
The Protected Airway Collaborative
@ProtectedAirway
Followers
3K
Following
613
Media
337
Statuses
730
Where Airway Mastery Gets Made #nextgen I #airwaytraining I #realworld I #JointhePAC
New York, NY
Joined February 2019
Excited to announce our new education hub. Airway Works // NYC. Starting September 1st. Immersive, interactive, hands-on. See where airway mastery gets made.

theprotectedairway.com
Discover Airway Works in NYC, your hub for hands-on airway training. Elevate your skills with immersive programs tailored for all levels.
0
3
4
Should we be using ultrasound to identify the CTM during eFONA? Not so fast.
theprotectedairway.com
Explore why tactile skills are crucial in emergency cricothyroidotomy, emphasizing simplicity and real-world application over ultrasound technology.
0
10
19
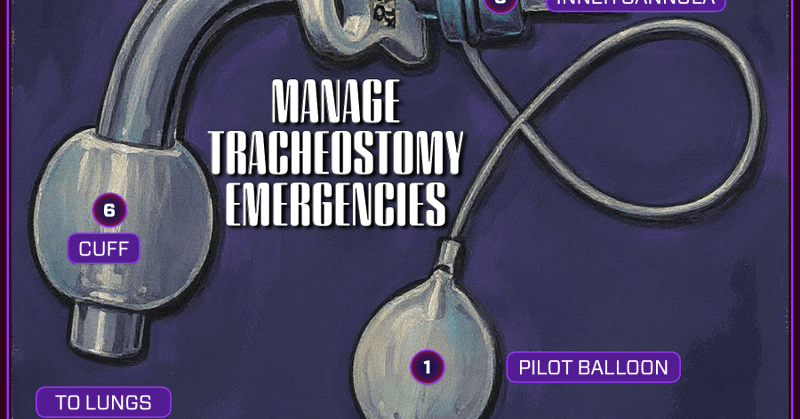
Trachesotomy Tube Key Features: What Every Provider Must Know.
0
2
9
A great topic. From the airway management perspective, these patients rarely require intubation. NIPPV is usually sufficient (even when they look peri-tube). If you do intubate, TURN OFF the Nitro! Or you will end up with a pt in arrest.

🫁 Crashing SCAPE? High-dose nitro works fast. 💉 Bolus hard (up to 2mg IV).💨 Add BiPAP.🕒 Peak in 5 min.⚠️ Taper when SBP <140 or MAP <65.Infographic via @REBEL__EM 🔥.@marco_propersi @emswami @srrezaie @mramzydo.❤️ Like 🔁 Repost 🔔 Follow.#FOAMed

0
2
7
Tracheostomy emergencies are high-risk, high-consequence. You need a plan before you're at the bedside facing one. #trach #tracheostomy #emergencymedicine #criticalcare #ems #anesthesiology
theprotectedairway.com
Master tracheostomy emergency management with actionable strategies for clinicians. Build confidence and save lives today!
0
10
18
Big shoutout to Dr Luca Uenlue, Dr Christian Hohenstein, and their entire faculty team. PAC Germany — you crushed it!

theprotectedairway.com
Celebrate our German team's creativity and collaboration at the PAC course, where innovation meets airway education. Discover more!
0
3
9
More data that addressing abnormal physiology in the peri-intubation period is essential.
theprotectedairway.com
Review of the BARCO study: a large, prospective airway registry from Brazil showing that major adverse events during emergency intubation occur in 1 in 3 patients and are strongly linked to 28-day...
1
6
10

New evidence that PEEP + PreOX is a highly effective combination.
theprotectedairway.com
Explore the latest evidence on preoxygenation from Roveri et al. (2025). This crossover RCT compares NRB, BVM, and BVM + PEEP across adults and children, showing PEEP improves oxygenation and...
0
3
7
Next time you're at the head of the bed, remember: you don’t get extra credit for a second attempt - just extra risk. Insights from the BARCO Study.
0
9
25
Video or Direct. That is the question when it comes to laryngoscopy these days. Maybe we are looking at the debate from the wrong perspective. This study helps reframe the debate. Maybe its about practice over tools.

theprotectedairway.com
Explore the debate on laryngoscopy training vs. tools. Discover why practice trumps devices in effective intubation training.
0
4
6
Thanks Luca Ünlü, Chris Root & Co. for these important insights on Confined Space Airway Management (CSAM). Whether you're intubating in a difficult prehospital setting or unexpectedly in the CT scanner, this is a great read! #intubation #difficultairway

theprotectedairway.com
Explore confined space airway management (CSAM) techniques to enhance patient care in challenging environments with expert insights.
0
4
12
The future of medical education is waiting to be designed. The origin story of PAC.

0
3
6
PAC is now available in Europe with upcoming events in Germany and Austria. Check it out!

theprotectedairway.com
The Protected Airway Collaborative focuses on enhancing airway management through top-tier education and training. Recently, the German Society for Emergency Medicine joined, offering the Protected…
0
4
15
Recently, the EMS Educator team joined us at PAC25. Their visit sparked a powerful conversation on The EMS Educator Podcast, where we explored their firsthand experience with our course and the broader ideas shaping the future of medical education
theprotectedairway.com
Recently, the EMS Educator team joined us at PAC25, spending two immersive days diving into our world of airway education. Their visit sparked a powerful conversation on The EMS Educator Podcast, w…
0
1
3
You can learn more about how to develop a fearless FONA mindset at our website
theprotectedairway.com
Master the Fearless FONA Mindset: conquer emergency airway challenges with confidence through critical skills and immersive learning.
0
0
0