

Jonas Willmann, MD
@jonas_willmann
Followers
410
Following
986
Media
27
Statuses
338
Radiation Oncologist | Research scholar @MSKCancerCenter and @Unispital_USZ | interested in 🫁, reirradiation & oligometastatic disease
Brooklyn, NY
Joined March 2014
🚨 just published @ESTRO_RT and @EORTC consensus on re-irradiation: definition, reporting,.and clinical decision making . @TheLancetOncol #radonc. A thread 🧵 . 👇 1/n.
4
46
108
RT @SawsanRashdanMD: Honored to share results of our IIT Phase II trial of osimertinib + consolidative RT in EGFR+ NSCLC, now published in….
0
29
0

Blazing-fast image creation – using just your voice. Try Grok Imagine.
284
562
3K
@RadOncUSZ @IJROBP 12/ Grateful to our international collaborators including Rob Olson, Sarah Baker, @SahgalArjun, Hanbo Chen, @umbertoricardi, @NAndratschke @Mat_Guc @IyengarPuneeth @EChrisDee and many more.
0
0
5
@RadOncUSZ @IJROBP 11/ Future directions:. 🔹Validate DMV in prospective studies guiding clinical decision making. 🔹Refine in histology-specific analyses. 🔹Explore biological foundations of DMV and metastatic trajectories.
1
0
4
@RadOncUSZ @IJROBP 10/ Potential use cases:.DMV stratifies outcomes after progression on metastasis-directed #SBRT. It may support:. ➡️Patient selection for repeat local therapy. ➡️Informing systemic therapy continuation vs. escalation. ➡️Integration into multimodal prognostic models.
1
0
3
@RadOncUSZ @IJROBP 9/ Why DMV matters:. 🔹 Simple: derived from routine imaging using basic arithmetic. 🔹 Dynamic: can be recalculated at each progression. 🔹 Generalizable: reproducible across cancers & cohorts.A practical tool for post-progression decision-making in OMD.
1
0
3
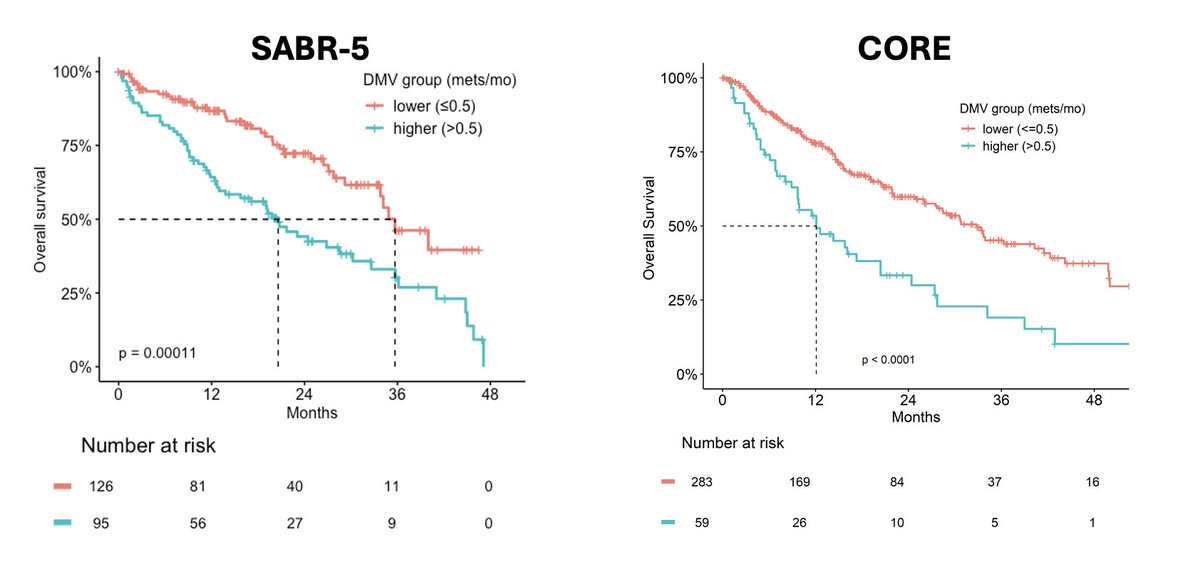
@RadOncUSZ @IJROBP 8/ Results — WFFS (repeat OMD only):. ✅SABR-5: trend toward shorter WFFS with high DMV (NS). ✅CORE: 18.8 mo (low DMV) vs 6.1 mo (high DMV), p<0.0001.
1
2
3
@RadOncUSZ @IJROBP 7/ Results — OS:. ✅SABR-5: median OS 35.7 mo (low DMV) vs 20.6 mo (high DMV), p=0.0001. ✅CORE: 32.8 mo vs 12.1 mo, p<0.0001.
1
0
3
@RadOncUSZ @IJROBP 6/ In this new study, we asked: does DMV hold up across tumor types & settings?.We analyzed:. 👉Prospective SABR-5 trial (n=221) 🇨🇦. 👉Retrospective CORE study (n=342) 🇨🇦🇺🇸🇮🇹.Both included pts with ≤5 mets progressing after metastasis-directed SBRT

2
0
2
4/ We previously proposed DMV, from the @RadOncUSZ cohort 🇨🇭:. 👉DMV = number of new/progressive metastases ÷ months to progression after prior SBRT. ⬆️ Higher DMV was linked to:. ⬇️Worse overall survival (OS). ⬇️Shorter widespread failure-free survival (WFFS) in repeat OMD.
1
1
5
3/ Background:.After SBRT or other local ablative therapies for oligometastatic disease (OMD), distant progression often dictates outcome. Post-progression treatments include:. 🔹Repeat local therapy. 🔹Continue or change systemic therapy.But no validated prognostic tools exist.
1
0
3
2/ Now published in the European Journal of Cancer. Full text 🔗
1
2
4
Distant failure after SBRT for oligometastatic disease is a common pattern of progression. Yet, we lack validated post-progression models to guide treatment. We tested whether Distant Metastasis Velocity (DMV) can fill this gap - and validated it across multinational cohorts 🧵
7
19
51
RT @DrJNaidoo: DUART trial 1yr durva after RT alone for stage III unresectable nsclc @ESMO_Open. - 102pts (defRT=53; palRT=49); PS2 7.9% .-….
esmoopen.com
Currently, patients with unresectable stage III non-small-cell lung cancer (NSCLC) ineligible for chemotherapy receive radiotherapy alone, with unsatisfactory results. DUART was a phase II single-arm...
0
16
0
RT @RobertoFerrara_: Want to dive into patterns, biomarkers and strategies to overcome primary and acquired resistance to immunotherapy in….
nature.com
Nature Reviews Clinical Oncology - Immune-checkpoint inhibitors have dramatically improved the outcomes in patients with advanced-stage driver-negative non-small-cell lung cancer (NSCLC), although...
0
20
0
RT @Cancer_Cell: KEAP1 and STK11/LKB1 alterations enhance vulnerability to ATR inhibition in KRAS mutant non-small cell lung cancer https:/….
0
41
0
RT @DrewMoghanaki: New data from the randomized PEMBRO-RT study demonstrate when an ICI-mediated Abscopal effect is most likely to occur in….
0
53
0
🫁 Intrathoracic relapse after PACIFIC-regimen for LA-NSCLC remains a major therapeutic challenge. 🧪 In the AUSTRAL trial, led by @Mat_Guc & @AndrearicFili, we target this unmet need by combining RT (reRT and/or metastatis-directed SBRT) + durvalumab + ceralasertib

2
17
32
RT @deadoc80: Glad to share our most recent @NatRevClinOncol piec on #microbiota #radiotherapy and #cancer #immunotherapy. Kudos to Jianzho….
0
9
0