
Sam S. Chang MD, MBA
@UroCancerMD
Followers
4K
Following
15K
Media
81
Statuses
1K
Patricia and Rodes Hart Endowed Chair, Chief Surgical Officer, Vanderbilt Ingram Cancer Center
Nashville, TN
Joined August 2011
It was great connecting with colleagues, attending meaningful educational sessions and celebrating the work of urologic oncology at the SUO 2025 Annual Meeting in Phoenix. Thank you to everyone who joined us and helped make it such an excellent event.
0
5
23

This is really impressive @jteoh_hk especially also the presence of detrusor muscle in all specimens could indicate that we may be able to get consistent and reliable resection quality with VES #BladderCancer @EurUrolOncol @Oncodaily #ERBT

Hot off the press!! First reported case series of transurethral robotic en bloc resection of bladder tumour using the Virtuoso Endoscopy System (VES). Published in @EurUrolOncol today! (1/n) #ERBT #UroSoMe
0
3
18
As a patient— why wouldn’t I want my surgeon to have best possible access, manipulation, and ability to remove all my tumor
VES is a novel robotic surgical system that allows transurethral ERBT. The concentric tube design of the instrument arms allows controllable manipulation at a small diameter of ~1mm. This is extremely crucial to allow a two-handed surgery w/o obscuring the endoscopic view. (2/n)
0
2
30
ERBT is only the beginning! Having a transurethral robotic system with different instruments (e.g.needle holder) allows us to explore new surgical approaches that can never be achieved b4. As a urologist, we should gear up for another exciting robotic journey in the future! (4/n)
2
8
53
We did 6 cases of robotic ERBT in 2 days. 100% detrusor muscle presence, 100% successful ERBT/ modified ERBT, 91% evaluable margins and clear resection margins, no grade 2 or above complications. Small number for sure but the results are indeed very promising. (3/n)
1
6
32
VES is a novel robotic surgical system that allows transurethral ERBT. The concentric tube design of the instrument arms allows controllable manipulation at a small diameter of ~1mm. This is extremely crucial to allow a two-handed surgery w/o obscuring the endoscopic view. (2/n)
3
19
73

#SUO25 Preview: #BladderCancer data from BCG-unresponsive to metastatic disease. @pjhensley11 @UKYMedicine joins @UroCancerMD @VUMCurology to discuss the bladder cancer session at the 2025 @UroOnc meeting, highlighting several clinical trial updates. #WatchNow on UroToday >
0
2
7

Best of the best! Multidisciplinary care & trials increasingly crucial across the bladder Ca/UTUC spectrum. #UromigosLive @JoshMeeks @UroCancerMD @OncoAlert @Uromigos @LauraBukavinaMD @UrogerliMD @IBCG_BladderCA
2
4
18

https://t.co/F33X7MplDG TMT for MIBC is a crucial treatment option for our patients. 💵However, its current costs are unsustainable, especially with the growing interest in expanding its use.
3
13
44
Real-world experience with nadofaragene firadenovec treatment for BCG-unresponsive #BladderCancer. @MarkTysonMD @MayoClinic & @MaxKates @brady_urology join @UroCancerMD @VUMCurology sharing real-world tips on optimizing nadofaragene firadenovec for BCG-unresponsive #NMIBC. Rectal
0
3
17
#SunRISe1 trial shows #TAR200 efficacy in BCG-unresponsive #BladderCancer. @DrFelixGuerrero sits down with @UroCancerMD @VUMChealth discussing SunRISe-1 results — TAR-200 shows 85% DFS at 6mo in BCG-unresponsive papillary-only #bladdercancer. ➡️ Similar responses in high-grade
0
8
15
#CISTO study: Comparing cystectomy vs. bladder-sparing therapy for recurrent #NMIBC. John Gore, MD, MS @fredhutch joins @UroCancerMD @VUMCurology breaking down the CISTO study - a patient-driven, prospective look at cystectomy vs intravesical therapy for recurrent NMIBC. 💥
0
4
14
Delighted to announce Noah Hahn & Max Kates @MaxKates new CoDirectors of Greenberg Bladder Cancer Institute @brady_urology Gratitude to David McConkey for steadfast leadership & wish him luck in new role at U of R. Excited for future! @BladderCancerUS @HopkinsMedicine
6
9
73

@JoshMeeks provides an amazing overview of the significant data emerging in the BCG-unresponsive NMIBC space, focusing on the CIS cohorts. We also discuss the recent ODAC decision on UGN-102 for lower risk disease which was recently FDA approved. https://t.co/xMrAN0SxPk
1
30
76
Congrats and so well-deserved! @MaxKates

Congratulations Max Kates @MaxKates The R. Christian B. Evensen Professor in Urology, one of the highest honors in academic medicine. A superstar surgeon-scientist, teacher, and all around amazing person. @bradyurology @HopkinsMedicine
2
0
10
Congratulations Max Kates @MaxKates The R. Christian B. Evensen Professor in Urology, one of the highest honors in academic medicine. A superstar surgeon-scientist, teacher, and all around amazing person. @bradyurology @HopkinsMedicine
16
12
108
Circulating and urinary tumor DNA in #BladderCancer treatment and surveillance. @alantanmd joins @UroCancerMD to discuss how these biomarkers provide real-time snapshots of disease status with significant prognostic value, highlighting that ctDNA positivity after neoadjuvant
0
3
13

BCG > gem for LG IR-NMIBC (better RFS); RARC = ORC (RAZOR: no diff in major comps/readmits —>frailty is the key); bilateral > unilateral primary RPLND for stage II seminoma (cuts RP relapse, ~15% crossover). Good stuff in @JUrology this month:
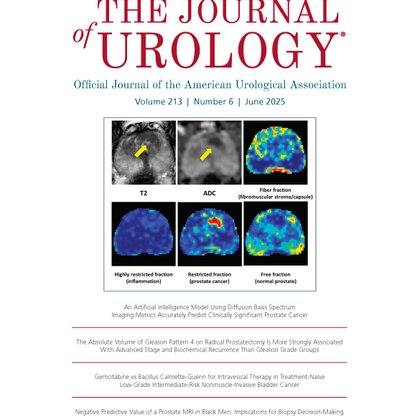
auajournals.org
3
10
25
Perioperative systemic therapies for muscle-invasive #BladderCancer. Jacqueline Brown, MD @WinshipAtEmory joins @UroCancerMD @VUMCurology to discuss recent advances, including the #NIAGARA trial combining chemotherapy with durvalumab, and emerging data on antibody-drug conjugates
1
2
7
#BOND003 Cohort P results for BCG-unresponsive papillary bladder tumors. @MarkTysonMD @MayoClinic joins @UroCancerMD @VUMCurology discussing early results from BOND-003 Cohort P: 90.5% HG-RFS at 3 & 9 months with oncolytic immunotherapy cretostimogene. Well-tolerated & CIS-free
0
2
6