
George Tolis
@georgetolisjr
Followers
8K
Following
32
Media
110
Statuses
1K
Median sternotomy, pump, Prolene, Steinway. Not certified for Cor-Knot or Atriclip.
Boston, MA
Joined July 2012
Now open access PDF. We need to tighten up our statistical arguments in cardiac surgery if we are to make bold statements about new techniques. Industry sponsored observational studies written by authors with COI and promoted by podium presentations is not good science.

Parish A, Tolis G, Ioannidis JPA. Across 73 meta-analyses mortality improvements are uncommon with newer interventions in adult cardiac surgery. J Clin Epidemiol. 2025
4
12
114
Why does it cost in the US $350,000 to get an undergraduate degree added to $400,000+ to get a medical degree? Why have years of research between school/training become mandatory forcing doctors to start practicing in their mid/late thirties and accumulate debt up to that point?
15
16
109

$1B and climbing. USDG’s growth is powered by the 100+ institutions and innovators building Global Dollar Network.
4
6
31
At our local Peterson School of the trades in MA it costs $10,950 for the 550 hrs (1-2 years) to become a licensed plumber. One can start at age 20 and by age 30 could be earning north of $300K/year. No threat from AI in the foreseeable future. In medicine we are eating our own.
6
9
102
In my opinion the main barrier today is the quality of the meetings/publications and the selection criteria for the speakers combined with their conflicts of interest more so than any language barrier. A truly sad state of affairs for our field.

@georgetolisjr Perhaps with the main barrier today being no longer a political one, but rather the language. Russian language sources seem far harder to work with.
0
3
20
For the history buffs, the contribution of Soviet physicians in medicine is immense, yet it was systemically suppressed from the free world, with the aid of their own system which kept many dissidents in the margins of Soviet society.
4
5
59

Web designers like @reijowrites bring powerful interactions to the web with one platform: Framer
0
4
54
I guess cardiac surgery and the Maury Povich show @TheMAURYShow have a lot of similarities.

@georgetolisjr More than one father. Not a painful choice.
3
2
28
As painful as it may be for many “westerners” (myself not included), the father of CABG is Soviet surgeon Vasily Kolesov, a Great Patriotic War hero from Leningrad. This does not diminish the contributions of DeBakey, Cooley and Favaloro who popularized CABG in the modern era.
10
10
133
I recently did one of the toughest (re) operations in my 23 year career : a CABG on a patient who underwent pericardiectomy 20 years ago. STS score 0.88%. Risk adjustment is a well intended strategy which disincentivizes surgeons from offering their skills to patients in need.
8
7
93
The best treatment for afib remains elusive. Congratulations to the authors on a great study free of biases and fanfare.

Bad news for enthusiasts of left atrial appendage closure from #AHA25. CLOSURE-AF is not yet published, but reports from New Orleans indicate inferiority compared with best medical care (the trial was designed for non-inferiority, making this the most unexpected and unfavorable
1
9
58
Where is August Alsina? His Rise Was Followed By Scandal

parlemag.com
Parle Mag - The Voice of The Culture, bringing you the latest in lifestyle, entertainment, and culture.
3
3
43
Thank you for your support @weldeiry and for the honor of your friendship!

Congratulations to @georgetolisjr at @BrighamWomens on his election this afternoon to honorary membership in the Interurban Clinical Club. Dr. Tolis is at the forefront of Cardiac Surgery (he proved it by saving my life in July, 2025) while being committed to training and
1
1
25
Over 370 pictures of this

@georgetolisjr Share some images! Old books are indeed treasure 👇🏼 https://t.co/8K8bHL2iNc
3
16
150
This is one of the most amazing cardiac /aortic textbooks ever published. Discontinued a long time ago. Phenomenal drawings and angiogram stills from the pre CT era. If you are fortunate enough to have it, guard it like a treasure.
7
16
201
If a dual stage venous cannula cost $35,000 instead of $35, what would the CABG literature look like today?
2
1
42
My point was not that this data is inaccurate but rather that the @nejm is basically publishing a study stating something along the lines that the roadworthiness of a Land Rover and a Toyota Corolla is the same 7 years after the two vehicles were purchased.

@georgetolisjr We clearly need the 10-year data. The median age in P3 was 74, an age group where a lesser invasive therapy is reasonable if possible. We should not claim this data shows one therapy's superiority yet…however, it's encouraging that in 2 RCTs (P3/NOTION) where patients were
1
0
31
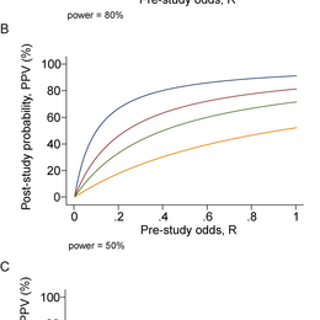
20 years old but so relevant today… https://t.co/ZdkNpiDaTg
journals.plos.org
Published research findings are sometimes refuted by subsequent evidence, says Ioannidis, with ensuing confusion and disappointment.

@georgetolisjr This is a randomized trial. Not at all like the observational studies of smokers vs non smokers.
1
1
19
These studies remind me of tobacco company-sponsored studies in the 1950s that showed no early mortality differences between smokers and non-smokers.

Presented at #TCT2025: In low-risk patients with severe aortic stenosis, transcatheter and surgical aortic-valve replacement had similar 7-year survival and valve durability outcomes, with no evidence of differences in composite end points. Full PARTNER 3 trial results:
12
20
127
The redo arch (with previous ascending replacement) feels to me technically easier than a virgin sternotomy total arch replacement. It almost seems that the graft originally placed pulls down the entire arch bringing the arch vessels closer to the operative field. Any opinions?
9
1
34
Another rare case from the recent past. Chronically trapped Sapien TAVI in the aortic arch, removed under DHCA. Patient with months of TIAs pre op, complete resolution after removal.
3
14
94
I think it is a matter of time before someone creates an AI enhanced video of a procedure and successfully submits it to a meeting for presentation.
1
2
45
You must have had the privilege over those past 25 years of working with exceptional surgeons who make a CABG look simple. It isn’t.

@spartywrx @georgetolisjr To be fair I’m a PA with 25 years in CT surgery I could probably make it though a CABG
4
2
102
Maybe I am naive and not a deep thinker, but I am not worried one bit about AI claiming my cardiac surgery job or that of the generation that follows me. I am extremely worried, however, about the dismantling of the standards that lead to credentialing and promotion in my field.
15
16
264