

Greg Hayes
@canuc_57
Followers
800
Following
2K
Media
443
Statuses
4K
Chief of Vascular Surgery @ProvSwedish. alum @UofTSurgery @UofTVascular🇨🇦 @shocktrauma Triple Boarded #aorta #carotid #dissection #CLI #spineaccess
Seattle, WA
Joined May 2016
RT @DudespostingWs: Dude who went out to sea in Norway captured footage of a massive shark he encountered.
0
11K
0
RT @JaysCare: This weekend, we celebrated the opening of Riverside Park, a new Field Of Dreams made possible by @td_canada in Pembroke ON!….
0
31
0

Blazing-fast image creation – using just your voice. Try Grok Imagine.
13
13
106
RT @MaherSabalbal: carotid endarterectomy will likely never be replaced. It is good old fashioned surgery that has withstood decades of try….
0
3
0
Time for cold one in the Great White North, thank you John Molson 1786 🇨🇦

1
0
5

0
0
0
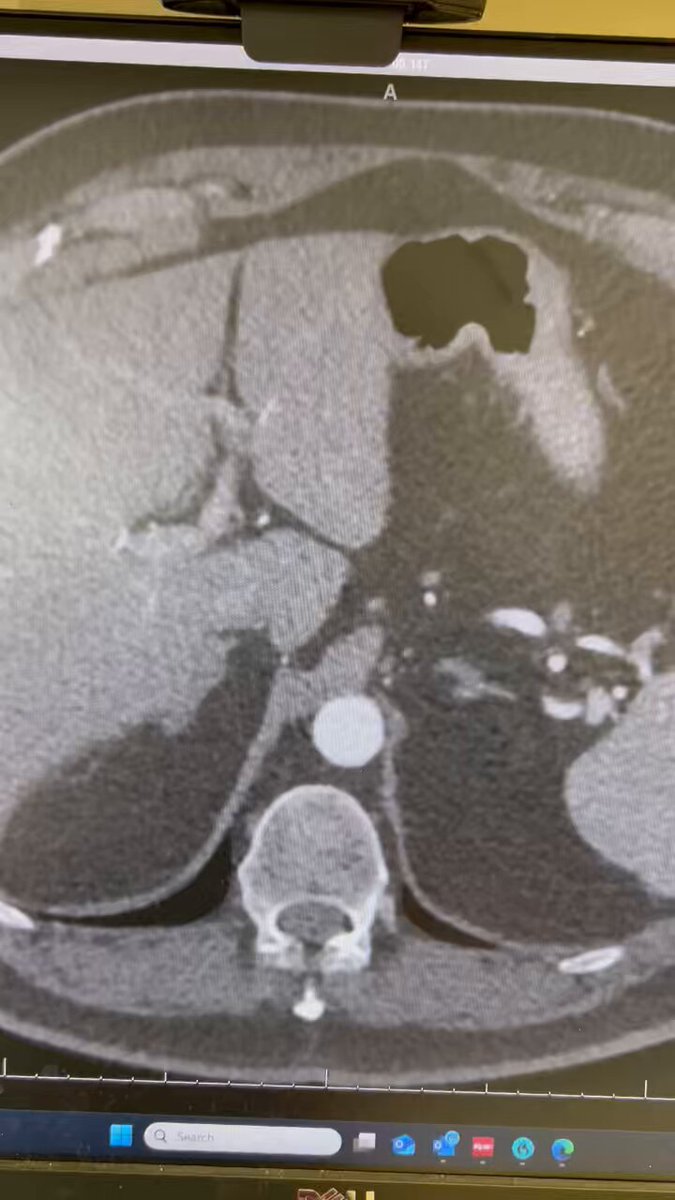
Your wish is my command @AmputationSuck! 68yo M, solitary kidney, CKD-3, 3.6cm R renal artery aneurysm. Workup? WWYD? @VascularSVS @CanadianSVS @MaherSabalbal @AWBeckMD @mattsmeds @academicaorta @farkomd @jmills1955

7
2
21
55yo active male, 3.5 cm pop aneurysm, adequate GSV, 3 vessel runoff, good landing zone for covered stent. Preferred Rx?.@VascularSVS @CanadianSVS.
5
2
4


Thank you Joe!.
Please don't spread disinformation. Upper extremity DVT in competitive athletes is most commonly related to venous TOS (Thoracic Outlet Syndrome) or Paget-Schroetter Syndrome. #VascularSurgery.
0
0
1
A beautiful brisk evening on call in #Seattle. Those illuminated construction cranes are building our new @ProvSwedish tower. #PNW

0
0
2

RT @LasVegasLocally: Amphibious 'Super Scooper' airplanes from Quebec, Canada are picking up seawater from the Santa Monica Bay to drop on….
0
7K
0
Looks like the women need to teach the men a few things @HockeyCanada.

0
0
2
Disappointing.

History repeats! Czechia beats Canada in quarter-finals and moves on.🇨🇿💪. @czehockey #WorldJuniors #CZECAN #IIHF

0
0
0
As the father of 3 daughters, this is awesome. I applaud these 4 young men.

0
0
4
Flags will be at half mast in 🇨🇦.
UPSET ALERT! Latvia beat Canada in a shootout drama for the first time ever at #WorldJuniors.🇱🇻💥 . Full game story ➡️ #LATCAN #IIHF @lhf_lv

0
0
0