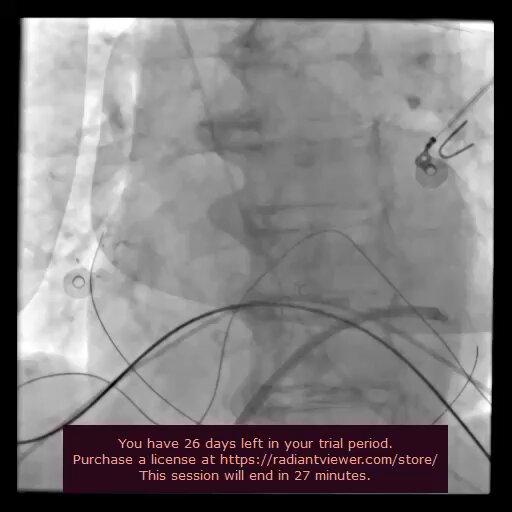
Here’s an interesting image of coronary spasm after cardioversion! @timucin_alt @akyurek_omer.
1
1
11
Of note, LPs reappeared couple of minutes later and epi ablation was required. @elifoykucelik @ozkanatfirat @seeenaaay.
0
0
2
Check out the prolongation and dissappearance of epi LPs(pentaray 13-14&15-16) during endo Rf. #EPeeps @timucin_alt @akyurek_omer
2
1
21
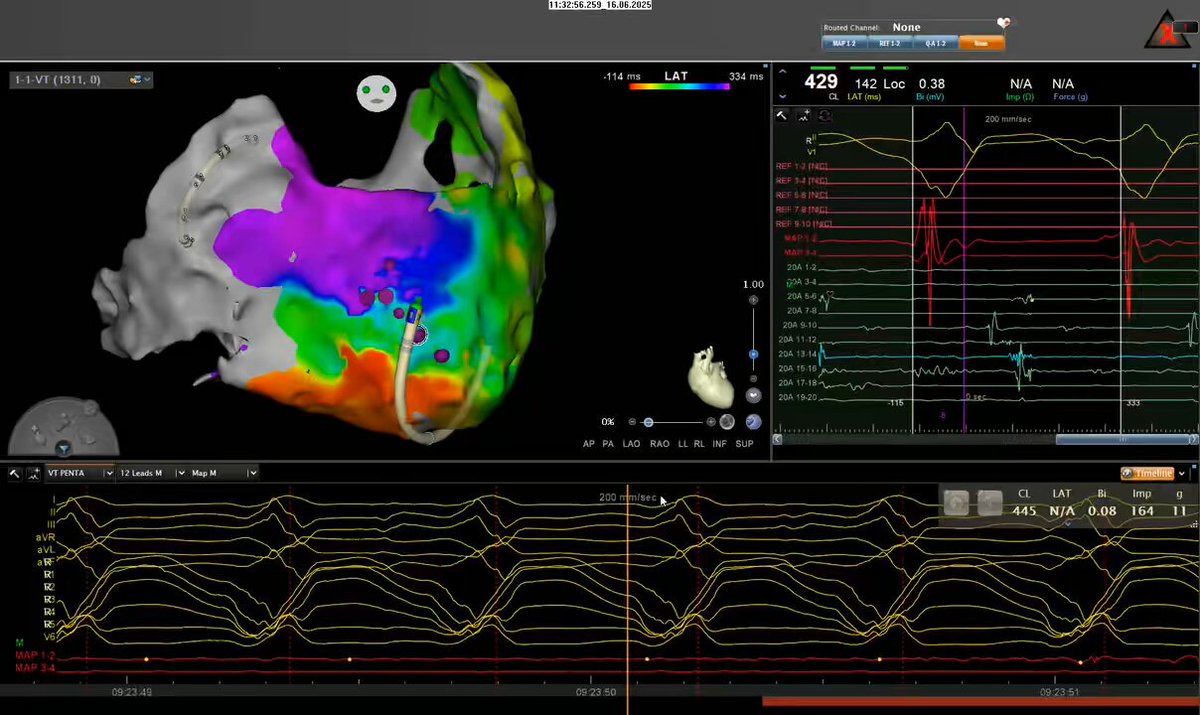
@akyurek_omer @timucin_alt @ozkanatfirat @seeenaaay @elifoykucelik 95% pacematch from distal annular vein.

0
0
2
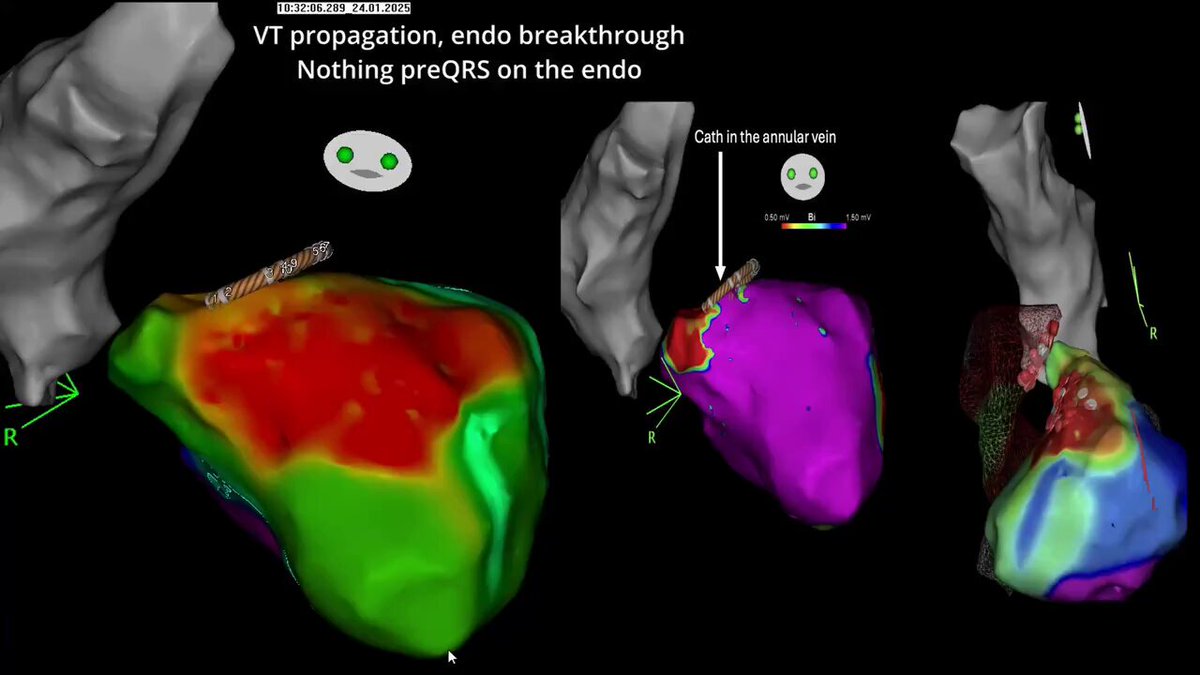
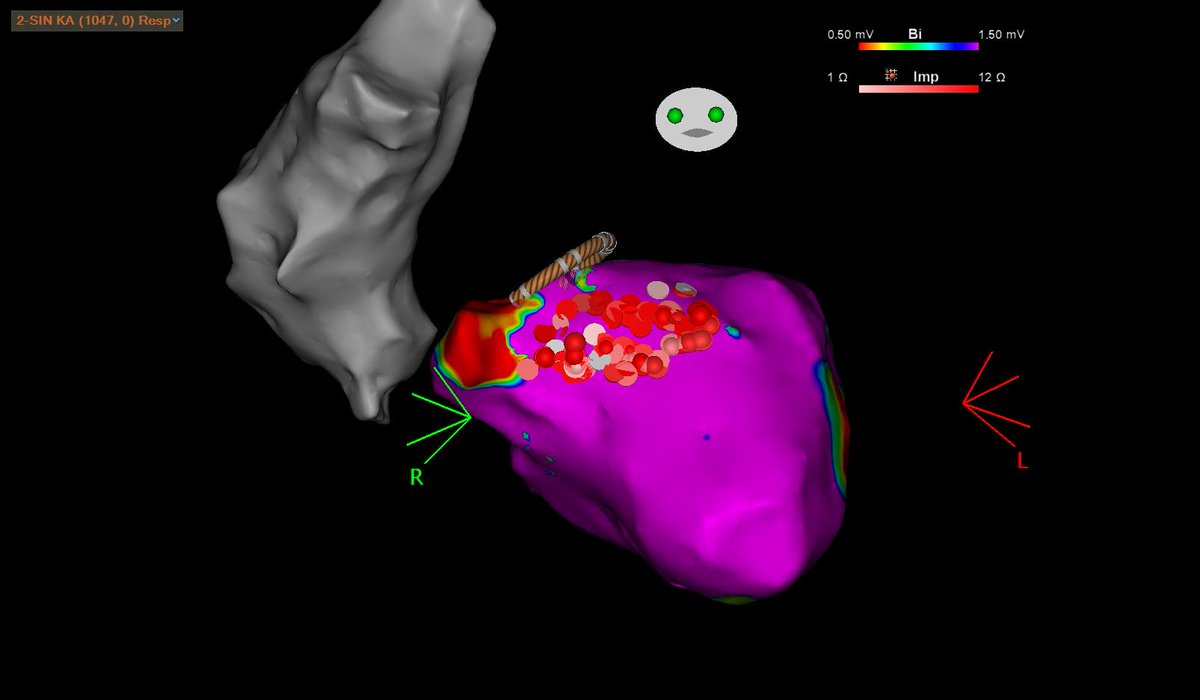
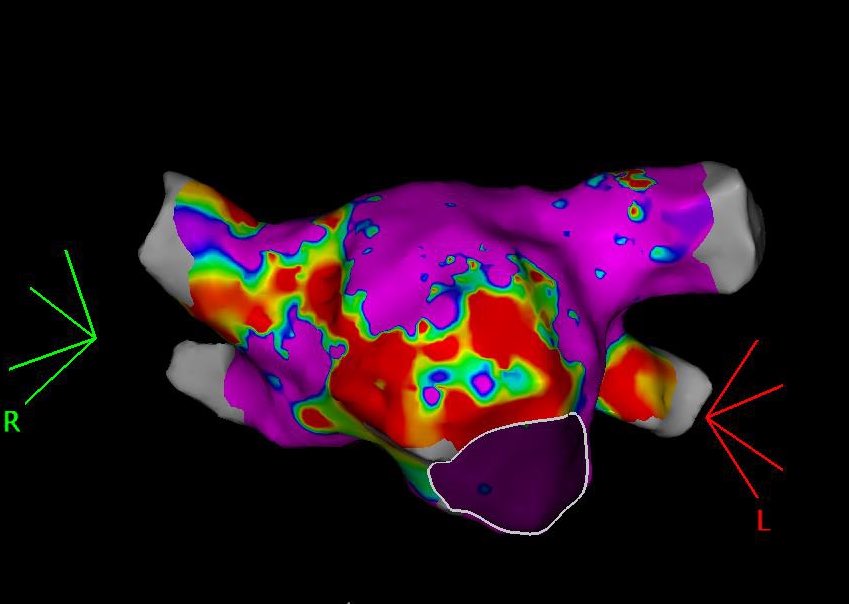
#EPeeps LV summit VT(+ICDshock) in a pt w bioprosthetic AVR&MVR. Endo breakthrough@QRS onset. Only precocity @ annularV (30ms). Extensive anatomical abl (endo+PA) fails, while ETOH inf. makes VT non-inducible. @akyurek_omer @timucin_alt @ozkanatfirat @seeenaaay @elifoykucelik

5
3
37
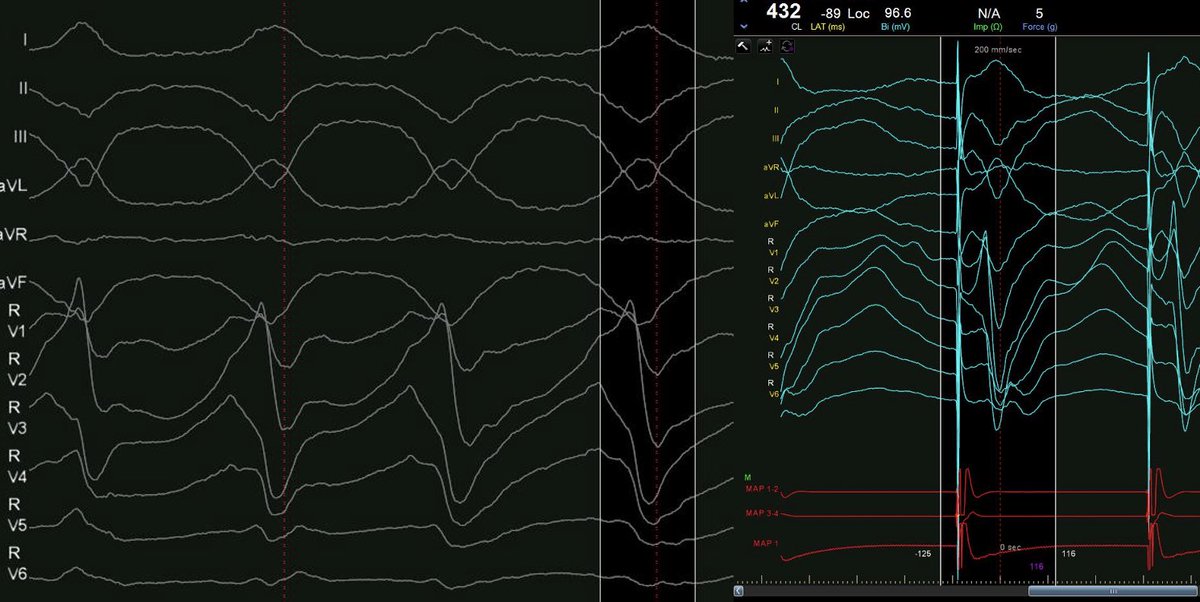
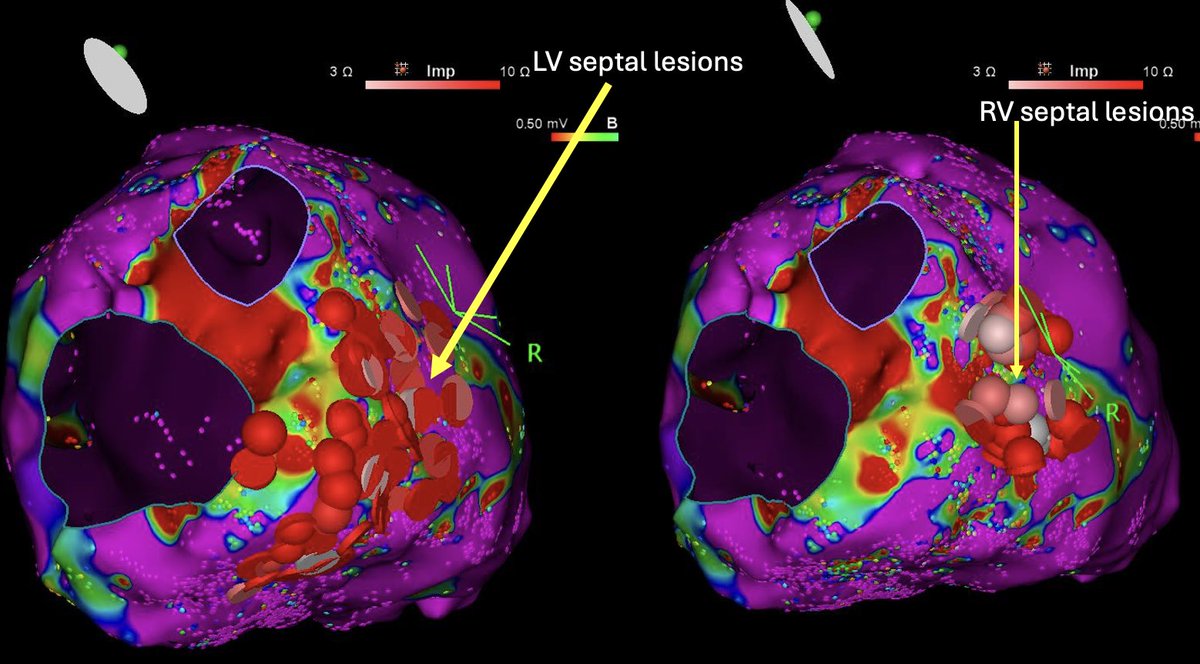
#Epeeps Classical presentation of midmyocardial septal scar and VT. Patchy biV LVA, low uniV and an unstable VT that has 94% pacematch at the RV septum. Sequential burn renders VT non-inducible. @timucin_alt @akyurek_omer


0
3
30
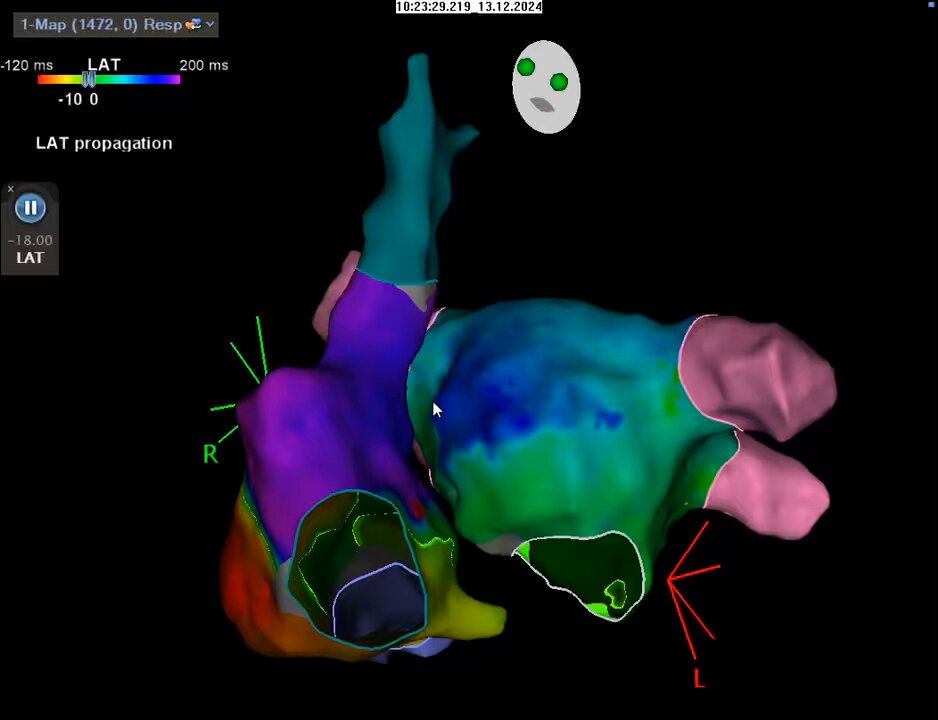
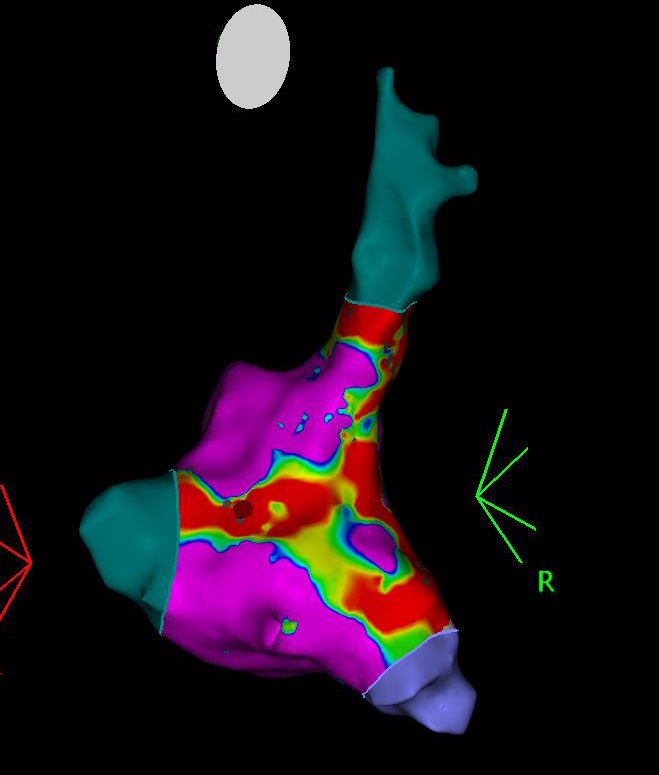
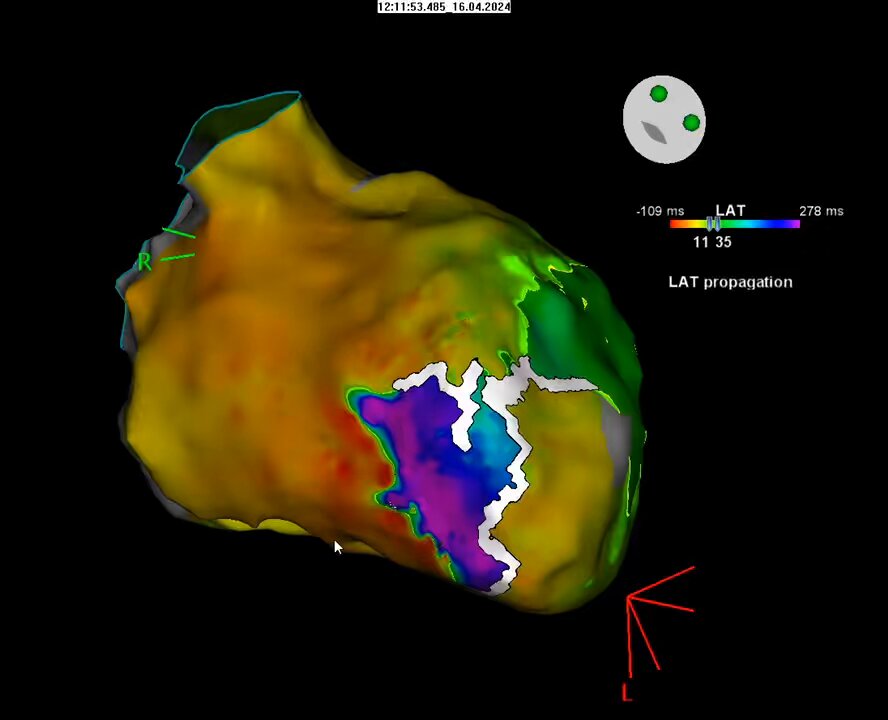
A biatrial flutter in a pt w septal scar w/o hx of abl! Easy to mistake for a cti flutter if only RA is mapped since only tiny portion of the cycle is missing. @akyurek_omer @timucin_alt #Epeeps
5
9
70
#Epeeps Intraprocedural Lead dysfunction manifesting as low bipolar imp(but normal uni!) in a fibrotic septum (postTAVR) after 2 attempts w torque build-up&entanglement prior to the optimal insertion. A visible defect was present on the lead which had to be replaced.




2
0
17

0
2
0
#Epeeps .Small patchy anterior wall bipolar LVA and huge unipolar LVA in an early revascularized anterior MI. Have a feeling that we’re gonna see this more often….Same pt, CL200ms apical VT w compl diastolic activation present in pentaray 9-10 bipol. @timucin_alt @akyurek_omer



0
4
31
A Pentaray-induced pvc leads to late local activation creating a reentry and then a #VT is unleashed. #ablateVT #Epeeps @akyurek_omer @timucin_alt @seeenaaay @elifoykucelik @ozkanatfirat

2
5
26
Epi #Rf terminates a slightly irregular AT within secs at a site w great EGMs. A large portion of the cycle missing at the endo with a large scar. Final lesion set is shown in both images. #Epeeps @timucin_alt @akyurek_omer @Arritmias_HRC @DrRoderickTung @ChristianHeeger @pjsm83



1
3
28
Concealed fusion, excellent stim-QRS and PPI-TCL= 0 vs. Activation map: the old meets the new. #Epeeps #ablateVT @akyurek_omer @timucin_alt @seeenaaay @elifoykucelik @E68754
0
2
20
Mitral apparatus hiding the critical component of a #VT circuit. A retroflexed Rf cath is needed to reach the critical site. Good contact ≠ contact w LV wall. ICE would have definitely helped . #Epeeps @akyurek_omer @timucin_alt #ablateVT
1
3
23
Two more basal VTs were induced, luckily extensive endocardial ablation achieved non-inducibility.


0
0
4
Despite the vox populi(and our opinion) this was a periaortic #VT. There was LVA at the basal LV, exit signals just beneath the aortic valve (76ms pre qrs). missing was the 120ms of early and mid diastolic actv. Nevertheless ablation at this site rendered this VT non inducible.


78y.o. M, hx of CABG (lad-lima, svg-rca), LVEF 15% , incessant VT. Where do #Epeeps suspect the isthmus is? 12 lead ECG on the next post.
3
1
14

78y.o. M, hx of CABG (lad-lima, svg-rca), LVEF 15% , incessant VT. Where do #Epeeps suspect the isthmus is? 12 lead ECG on the next post.
1
0
6