
Ed
@Rx_Ed
Followers
43,988
Following
35
Media
2,638
Statuses
30,290
Professor, Author & Researcher - Internal Medicine, Infectious Diseases & Clinical Pharmacology
New York, NY
Joined December 2011
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
Robert Fico
• 242180 Tweets
Slovakia
• 145560 Tweets
Wicked
• 88558 Tweets
Newcastle
• 65928 Tweets
Assassin's Creed
• 58089 Tweets
Antony
• 48348 Tweets
Brighton
• 46444 Tweets
Gordon
• 43796 Tweets
Ubisoft
• 40191 Tweets
Amad
• 38175 Tweets
Yasuke
• 36425 Tweets
Stones
• 32765 Tweets
Cole Palmer
• 29629 Tweets
#MUNNEW
• 26060 Tweets
Nkunku
• 25377 Tweets
Scrap
• 24051 Tweets
$CTA
• 23169 Tweets
Cádiz
• 23151 Tweets
Mainoo
• 17847 Tweets
Nitro
• 17121 Tweets
Celta
• 12942 Tweets
Japão
• 11888 Tweets
Amrabat
• 10763 Tweets
#AtalantaJuve
• 10489 Tweets
Orioles
• 10159 Tweets
Bruno Fernandes
• 10084 Tweets


















Pinned Tweet

Medicine is a service much more than a science. Doctors need to understand social theory and human rights abuses in order to deepen their comprehension of who becomes sick and why, and of who has access to healthcare and why.
43
429
2K

Did you know insulin DECREASES the production of lung surfactant?
That is why gestational diabetes is associated with lung disease in neonates.
25
480
3K
Lung cancer = high amylase
Ovarian cancer = high amylase
Perforated esophagus = high amylase
Ectopic pregnancy = high amylase
Aspirin = high amylase
Tthiazide diuretics = high amylase
OCPs = high amylase
But most of you will only think of pancreatitis when you see high amylase.
22
541
2K
Residency is hard. In this thread, I’m not going to tell you how to make it easier, because that’s subjective.
Instead, I’ll tell you the top 10 mistakes most of you make that result in a residency experience that is even harder!
#MedEd
#ERAS
#Match2023
17
454
2K
Studying medicine makes you reach a point where you feel going to the supermarket to buy milk is like going out to a fancy event!
28
399
2K
SAFE in pregnancy:
All Penicillins
All Cephalosporins
All Carbapenems
Doxycycline
Aztreonam
Azithromycin
Nitrofurantoin
Metronidazole
Hydroxychloroquine
Sulfasalazine
TNF inhibitors
Heparin
Acyclovir
Oseltamivir
Tenofovir
Raltegravir
31
438
2K
Heparin does two things outside the clotting cascade:
-DECREASES the level of aldosterone, which causes HYPERkalemia and HYPOnatremia
-INCREASES the level of PTH, which causes HYPERcalcemia and osteoporosis
11
453
2K
Don’t call them “white nationalists” — they’re domestic terrorists.

198
368
2K
In medicine, not everything meaningful has to be useful.
For example, holding a terminal cancer patient’s hand is not useful therapeutically. But extremely meaningful personally.
Medicine is a service more than a science. See my pinned tweet.
6
277
2K
Yes, my friends, azithromycin is now the FIRST line agent for traveller’s diarrhea.
As an infectious diseases specialist, it still blows my mind to think about it. But facts are facts!
Traveller’s diarrhea
=
Give azithromycin
17
224
1K
-All diabetes patients are magnesium deficient until proven otherwise.
-All hypokalemia patients not responding to potassium supplementation are magnesium deficient until proven otherwise.
-All patients on long-term PPIs are magnesium deficient until proven otherwise.
9
273
1K
Why is bradycardia common in inferior MI?
Because of the hyperactive vagal tone which inhibits SA node.
(You get to impress me on rounds if you know that what I just described is called the Bezold-Jarisch reflex)
15
201
1K
H1 receptor blockers treat ALLERGY.
H2 receptor blockers treat HEARTBURN.
H3 receptor blockers treat NARCOLEPSY.
Pitolisant is the **ONLY** H3 receptor blocker.
**blocking ANY histamine receptor prolongs QTc**
6
273
1K
HER2+ breast cancer gets trastuzumab
ER+/PR+ breast cancer gets tamoxifen
BRCA+ breast cancer gets olaparib
4
264
1K
There are two facts the majority of medical students find absolutely shocking, it’s like I insulted them.
1. Doxycycline is SAFE in pregnancy
2. ACEi are the drugs of choice for HTN in patients with renal artery stenosis
I know what you were taught & I’m sorry they lied to you.
54
173
1K
Most of you know vitamin B12 deficiency causes megaloblastic anemia.
But not many of you know vitamin B12 deficiency causes PANCYTOPENIA.
13
133
1K
Abdominal pain that radiates to the back has TWO emergent conditions:
-Pancreatitis
-Aortic dissection
10
135
1K
In acute MI, oxygen is not just useless, but also HARMFUL.
Stop using MONA and start using CAST:
-Clopidogrel
-Aspirin
-Statin
-tPA
Really depressing to see books and question banks still use the horrible MONA till this day. You are harming patients!
0
239
1K
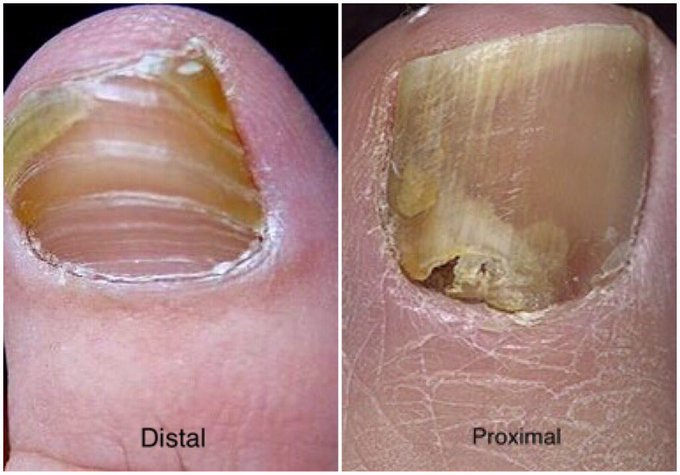
The most common type of onychomycosis is DISTAL.
Persons with PROXIMAL onychomycosis are immunocompromised until proven otherwise.
7
179
1K

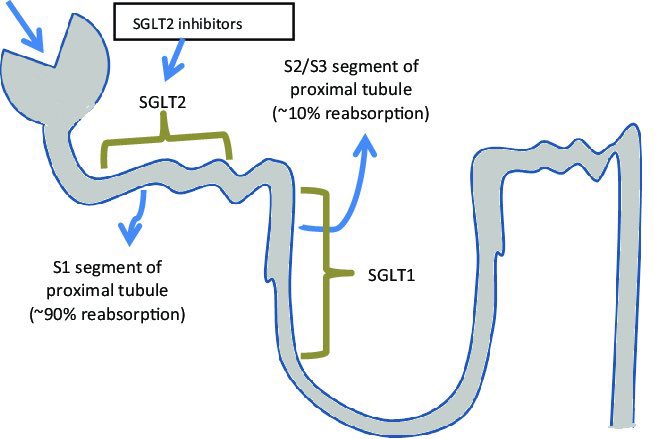
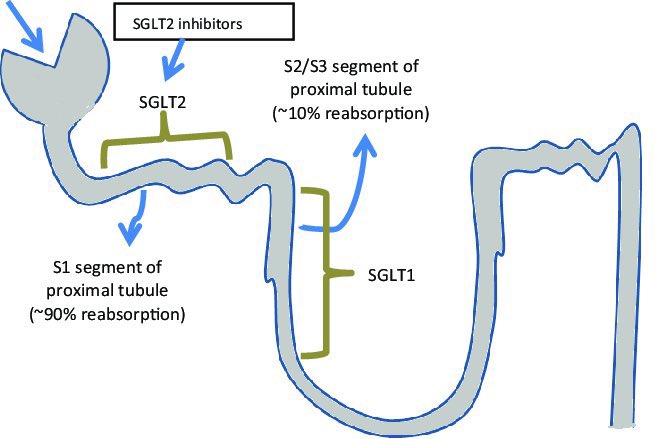
Pay attention to this thread:
Sodium/Glucose Cotransporter *2* (SGLT2) receptors are in the *1st* part of the proximal tubule, where 90% of glucose reabsorption occurs & also where SGLT2 inhibitors like empagliflozin work.
SGLT *1* receptors are in the *2nd* part of the tubule.
6
252
950
While we protest and get arrested here in New York fighting for the lives of the innocent civilians killed and kidnapped in the Middle East, the “beacon” of Islam, Saudi Arabia, celebrates Halloween!
ماشاء الله 🤡
0
452
892
1st line Tx for PCOS:
-Metabolic dysfunction: metformin
-Infertility: clomiphene
-Hirsutism: spironolactone
-Menstrual irregularity: OCP
19
216
914
H. pylori doesn’t cause GERD. So why do we use PPIs to treat the infection? Shouldn’t Abx be enough?
Raising the pH with PPIs does TWO things:
-Increases bioavailability of Abx by increasing its ionization potential
-Decreases bacterial transcription of the neutralizing urease
14
142
886
-Mitral stenosis
-Mechanical valve
-Antiphospholipid syndrome
These are the only three indications for warfarin in contemporary medicine. For everything else, we have DOACs.
20
167
871
The most common physical finding in Sjögren syndrome is JOINT PAIN!
The most common WRONG answer is dry mouth.
14
90
862
Vitamin B12 deficiency can cause ALL sorts of neurological complications.
The MOST common is peripheral neuropathy and the LEAST common is dementia.
2
122
828
The two most common drugs associated with vitamin B12 deficiency are...?
Metformin and PPIs!
6
129
811
TIA:
Use aspirin + clopidogrel for 21 days
OR
Use aspirin + ticagrelor for 21 days
Then discontinue clopidogrel or ticagrelor and continue aspirin ALONE indefinitely
12
151
800
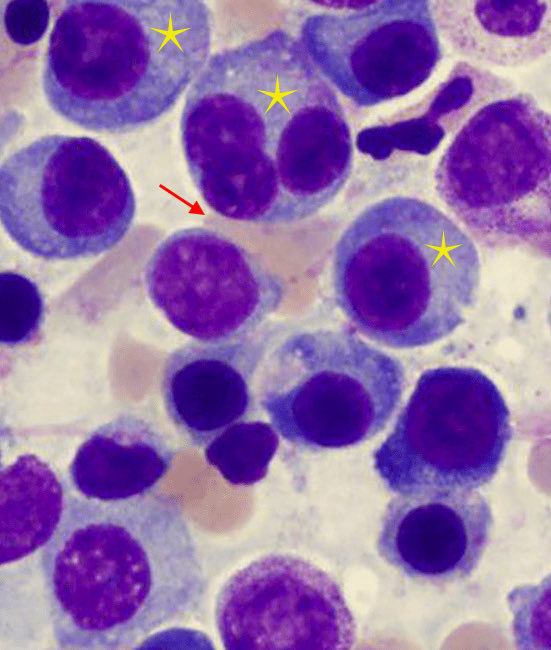
What is the mechanism of anemia in multiple myeloma?
-The HUGE plasma cells SQUEEZE the RBCs (red arrow)
-The dysfunctional Golgi apparatus inside the cell (yellow star) makes the cell produce faulty immunoglobulins (will not fight infection but will clog-up the kidney instead)
9
169
783
Propofol has NO analgesic effect
Etomidate has NO analgesic effect
Thiopental has NO analgesic effect
8
109
777

This is super important:
Unexplained microcytic anemia in a person 45-years or older is colon cancer until proven otherwise.
7
148
760
B-cells are produced with IgM & IgD as default antibodies
If B-cell receives IL4, it switches to IgG1 & IgE
If it receives IL5, it switches to IgA
If it receives TGFß, it switches to IgG2 & IgA
If it receives INFγ, it switches to IgG3
If it receives BAFF, it switches to IgG4
1
156
750
Regardless of age, postcoital bleeding is cervical cancer until proven otherwise.
1
106
741
A quick review of SGLT2 inhibitors in a mini-thread:
Sodium/Glucose Cotransporter *2* (SGLT2) receptors are in the *1st* part of the proximal tubule, where 90% of glucose reabsorption occurs & also where SGLT2 inhibitors like empagliflozin work.
SGLT *1* receptors are in the
1
203
746
Oral ulcers are PAINFUL in:
-Behçets
-Sjögrens
-Herpes
Oral ulcers are PAINLESS in:
-SLE
-IBD
-Reactive arthritis
3
146
739
Anti-diabetes medications and cardiac protection:
-The best are SGLT2 inhibitors (eg dapagliflozin)
-Followed by GLP1 analogs (eg semaglutide)
-DPP4 inhibitors (eg linagliptin) have NO significant cardiac protection
7
178
734
GI bleeding makes your stool black.
Ferrous replacement makes your stool black.
How to differentiate?
Ferrous makes you CONSTIPATED!
8
117
713
Parkinson
+
Orthostatic hypotension
=
Shy Drager Syndrome
Parkinson
+
Ataxia
=
Olivopontocerebellar atrophy
Parkinson
+
Vertical gaze palsy
=
Supranuclear palsy
Parkinson
+
Acute Sx onset
=
Vasculitis
2
133
696
The most common infection after tattooing is staphylococcus.
Not HIV, HBV or HCV.
Also, if someone comes to clinic telling you they plan on getting a tattoo, the first thing to do is to check their TETANUS vaccine status!
3
111
686
What are the BIGGEST updates in nephrology?
-SGLT2i for CKD priegrssion & HF regardless of DM
-Finerenone (non-steroidal MRA) for CKD progression in T2DM
-Patiromer & Zirconium for hyperkalemia with ACEi/ARBs
-Tolvaptan (V2 blocker) for PCKD
We’re updating all videos & slides!
3
144
692

Insulin does not remove potassium form the body.
Insulin redistributes potassium within the body.
8
71
672
Statins are one of the most potent anti-inflammatory drugs known to man.
As a side effect, they also lower LDL.
11
95
667
Gallstone is the most common cause of ACUTE pancreatitis.
Alcohol is the most common cause of CHRONIC pancreatitis.
3
93
669
So you feel “stressed out” studying for the USMLE?
I will have to learn how to live with myself without having had the honor of having this saint in my class.
This Palestinian doctor in Gaza reached a level of nobility the rest of us can only dream about.
الله يرحمه
0
239
650
What is more dangerous than ignorant people?
Pseudo-educated people. People who THINK they know things.
11
150
654
There are 2 major advantages with bumetanide over furosemide:
-Bumetanide is 40x more potent vs frusemide
-Bumetanide diffuses passively vs furosemide needs active tubular secretion
That is why we teach our residents bumetanide is the loop diuretic of choice in the ICU setting.
3
131
654
If a drug that inhibits CYP450 is used concomitantly with another that induces CYP450, the inhibitor usually dominates.
Why?
Inhibitors act on EXISTING enzyme molecules. Inducers need time for NEW molecules to be synthesized.
It’s easier to ruin a relationship than build one!
13
124
655
For every 10-point increase in pCO2, the HCO3 will:
Rise 1 point (acutely)
Rise 3.5 points (chronically)
For every 10-point decrease in pCO2, the HCO3 will:
Drop 2 points (acutely)
Drop 5 points (chronically)
2
162
642
-Doxycycline is SAFE in pregnancy
-ACEi are the drugs of choice for HTN in patients with bilateral renal artery stenosis
(I know what you were taught and I am sorry they lied to you)
0
110
647
Aspirin for MI patients is time dependent (the faster you give aspirin, the lower the mortality)
Beta blockers and statins are not time dependent (as long as they’re given at any point before discharge, it’s OK)
Remember - NO oxygen at all unless the patient hypoxic!
6
153
631
One of the “quick and dirty" tricks I teach the residents — to correlate the urine osmolarity with specific gravity, multiply the last 2 digits by 30.
e.g. if the specific gravity is 1.010, the urine osmolarity is 300
1.020; 600
1.040; 1,200
and so on...
7
138
628
Drug-induced hearing loss:
IRREVERSIBLE:
-Aminoglycosides
-Chemotherapy
-Loop diuretics
REVERSIBLE/partially reversible:
-Aspirin
-NSAIDs
-PDE5i
-Anti-malarial
The risk depends on:
-Dose
-Tx duration
-Infusion rate
-Clearance rate
-Concomitant use
6
169
619
What EXACTLY is tumor lysis syndrome (TLS)?
Malignancy PLUS at least 2 of the following:
- K > 6 mEq
- UA >8 mg/dL
- Ca > 7 mg/dL
- PO4 > 4.5 md/dL
(TLS can happen after chemotherapy *OR* radiation therapy)
10
133
617
Why is hypercalcemia associated with nephrogenic diabetes insipidus?
Because excess calcium DECREASES the affinity of ADH to V2 receptors.
5
91
613
Placebo:
-Glucosamine
-Omega-3
-Fish oil
-Collagen
-Probiotics
-Hyaluronic acid
-Vitamin E
18
95
597
Normal adrenals make 80% epinephrine and 20% norepinephrine.
In pheochromocytoma, the ratio is FLIPPED (20% epinephrine and 80% norepinephrine).
That is why we don’t see vasodilation in pheochromocytoma (norepinephrine does NOT stimulate ß2 receptors).
4
109
599
Why PPIs in upper GI bleeds?
PPIs stabilize blood clots over ulcer formation and CLEARS visualization of the lesion with endoscopy.
We don't wait for endoscopy to start PPIs. We start STAT!
0
123
600
Stop saying smoking is “protective” against UC. That is just STUPID!
The right link is this: if UC patient (previously well controlled with drugs) presents to clinic with flare up, the question you should ask is “Did you recently quit smoking?”
BIG DIFFERENCE!
5
92
585
The most common cause of toxic shock syndrome is staphylococcus. The most common WRONG answer is tampons (stop blaming women for everything).
TSS is treated with vancomycin + clindamycin
Why?
Vancomycin KILLS the bacteria.
Clindamycin stops the RELEASE of toxin.
3
105
587
Ed’s “rule of 5” of antibiotic duration:
COPD exacerbation: 5-days, no more
Bronchitis: 5-days, no more
Cellulitis: 5-days, no more
Cystitis: 5-days of nitrofurantoin, no more
Pyelonephritis: 5-days of fluoroquinolone, no more
CAP: 5-days, no LESS
7
156
585
One of our IMG residents just told me her younger sister is an ER intern in Egypt and has not gotten paid in months! al-SiSi should stop building new malls and highways and start paying his doctors! There’s a PANDEMIC!
Did you know Egyptians eat pigeons? They stuff it with rice!
15
52
575
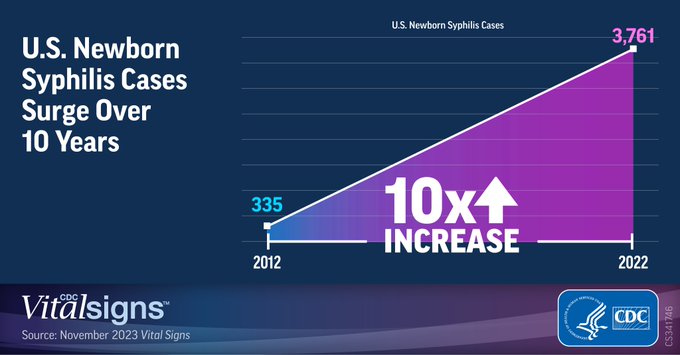
America ran out of benzathine penicillin to treat syphilis during pregnancy. Meanwhile, the rate of congenital syphilis cases increased by a stunning 203%!
We now have to borrow penicillin from France. But hey, let's spend $10 million/day to fund foreign governments instead!

0
205
572
Plasmodium!
Falciparum:
-Most common
-Most deadly
-Mainly in Africa
-NO liver reservoir
-Chloroquine resistant
-High parasitemia because it infects RBCs
Vivax:
-Less common
-Has liver reservoir
-Mainly in Asia/South America
-Low parasitemia because it infects RETICULOCYTES
4
134
578
Class 1 antiarrhythmics often causes confusion among students and I finally understood why. It’s because most of you don’t think of the STATE of the Na channels.
Na channels can exist in 3 states:
-Active
-Inactive
-Resting
1/3
2
126
573
β-Thalassemia can cause iron overload even in the absence of transfusion therapy.
Yes? No?
60
54
576
The FASTEST way to raise the platelets in acute ITP is…
IVIG!
The most common WRONG answer is steroids.
10
67
565
t(15:17) = AML
t(9:22) = CML
t(11:14) = Multiple myeloma
t(8:14) = B-cell lymphoma
t(14:18) = Follicular lymphoma
3
111
561
Did you know abdominal pain can be the ONLY physical finding of diabetic ketoacidosis?
12
49
546
Rhabdomyolysis CAUSES high phosphate
LOW phosphate CAUSES rhabdomyolysis
Rhabdomyolysis CAUSES hyperkalemia
Hypokalemia CAUSES rhabdomyolysis
2
108
552
In Parkinson disease, anosmia can be the FIRST symptom and may precede the rigidity and resting tremor by years!
3
92
535
TIA:
-Start aspirin PLUS clopidogrel for 21 days
-Then discontinue clopidogrel BUT continue aspirin indefinitely
0
95
544
The owner of this account is no longer with us. Dr. Alrayyes was killed last night in Gaza. We, forever, lost his contribution to medicine and patient care. Where is the rage?
Doctors without humanity are PR agents.


0
236
531
Prescribing an ACEi concomitantly with an ARB is like wearing two bras on top of each other.
Wrong!
13
78
529
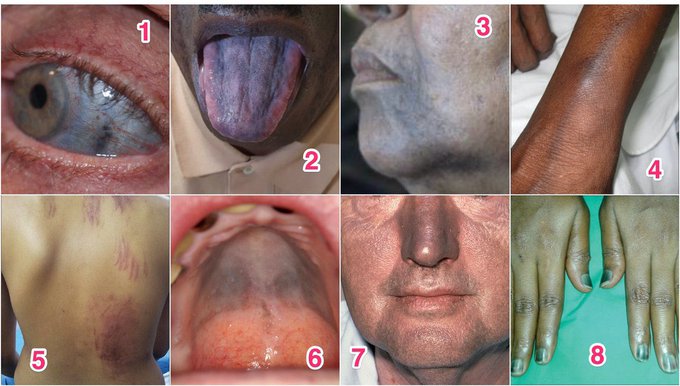
Most common drugs that cause skin hyperpigmentation:
1. Scleral -Minocycline
2. Tongue -Hydroxyurea
3. Perioral -Chloroquine
4. Vein used for IV -5FU
5. Flagellate -Bleomycin
6. Intraoral -Imatinib
7. Photodistribution -Amiodarone
8. Nails -Vincristine
3
128
522
Medicine is a TEAM service. Never trust a doctor who claims to know it all!
The more you know, the more you’ll realize that there is a lot that you don’t know. That’s the key to saving lives.
4
192
532
The most common cause of osteoporosis is HORMONE deficiency (estrogen deficiency in females and testosterone deficiency in males).
The most common WRONG answer is calcium/vitamin D deficiency.
3
71
513
Metronidazole does NOT inhibit acetaldehyde dehydrogenase in any clinically significant manner.
Avoiding alcohol while taking metronidazole to prevent “disulfiram-like reaction” is simply inaccurate.
40
80
513
There are 3 NEW things you should know about asthma:
*LONG* acting ß-agonists plus inhaled steroids are now used as RESCUE Tx
Leukotriene inhibitors like montelukast have been UPGRADED and are now used EARLY in Tx
*LONG* acting muscarinic antagonists play a role in asthma Tx
9
138
509
Ipratropium is an ACUTE management drug.
Ipratropium has NO utility in chronic management of asthma or COPD.
5
64
511
More urine output with diuretics does NOT mean renal failure is reversing.
You can’t FORCE love and call it “true” love!
4
105
510
Aminoglycoside associated nephrotoxicity is usually reversible.
Aminoglycoside associated ototoxicity is not.
3
53
499
