

Rajesh Sasidharan
@SRajesh_IR
Followers
2K
Following
2K
Media
148
Statuses
512
HPB and GI Interventional Radiologist @Rajagiri_Hosptl | @MAMC_NewDelhi and @ILBS_India alum | Passionate about interventions in portal hypertension
Cochin, India
Joined May 2020
Inviting applications for our Hepatobiliary Interventional Radiology Fellowship. Last date for submitting applications - 15th June, 2025. Course commencement - 1st July, 2025. Send your CV to - Rajesh.S@rajagirihospital.com
0
2
28
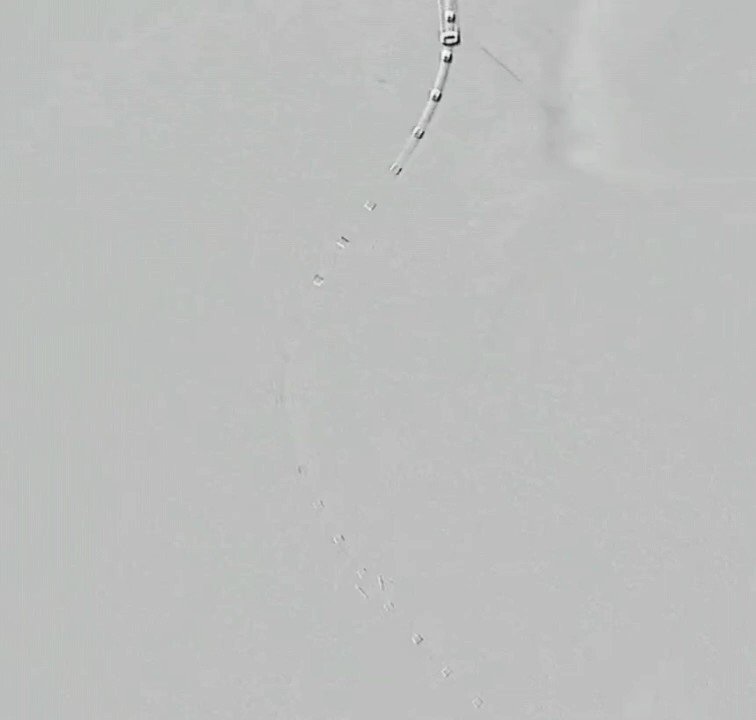
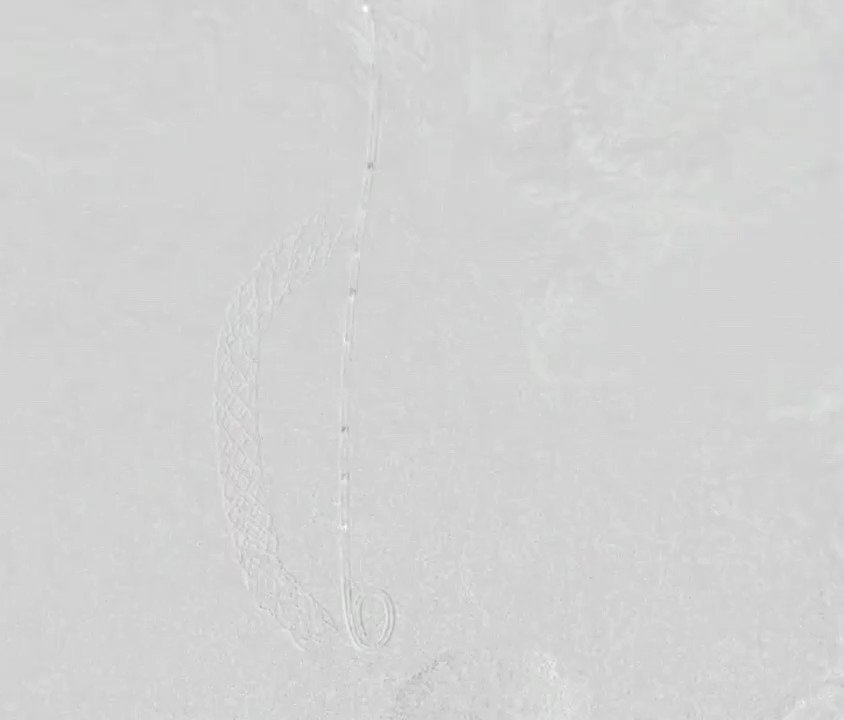
Parallel guidewire anchoring technique for cannulating a blocked TIPS stent.
5
11
109
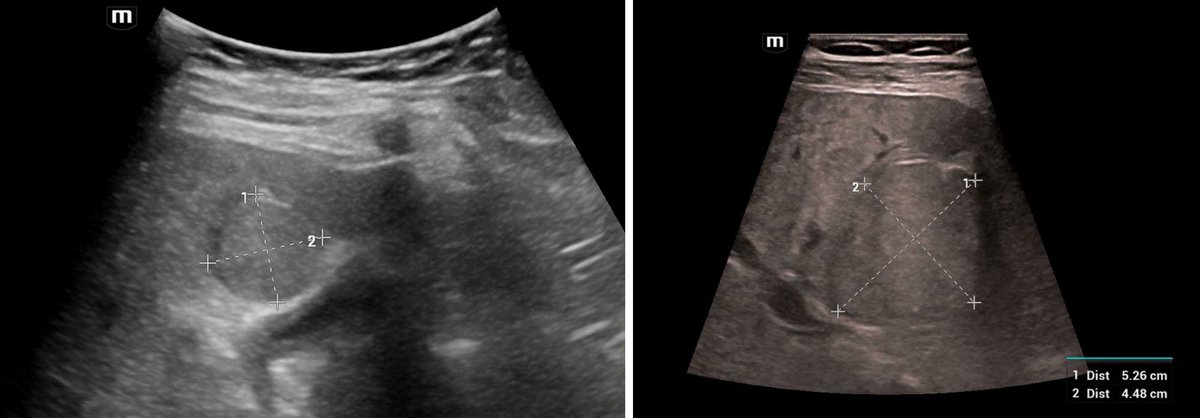
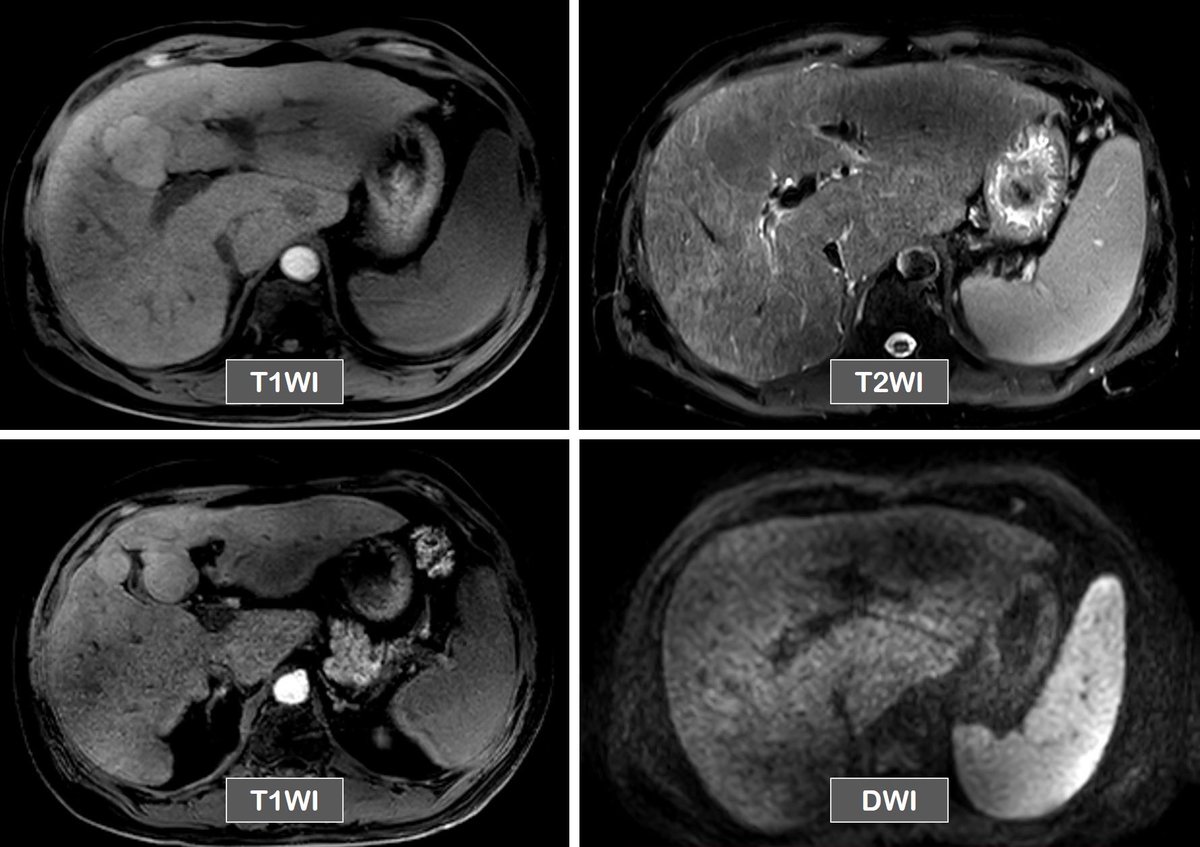
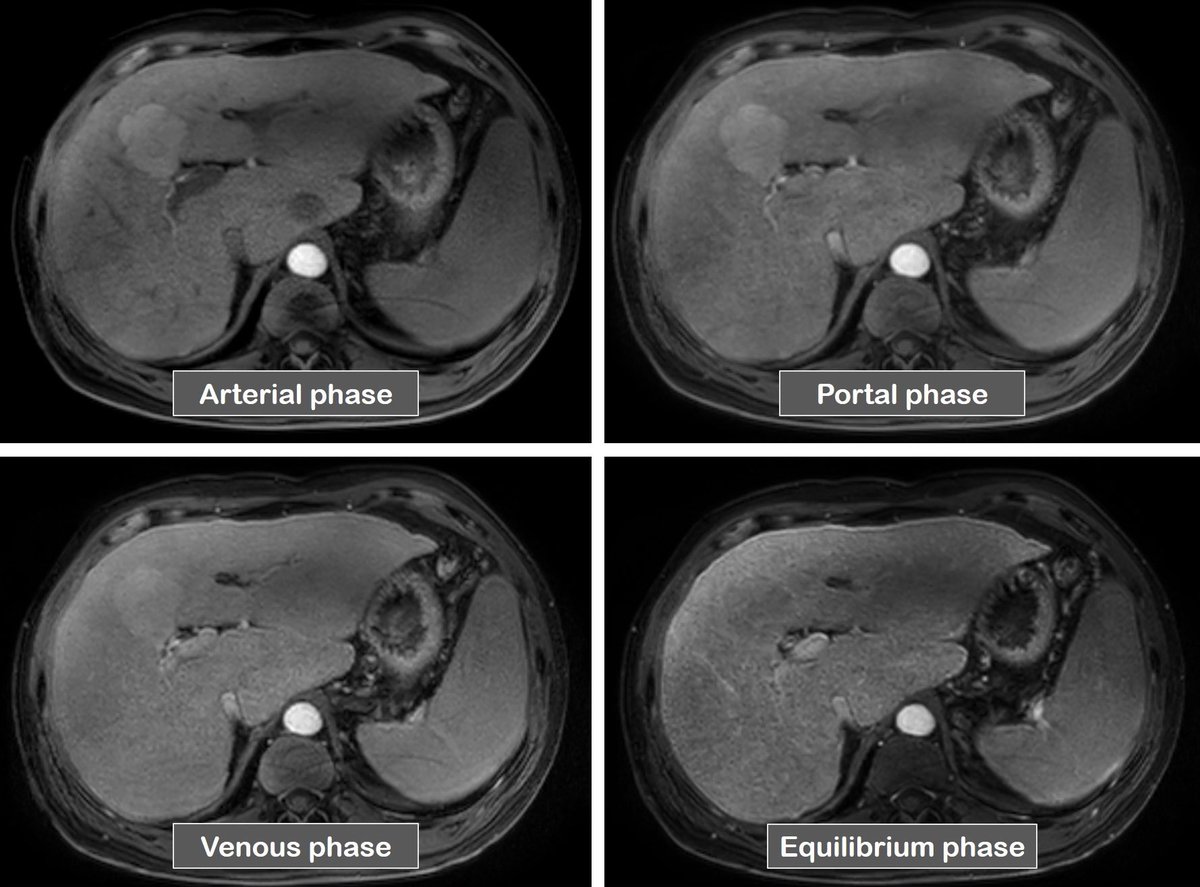
48 yo man, alcohol associated liver disease. Focal lesion in segment 4 wrapping around GB fossa in an inverted V shape. CT - Arterial enhancement. No convincing washout. MRI - T2 hypo, T1 hyper, no diffusion restriction, washout +. Subtraction images not available. Thoughts?

3
2
14
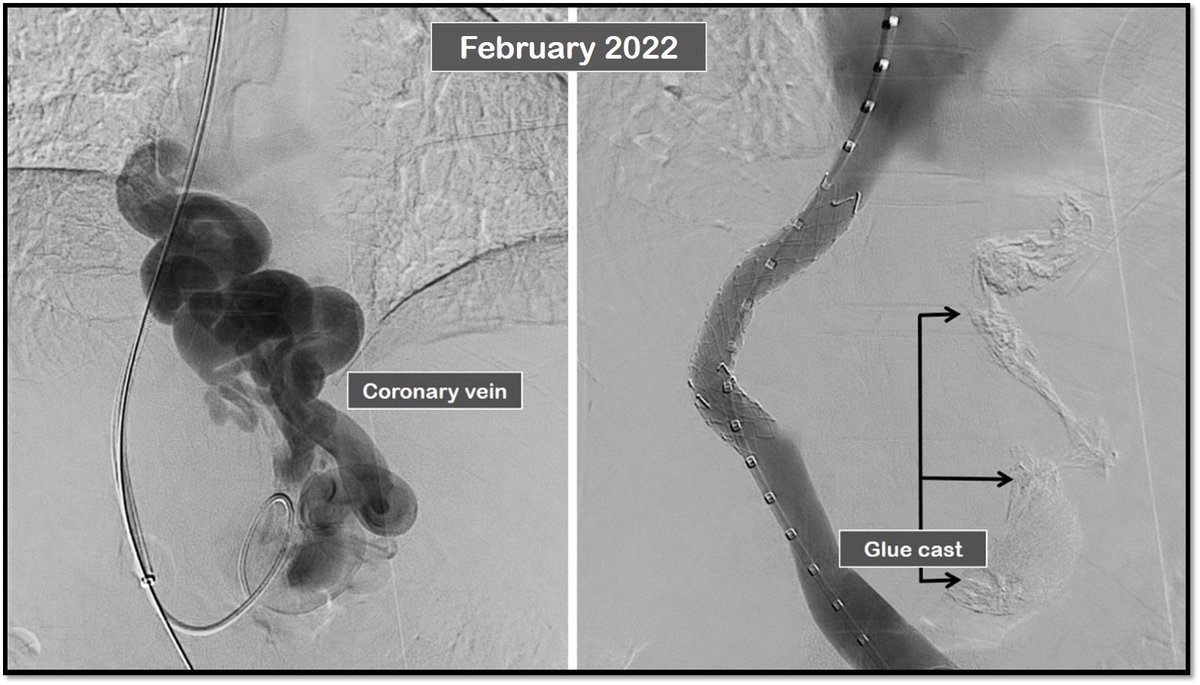
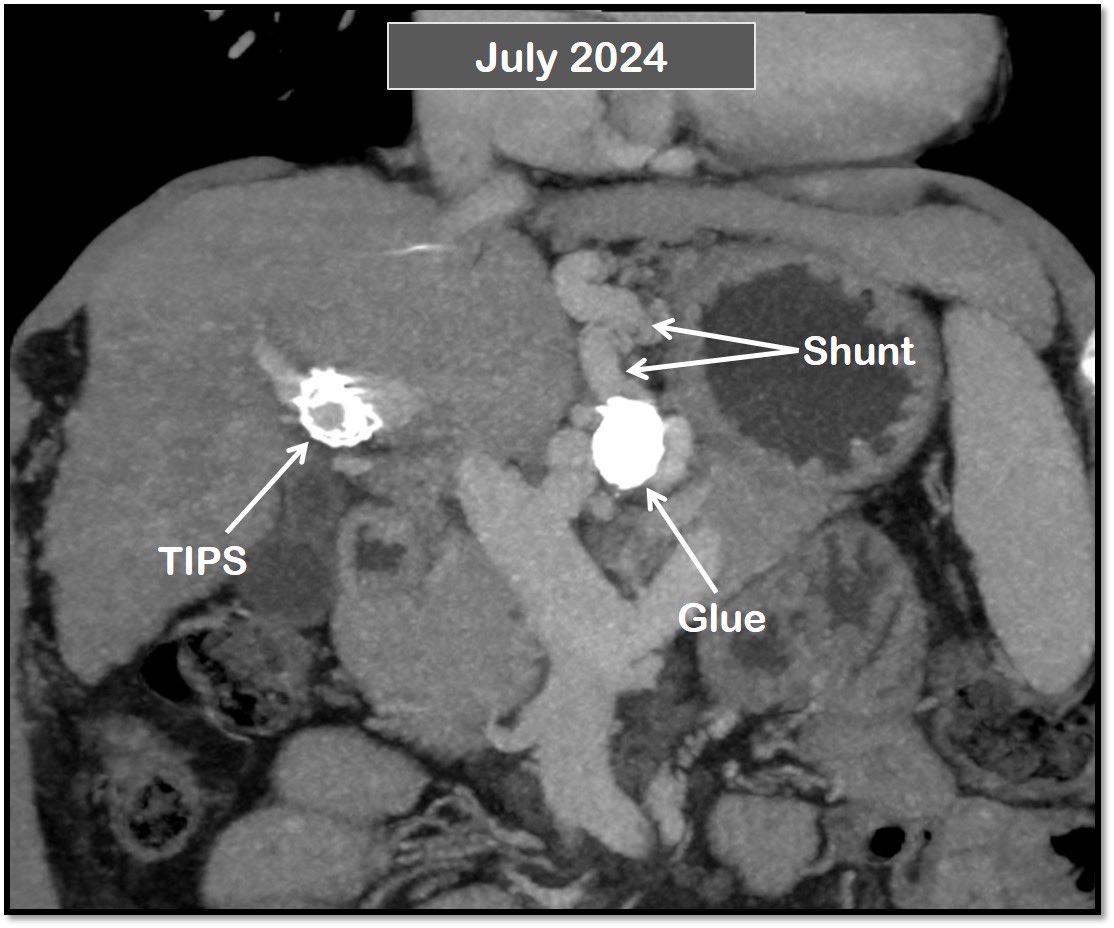
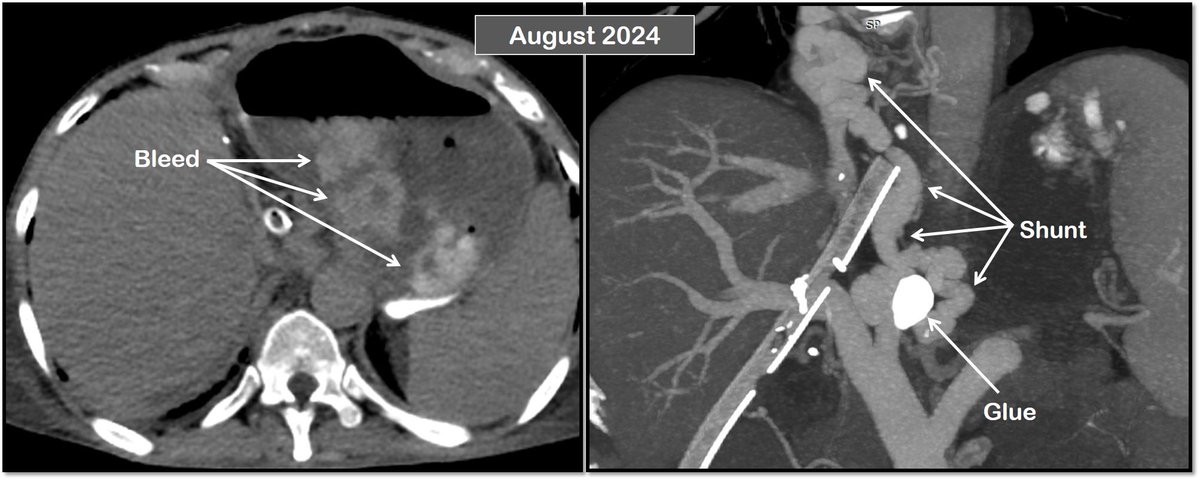
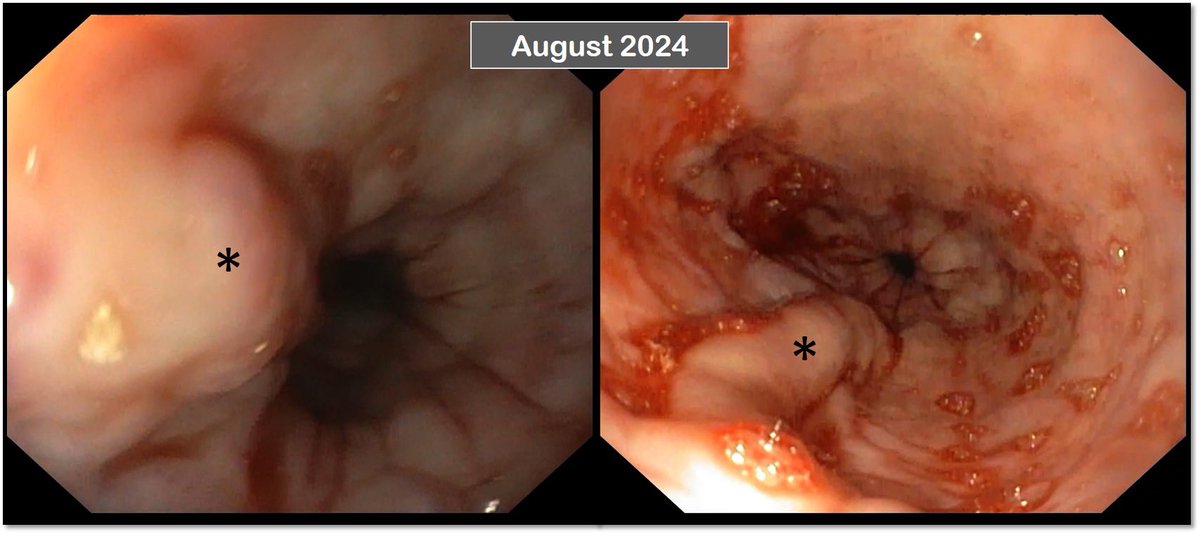
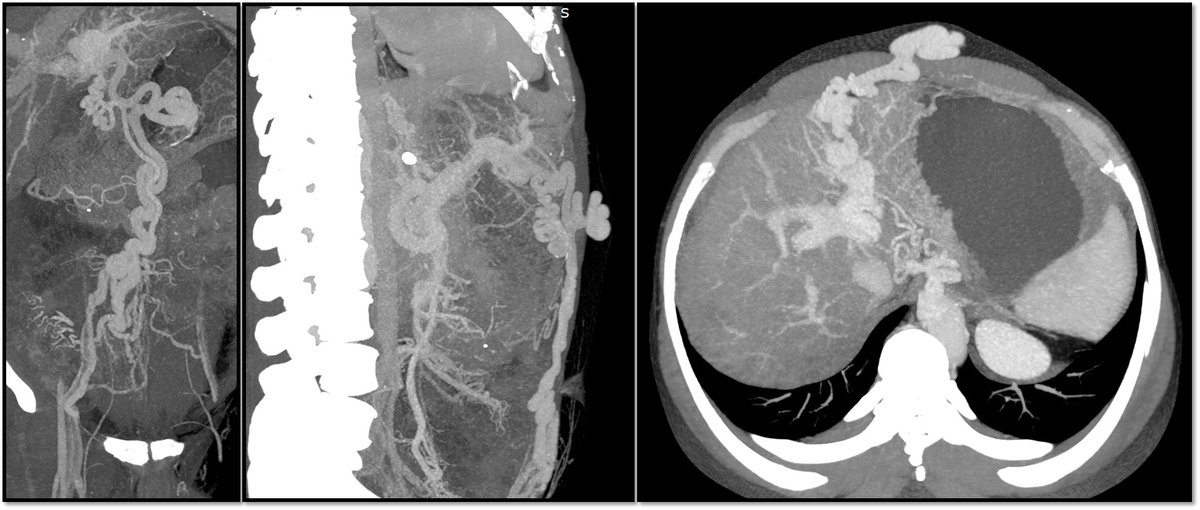
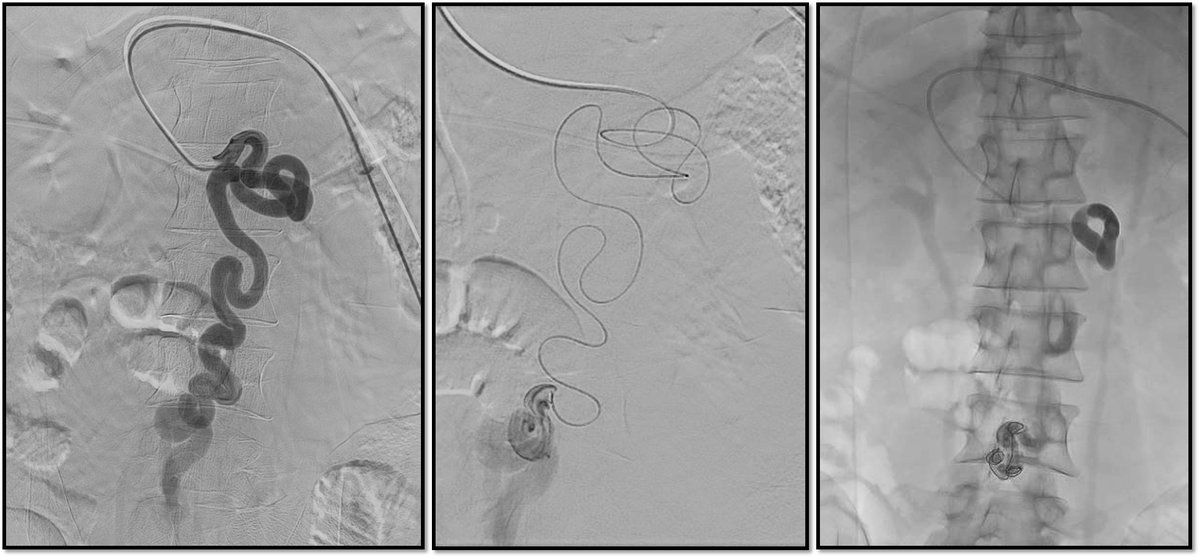
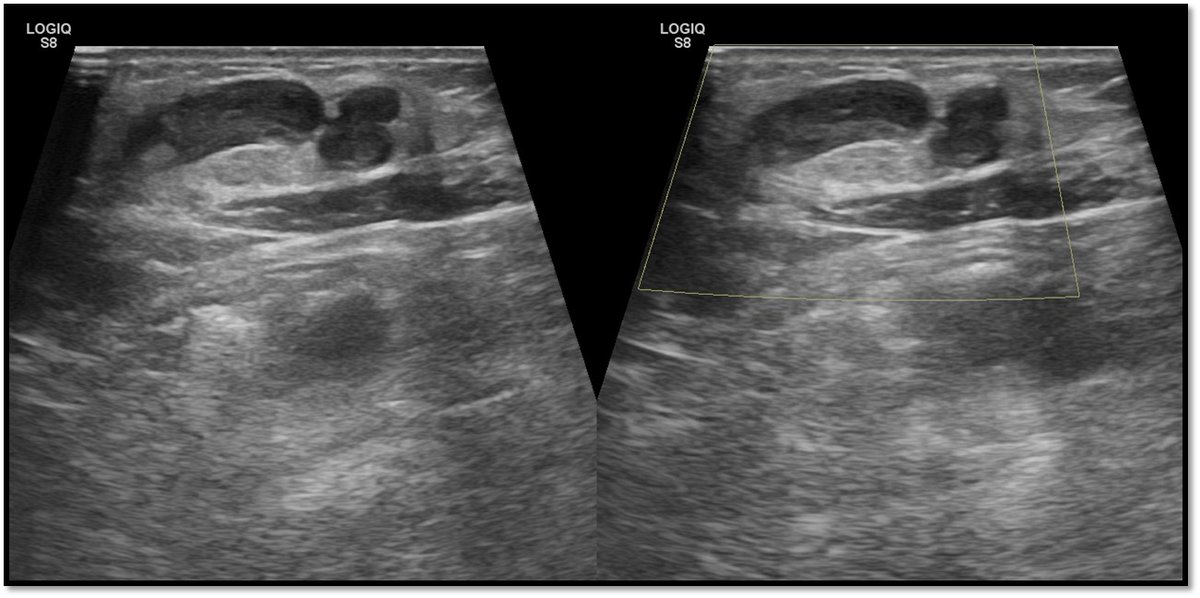
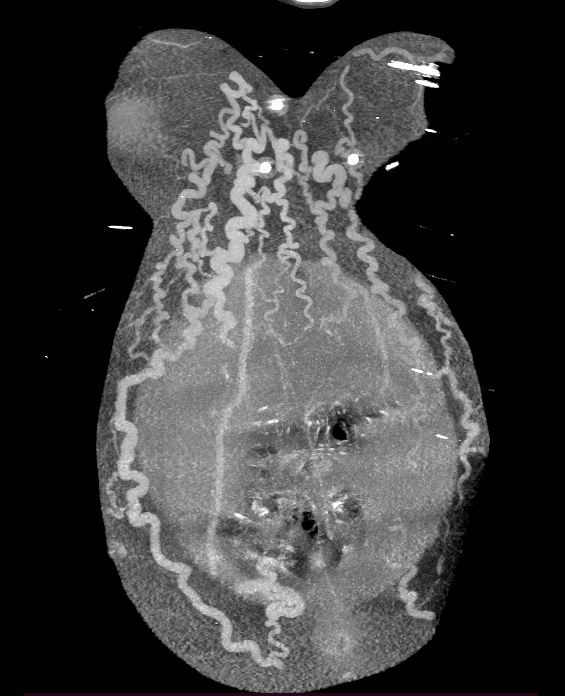
Persistence of portosystemic shunt and varices post TIPS and transplant with post LT bleed. 57y/M, CLD, recurrent bleed. TIPS - 2022. Coronary vein blocked with TIPS. 2024 - HCC. Patent TIPS. Persistent coronary. Underwent LT. 6th POD - Variceal bleed. Banded. Thoughts?
6
1
30
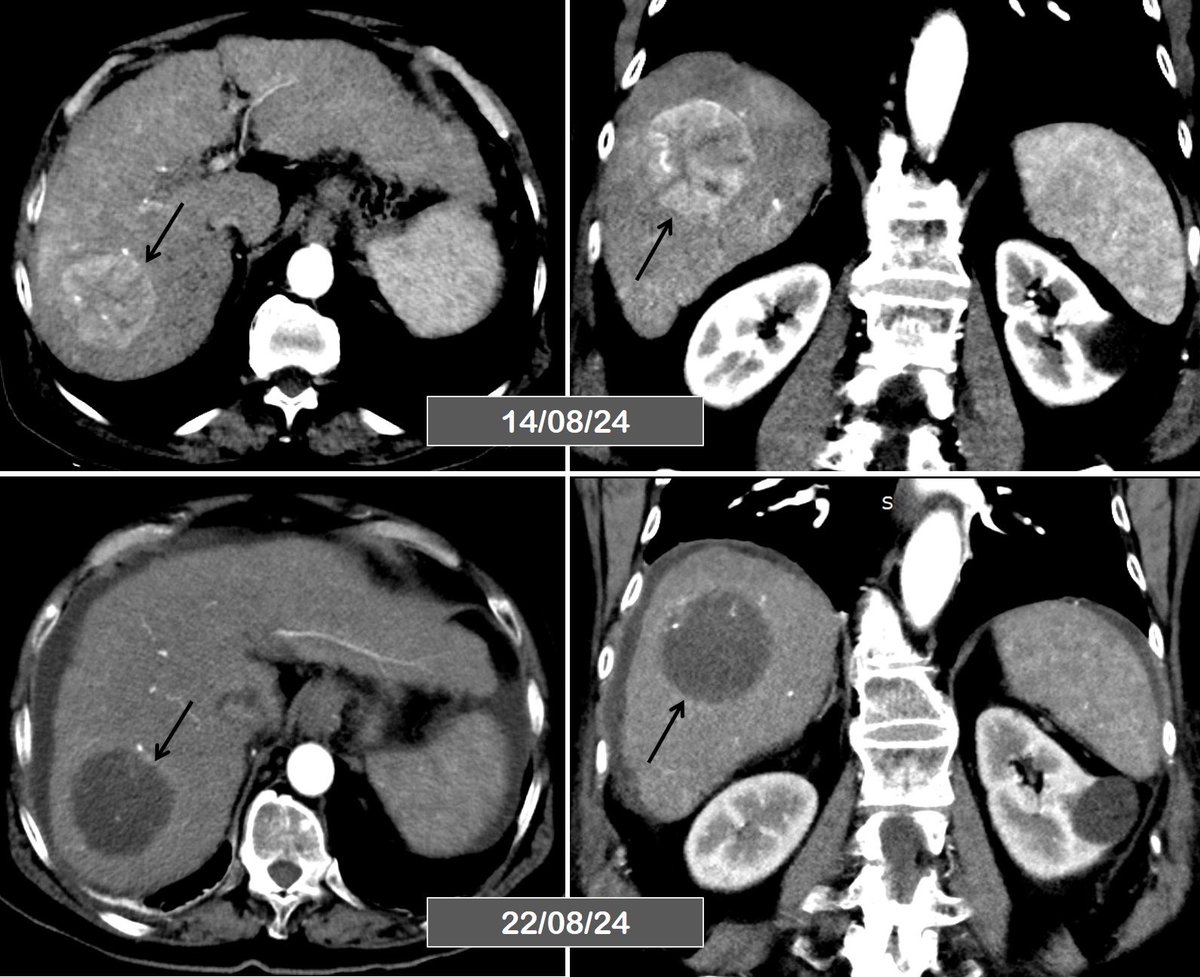
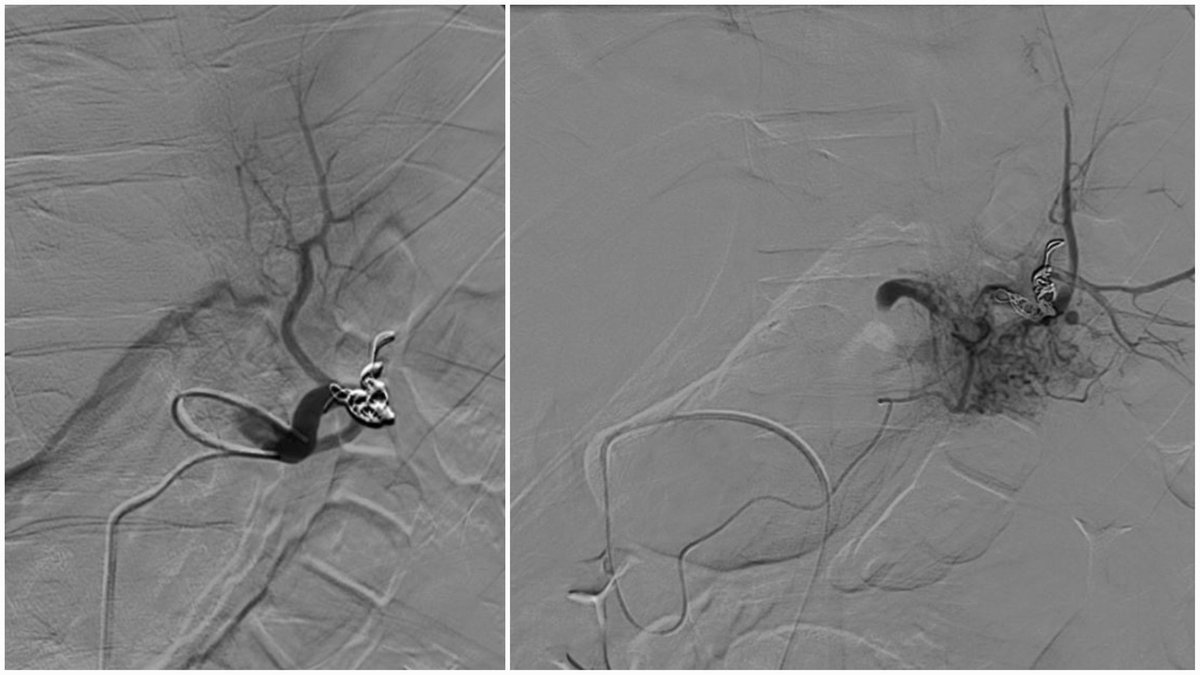
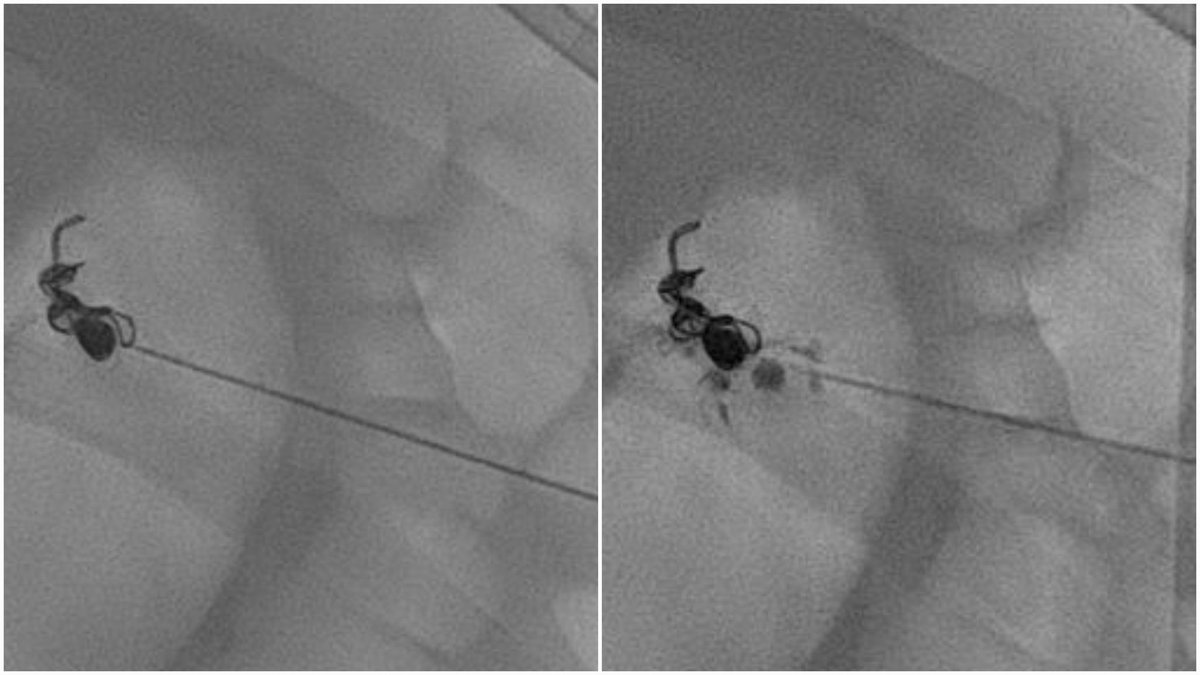
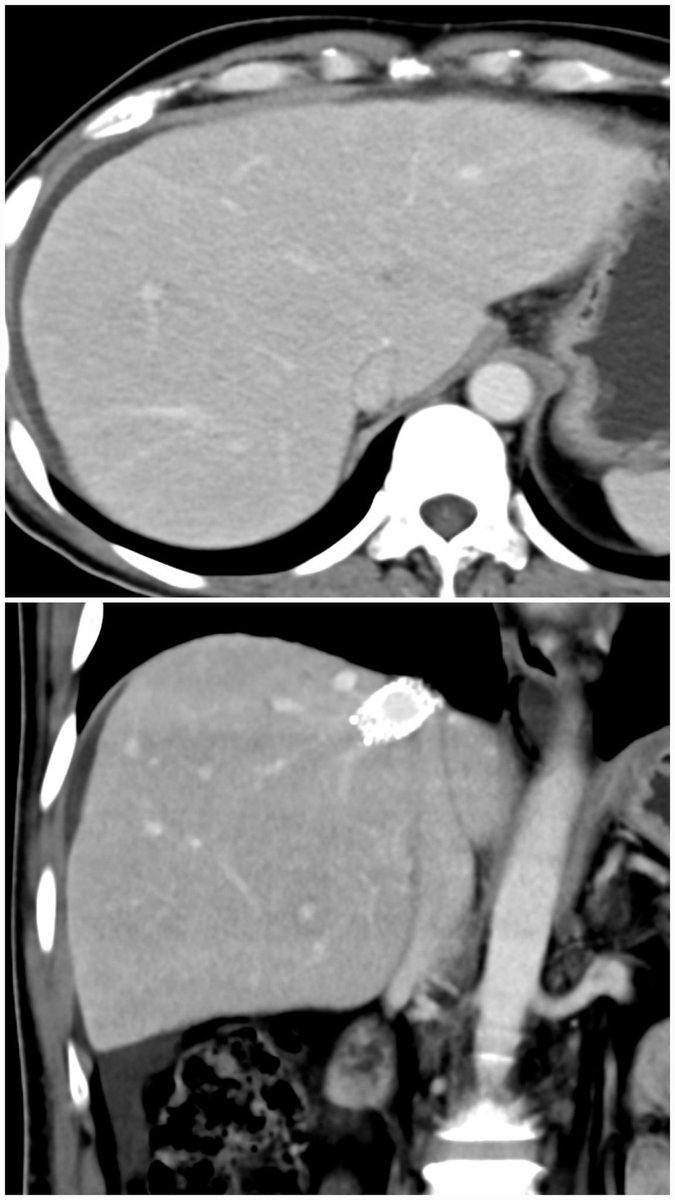
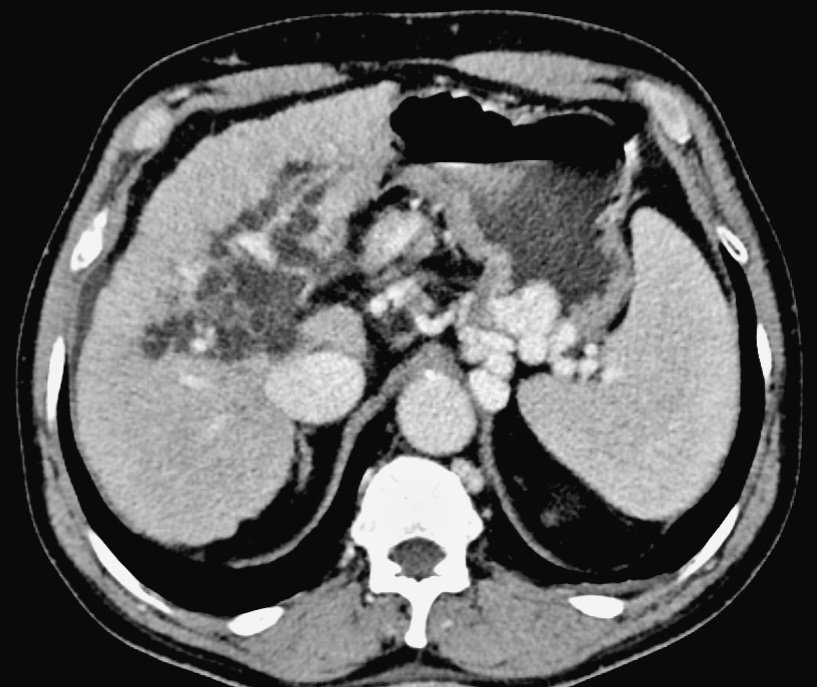
Spontaneous necrosis of HCC. 76y/M, Solitary HCC, planned for TACE. Presented with fatigue and abdominal discomfort 2 days prior to scheduled procedure. Bilirubin ⬆️ from 1.2 to 11, ALP & GGT raised. Imaging repeated to rule out any obstructive biliary pathology. @theliverdr
3
3
27
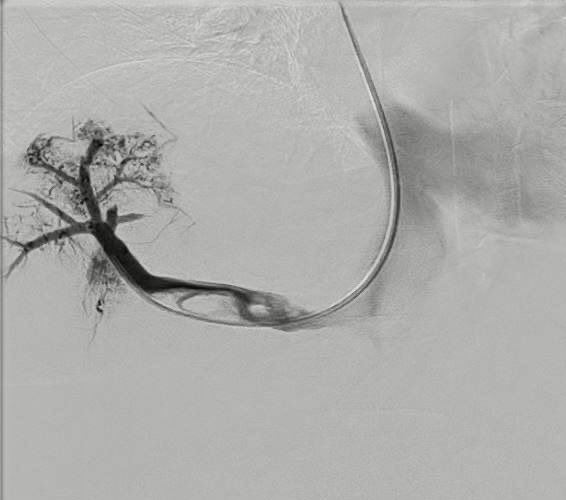
40y/F, Polycythemia, BCS. High SAAG, low protein ascites. Bilirubin 3.1. All hepatic veins thrombosed. Segment 7 vein partly patent (angio below). WWYD?. 1. Anticoagulation.2. HV thrombolysis/stenting.3. TIPS/DIPS.4. Liver Transplant.5. Need more info/investigations (specify)

11
5
24
Thrilled to announce the launch of our fellowship program in Hepatobiliary Interventional Radiology at the Center of Excellence in GI Sciences at Rajagiri Hospital, Kochi, Kerala. More details in the poster below.
5
6
44
PVR-TIPS for refractory ascites. 71 y/F, NASH-cirrhosis. On weekly LVP. CT - Thrombosed main portal vein and its right and left branches. Ultrasound guided transjugular puncture of the thrombosed right portal vein done for TIPS. With @shobhit_IR, @akhilbaby55, @theliverdr
0
3
25
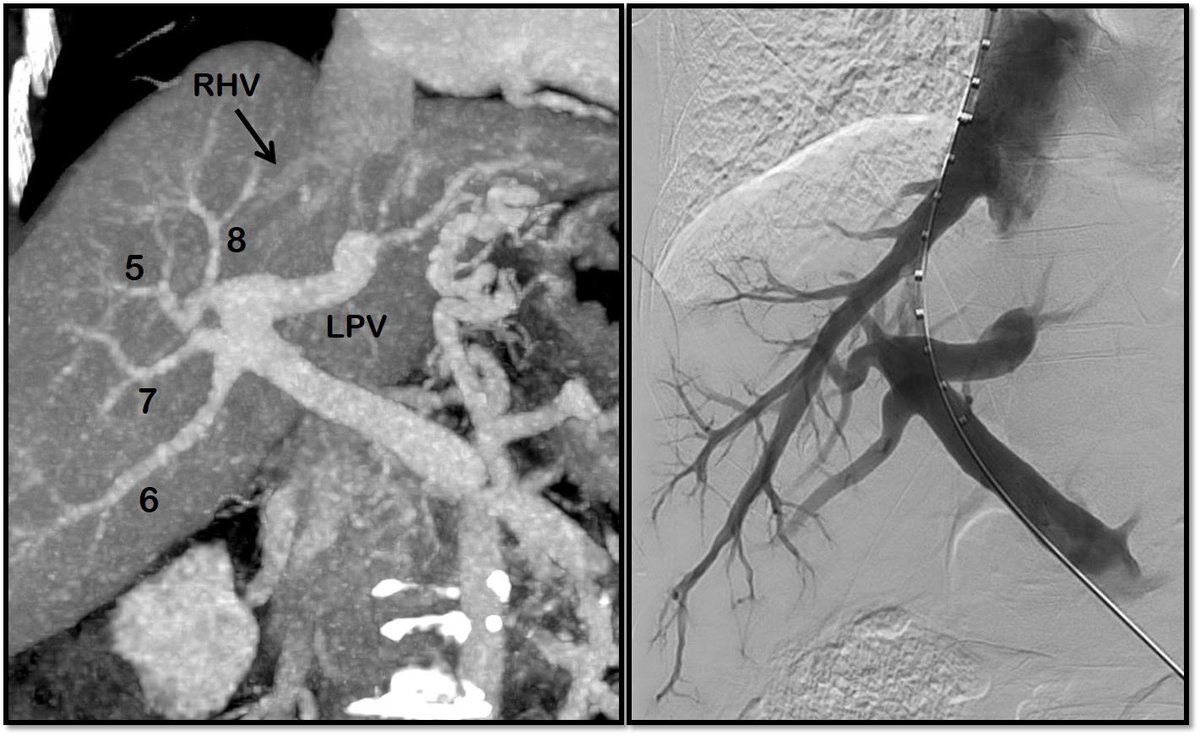
Right-to-left TIPS in variant portal venous anatomy. Nakamura type D. No suitable angle from RHV to any of the RPV branches. At the risk of going extrahepatic, single-wall puncture of meandering LPV trunk done under USG guidance. With @shobhit_IR, @akhilbaby55, @theliverdr

1
6
30
‘Vampire bite’ jugular access for occluding dual efferents of lienorenal shunt. 62 year old gentleman with recurrent severe hepatic encephalopathy. With @shobhit_IR, @akhilbaby55 and @theliverdr


2
5
33
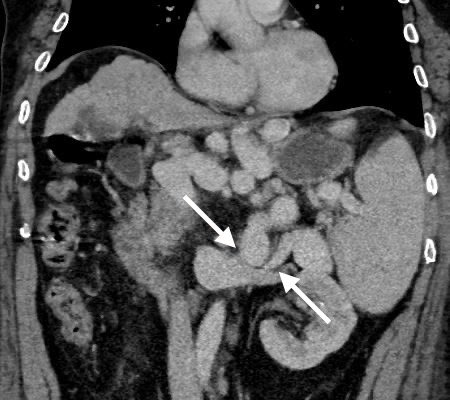
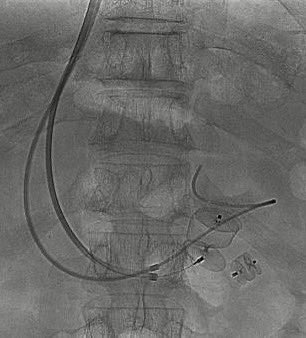
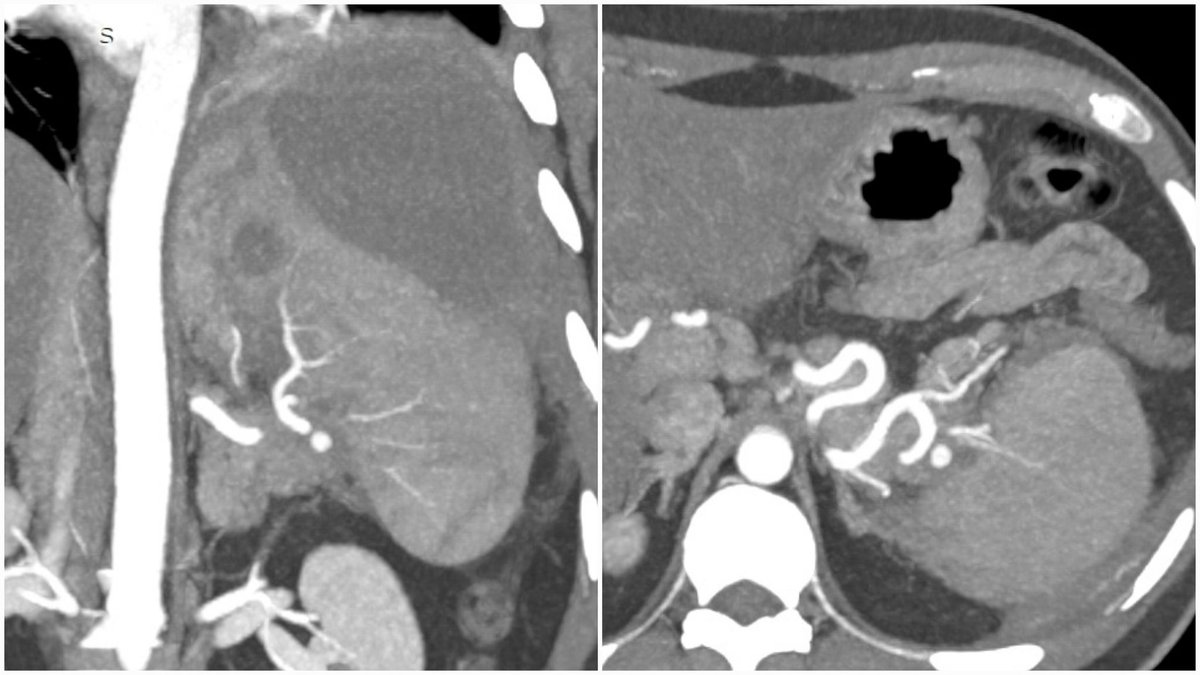
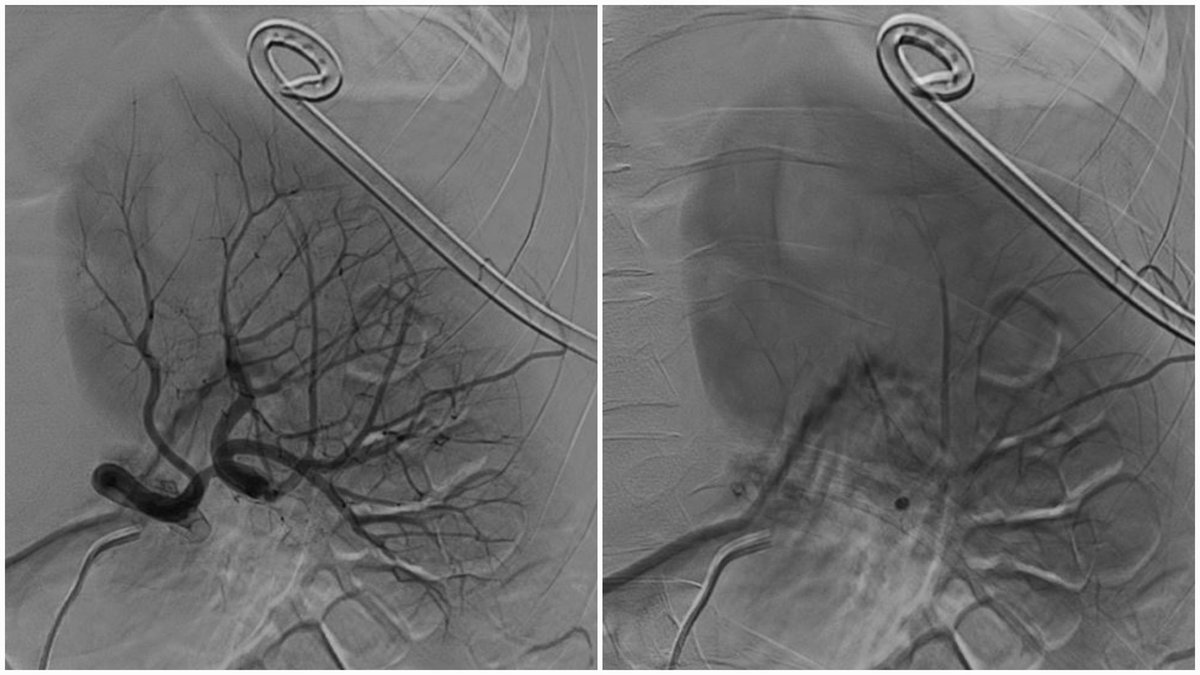
Subcapsular splenic hematoma ⬅️ pseudoaneurysm ⬅️ pancreatitis. Drainage f/b front and back door coil embolisation of parent artery. PSA starts filling from gastroepiploic artery🤯. Percutaneous trans-splenic glue embolisation to the rescue. With @shobhit_IR and @akhilbaby55
0
6
36
Hepatic vein stenting for Budd Chiari syndrome. 44y/M with ascites. Normalisation of hepatic enhancement merely 2 days after stenting. Middle and left hepatic veins start draining through collaterals into the stent. Ascites ⬇️. With @shobhit_IR, @akhilbaby55 and @theliverdr


3
12
98
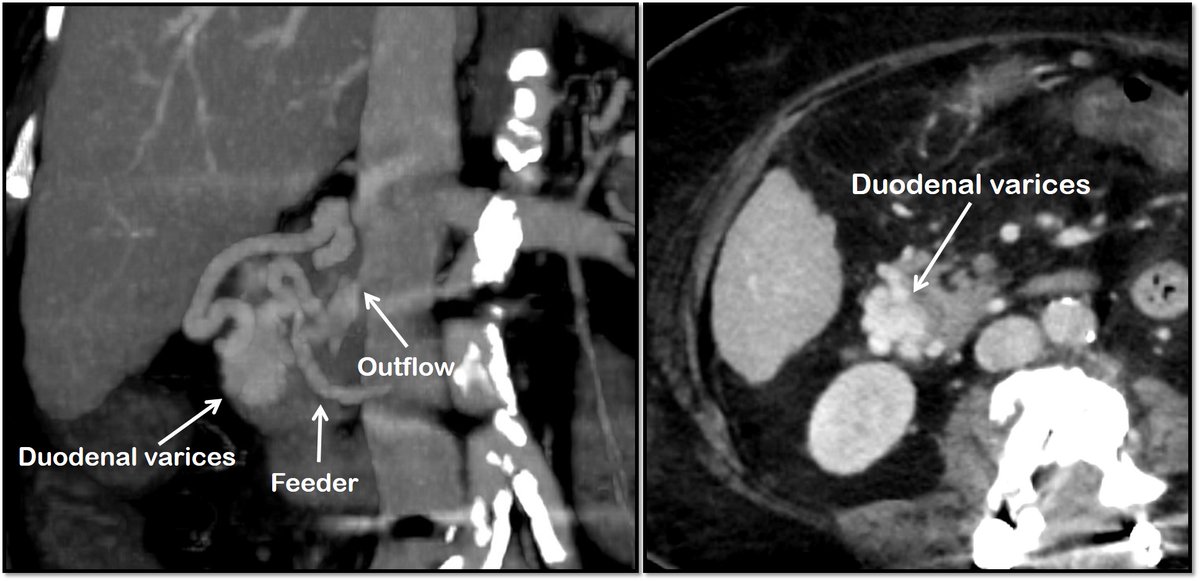
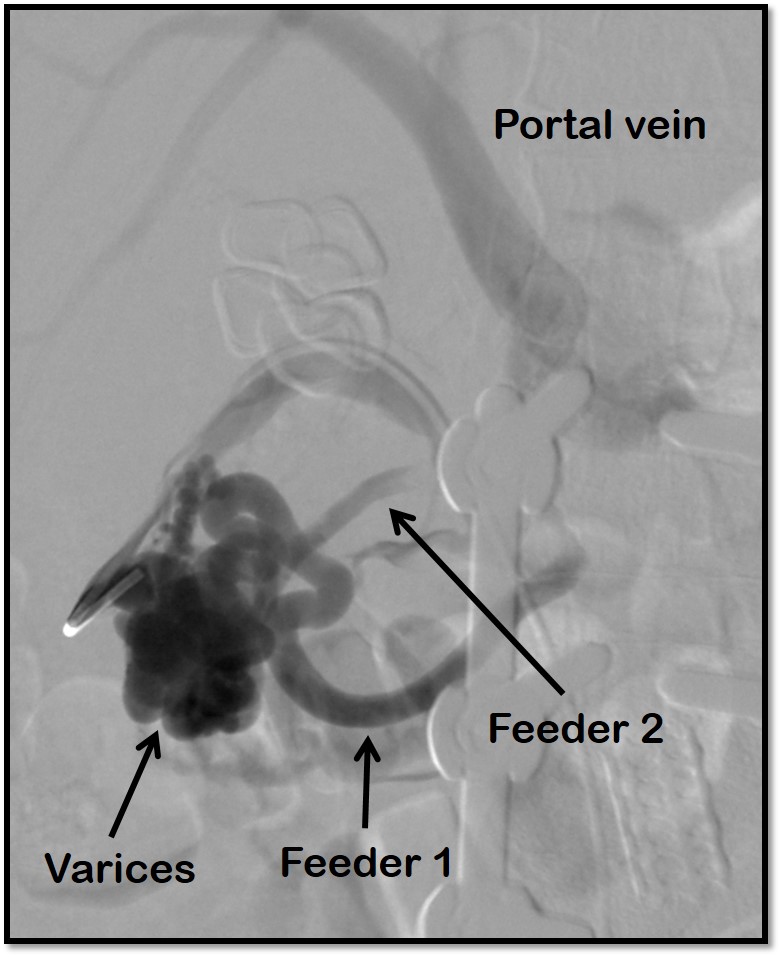
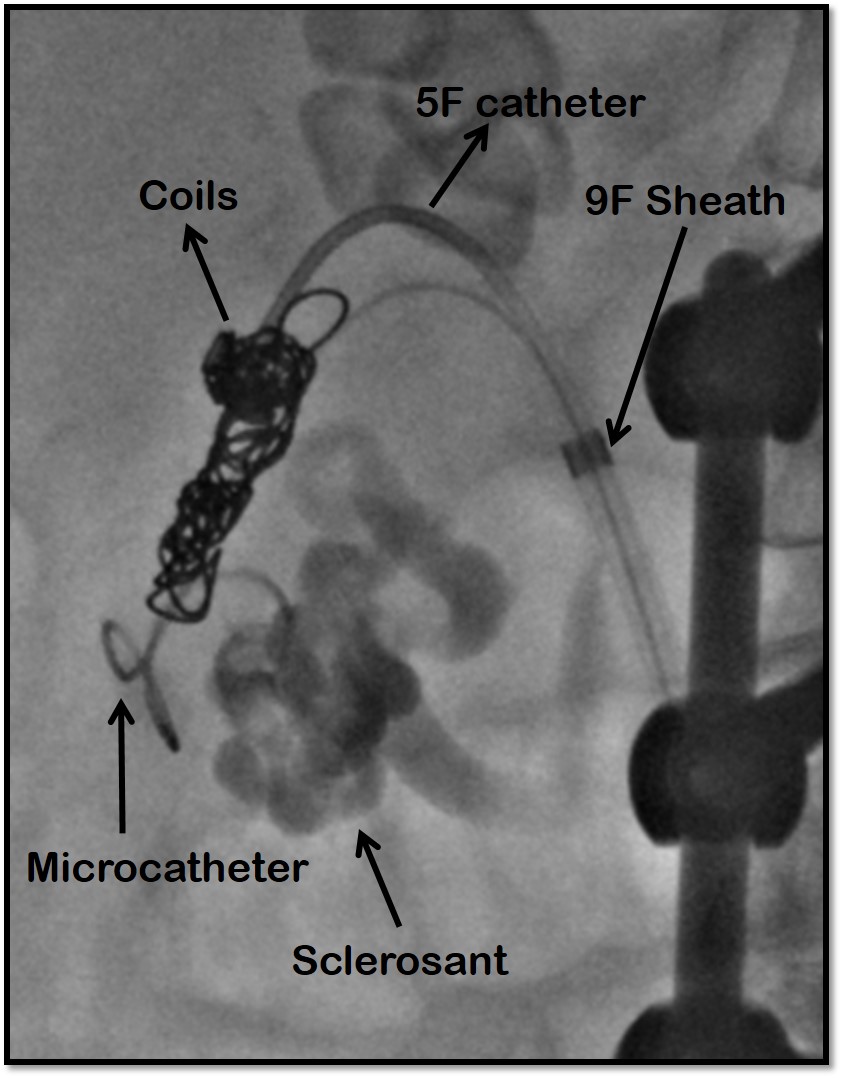
CARTO for ectopic variceal bleeding. 70y/F, Cirrhosis, Upper GI bleeding. Imaging - Dual afferents from superior mesenteric vein feeding duodenal varices with a single outflow into IVC. Coil-assisted retrograde occlusion of shunt and varices. With @SudheerPargewar
3
7
48
Transabdominal USG-guided left to left TIPS - step by step guide. Cannulate LHV ➡️ Insert RUPS over wire ➡️ USG probe in midsagittal plane in epigastrium ➡️ rotate stiffening cannula to bring it in the same plane as USG probe ➡️ PV puncture ➡️ stenting. With @SudheerPargewar


6
24
82
RT @ISVIRJUNIORWING: "🔍 Ready to delve into the latest insights on IR management of portal hypertension? Join us at the upcoming ISVIR mast….
0
3
0
Consent ✅️. Herniated paraumbilical vein varix. 40y/M, CLD, 'epigastric hernia' containing convoluted and dilated paraumbilical vein, referred for embolisation due to increasing size and risk of inadvertent injury to the vein. With @shobhit_IR and @theliverdr

2
3
24
RT @abhishek_mamc: lot of patients requiring Interventional Radiology treatments under Ayushman Bharat are being refused as we are told tha….
0
26
0
Single session IVC plasty plus DIPS. 23y/F, chronic Budd Chiari syndrome, obliterated native hepatic veins with IVC web and thrombus. Refractory ascites. With @shobhit_IR

0
3
45
Portal vein aneurysm. 38y/F, Incidentally detected extrahepatic saccular aneurysm just proximal to the bifurcation of main portal vein. No evidence of cirrhosis or portal hypertension. No history of trauma or pancreatitis. Kept on imaging surveillance.


4
6
49
Peribiliary cysts. Often misdiagnosed as biliary dilatation, biliary-IPMN or choledochal cysts. Are usually benign incidental findings in patients with cirrhosis (often with alcohol as the etiology) and severe portal hypertension. No active intervention required in most.
2
15
76