

Psychiatry Excellence
@psycheureka
Followers
10K
Following
7K
Media
1K
Statuses
8K
We provide psychiatry education for Psychiatrists, GPs & Mental Health Practitioners. • Join The Academy 👇
Australia
Joined March 2016
@psycheureka Nice thread. Many practitioners struggle to treat psychophysiological insomnia. CBT-I doesn’t work properly, nor do sleep hygiene/SC. I’ve seen cases with good PSG who do everything and not work and become dependent on benzos or Z-drugs. Any recommendation? Also threads is nice.
2
1
2

𝐈𝐧 𝐣𝐮𝐬𝐭 𝐭𝐰𝐨 𝐝𝐚𝐲𝐬, 𝐓𝐡𝐞 𝐀𝐜𝐚𝐝𝐞𝐦𝐲 𝐀𝐃𝐇𝐃 𝐌𝐚𝐬𝐭𝐞𝐫𝐜𝐥𝐚𝐬𝐬 𝐠𝐨𝐞𝐬 𝐥𝐢𝐯𝐞 𝐢𝐧 𝐌𝐞𝐥𝐛𝐨𝐮𝐫𝐧𝐞.🚀 We’ll be at the Langham Hotel with colleagues joining both in-person and online. I’ll be sharing what I’ve learned across more than a decade of
0
2
9
Want to refine your understanding of PTSD management? Join The Academy for clinician-focused courses covering PTSD symptoms, neurobiology and management strategies: Earn CPD points and translate evidence into practice 🎓 https://t.co/YRvxNiWH01
academy.psychscene.com
Gain a comprehensive understanding of Post Traumatic Stress Disorder (PTSD) with our expert-led course! Covering clinical features, neurobiology, phenotypes, diagnosis, and management, this course is...
1
1
6
PTSD recovery isn’t just symptom reduction—it’s restoring adaptive functioning. By improving the balance and coordination among the salience, default-mode and executive networks, patients regain emotional regulation, cognitive control and the ability to re-engage with life.
1
2
3
Pharmacological Approaches • SSRIs/SNRI: (e.g., sertraline, paroxetine; venlafaxine used per guidelines) help at the symptom level; network effects are an area of research. • Prazosin: May reduce trauma-related nightmares for some; evidence is mixed for overall PTSD symptoms.
1
1
3
How Therapies Work • Trauma-Focused CBT: First-line. Reduces symptoms by modifying appraisals and avoidance; imaging suggests normalisation of abnormal network interactions. • EMDR: First-line. Mechanism not settled; a leading account is working-memory taxation during
2
1
3
Why do some recover while others develop chronic symptoms? Resilience and vulnerability factors matter—e.g., social support, prior mental health, and stress biology. Evidence-based early assessment and treatment improve outcomes. Routine single-session psychological debriefing
1
1
2
The Role of the Anterior Insula The anterior insula helps switch between the DMN (internal focus) and CEN (goal-directed control). In PTSD, switching can be impaired—leaving patients “stuck” in reactive states with limited top-down regulation. A promising mechanistic account,
1
1
2
How network disruptions show up clinically • Intrusions: flashbacks, distressing memories • Avoidance: of trauma-related cues • Hyperarousal: sleep disturbance, exaggerated startle Each arises from interacting neurocognitive changes rather than a single circuit failure.
1
1
2
Central Executive Network (CEN/FPN) The DLPFC and frontoparietal control systems support regulation of attention and emotion. In PTSD, altered engagement/connectivity is linked with: • Difficulty managing intrusive memories • Reduced cognitive flexibility
1
1
3
In PTSD, altered connectivity in hubs such as the mPFC and PCC relates to difficulties with self-referential processing and autobiographical memory—contributing to: • Flashbacks • Intrusive thoughts These experiences reflect dysregulated memory processing rather than a
1
1
6
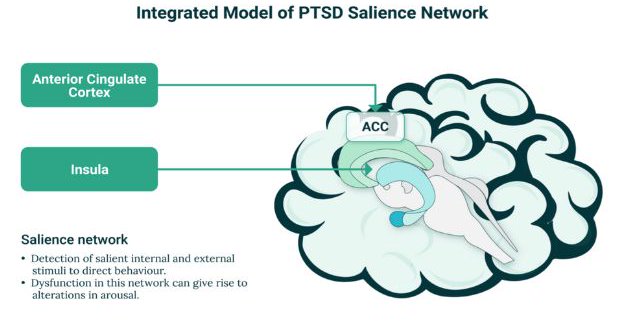
The Salience Network Heightened signalling in the anterior insula and dorsal ACC can bias threat appraisal, making neutral cues feel unsafe. This helps explain: • Hypervigilance • Heightened arousal Competitive dynamics with other networks may occur, but direct “resource
1
1
5
The Integrated Model of PTSD highlights these networks: • Salience Network: Detects and prioritises salient/interoceptive and potential threat cues. • Default Mode Network (DMN): Supports autobiographical memory and self-referential processing. • Central Executive Network
1
1
4
Why do some individuals recover from trauma while others develop PTSD? A useful lens is how three large-scale brain networks interact: • The Salience Network (SN) • The Default Mode Network (DMN) • The Central Executive/Frontoparietal Network (CEN/FPN) Understanding their
4
21
86
Learn more about the neurobiology and pathophysiology of insomnia on the Psych Scene Hub: https://t.co/iwkU15nUJf

psychscenehub.com
Insomnia is more than difficulty sleeping; it affects cognition, mood, and overall health. Linked to neurobiological imbalances, insomnia doubles the risk of depression and disrupts immunity. Explore...
0
1
4
Insomnia is best conceptualised as a 24-hour hyperarousal disorder involving cognitive, cortical and autonomic systems; precise causal pathways remain under investigation. Understanding diagnostic criteria, circadian factors, and common psychiatric/medical links helps identify
2
0
3
7. Assessment Tools A sleep diary tracks bedtimes, awakenings, sleep quality, and routines. Actigraphy offers movement-based estimates of sleep but may be inaccurate in insomnia. Polysomnography remains the gold standard when other sleep disorders are suspected.
1
0
2
6. Validated Scales Use standardised tools to support assessment and monitoring: • Insomnia Severity Index (ISI) or Sleep Condition Indicator (SCI) to quantify insomnia severity and change over time. • Pittsburgh Sleep Quality Index (PSQI) for global sleep quality. •
1
0
2
5. Risk Assessment Evaluate daytime sleepiness and safety-critical activities. Ask specifically about driving and operating machinery; follow DVLA fitness-to-drive guidance when excessive sleepiness is present.
1
0
2
4. Psychosocial Factors Assess perfectionism, evening cognitive/emotional arousal, and limited wind-down time. Consider caregiving duties, stressful events, or bedtime disruptions. Note sleep disturbance from pets or household demands.
1
0
3