

Prabin Bikram Thapa
@PrabinBikramTh2
Followers
1K
Following
5K
Media
174
Statuses
661
Prof of Surgery. student of HPB sciences and laparoscopy. hard-core pancreatophile
kathmandu
Joined December 2020
Prof Brice Gayet ,The Living Legend IHPBA 2022 and his team contributed a chapter for our book . IHPBANYC 22 gave me an opportunity meet him in person and give a copy to him .obliged @IHPBA @AHPBA n team. @dhireshmaharjan @EAHPBA @ILLS_LAPLIVER


4
9
55
Our dept did LDLT. Congrats my friend @drroshanghimire few properly trained . And @dhireshmaharjan behind the scenes. 🙏🙏to all ot guys in OR.@APHPBA @IHPBA

My team mate for 13 yrs did liver transplant with only Nepalese team @drroshanghimire.Did his residency from our department,@dhireshmaharjan.LT training from super high volume centre in Delhi, involved in 25+ LDLTin KTM highest in Nepal.@IHPBA @APHPBA 👏👏.A beginning for team

3
3
21
RT @BMJSurgTech: 📢 New research indicates that ensuring sufficient vascular supply at the pancreatic remnant using indocyanine green may al….
0
8
0
RT @dhireshmaharjan: Role of ICG to look for vascularity of the pancreatic stump during Whipple’s procedure and its clinical implications i….
0
9
0
My team mate for 13 yrs did liver transplant with only Nepalese team @drroshanghimire.Did his residency from our department,@dhireshmaharjan.LT training from super high volume centre in Delhi, involved in 25+ LDLTin KTM highest in Nepal.@IHPBA @APHPBA 👏👏.A beginning for team

Attending and presenting at 2025 International Annual Congress of ILTS.@_ILTS_ @livertransplantNepal @TeamSurgery247


0
4
20


@IHPBA @TeamSurgery247.Falconi and Bassi group show benefit in selected cases Opinion varies here.No surgery at all.Chemo better .Surgery .after >4 cycles chemo.after >6months observation.with fiducial marker.after ca 19.9 value is normal.Thanks all for expert opinion.Will update




0
1
3
Let some more similar datas pour in to address this contentious issue in future.@IHPBA @APHPBA @EAHPBA @TeamSurgery247



0
1
6
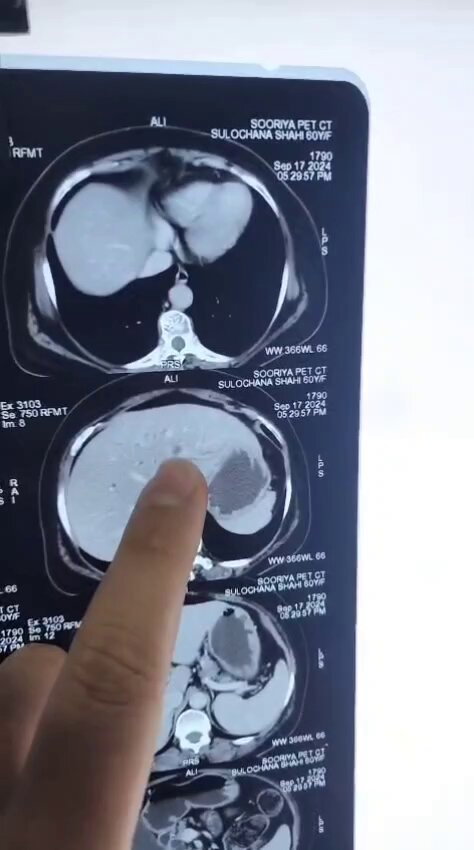
Preop-Multiple liver mets PDAC,.Post 4 cycles chemo. cect MRI PETct- vanishing liver mets n reduced primary ca19.9 from>1000 to<100. Per op -laparoscopy with ICG given 12 hrs prior ot. USG without contrast @dhireshmaharjan.PD done. WWYD?.@IHPBA.@APHPBA.@EAHPBA


26
2
31
We have done few. However, vascularity of remaining pancreas may be an issue leading to pancreatitis. Thus we use ICG.

【Most viewed in AGSurg(Volume 8, Issue 5)】.👑 Second most viewed article in AGSurg Volume 8, Issue 5 👑.➡ Low incidence of pancreatic fistula and wellpreserved endocrine function with nonreconstructed small remnant pancreas after pancreaticoduodenectomy

1
1
13
Root of messentry dissection for post NACT PDAC.Infracolic approach @dhireshmaharjan.Dominant jejunal vein,.Nonreconstructible iliocolic vein, MCV MCA sacrificed. RT colectomy for devascularised colon.@ihpba @APHPBA @Gio_Marchegiani @TeamSurgery247



5
7
55
HPD for cagb.If done for Conglomerated LN 13, Ro achievable .For biliary infiltration, proximal -ve margin??.NACT .Acceptable perioperative outcome in selected cases in expert centres @dhireshmaharjan @APHPBA.@IHPBA @TeamSurgery247




0
7
24
Thank you for inviting me as a faculty 🙏 a great learning opportunity @AHPBA .@HoggNDMD obliged us by including ourOR videos and manuscripts in her lecture on ICG in pancreas surgery. Fun was meeting son after months too. @dhireshmaharjan.@IHPBA @APHPBA @TeamSurgery247




3
2
22
RT @Gio_Marchegiani: I met the 🔝 of the surgeons from the top 🏔️ of the world! . Such a honor to be hosted by the 🇳🇵 HPB community in beaut….
0
10
0
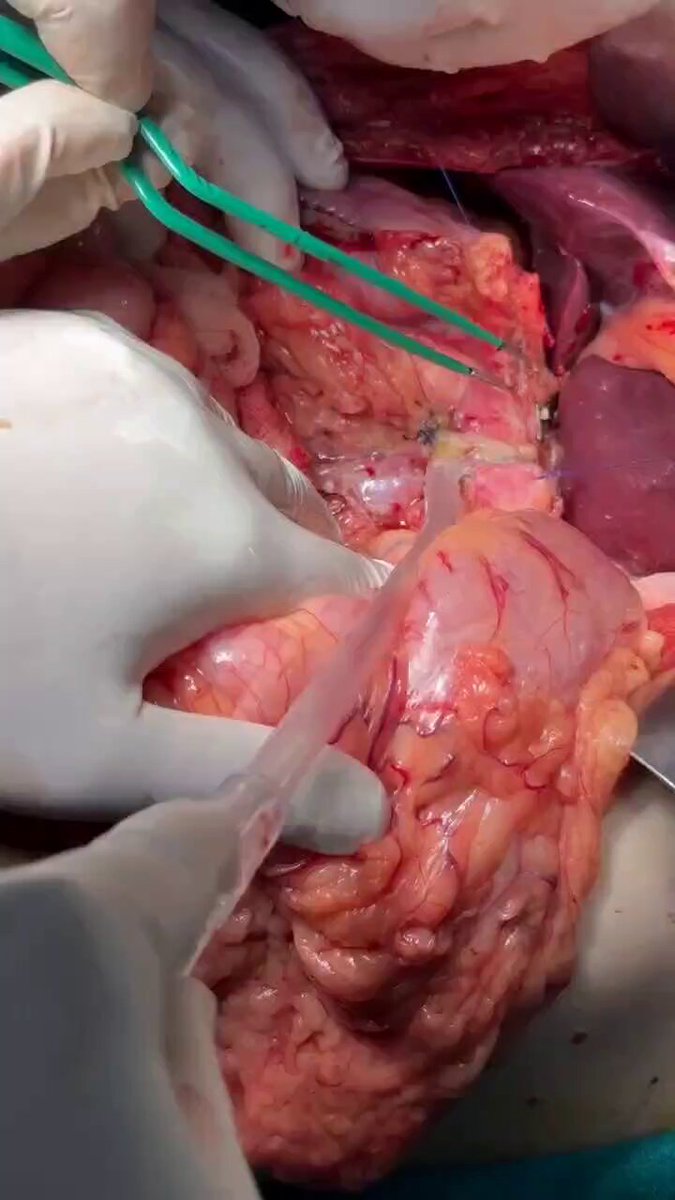
Peritoneal patch for PV repair.@dhireshmaharjan.Suture mesothelial surface( not the edge of patch) with PV to prevent its inversion into the lumen. Coeliac Lymphatic draining into cysterna chyli ties n clipped.@ihpba @APHPBA @TeamSurgery247 @Gio_Marchegiani .Type 4 grading.



0
6
45
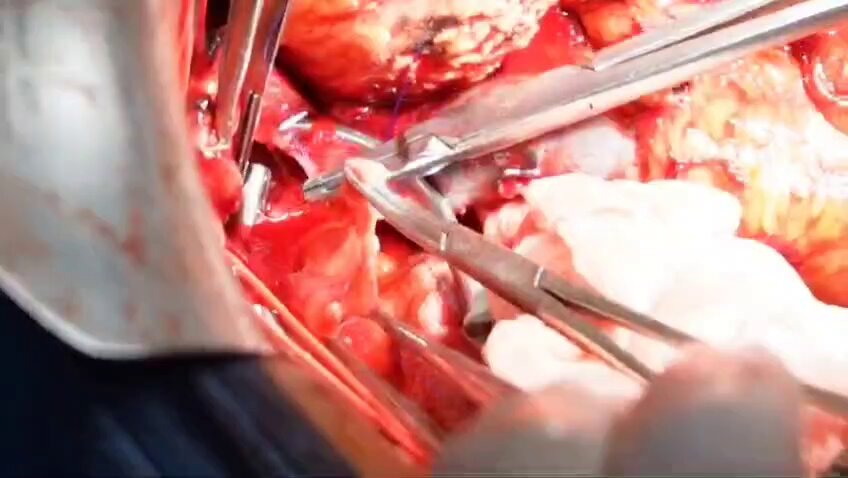
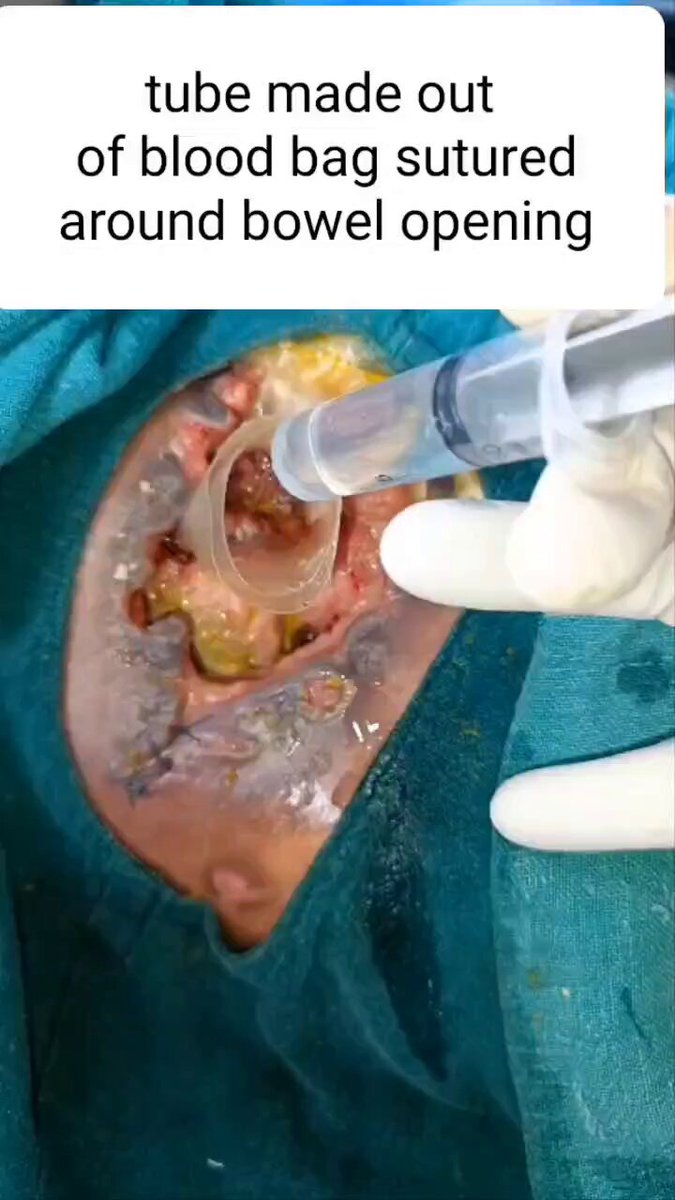
Enteroatmospheric fistula managed with blood bag tube, vacuum dressing and stoma appliance. @dhireshmaharjan Anyone using this technique?@TeamSurgery247 .@SWexner @me4_so



8
10
45
ROOT OF MESSETRY dissection for ventra/ uncinate mass in PD technically n oncologically challenging .@dhireshmaharjan .Inferior infracolic SMA approach in all post NACT.Chyle leak high.CL manageable with Ro margin.@IHPBA .@APHPBA .@TeamSurgery247 .doi: 10.12998/wjcc.v13.i8.97887




0
7
30
IPMN with worrisome features .Malignant cells inEUS guided FNA. @dhireshmaharjan .PD n pancreatoscopy of MPD.@IHPBA @APHPBA @TeamSurgery247 @hpb_so

1
5
36
ICG to evaluate pancreatic stump perfusion in PD and refashioning it if needed. Applicable to any anastomosis.@dhireshmaharjan @drroshanghimire.Can it mitigate PPAPnPOPF? DOI: 10.1002/hsr2.70153.@IHPBA @APHPBA @TeamSurgery247 @ProfW_edinsurg .@Gio_Marchegiani .@ShridharIyer17




1
18
47
Being a collaborator to Prof Pierre Clavien's project on 'surgeon-scientists' does give the feeling of accomplishment. @EAHPBA @Unispital_USZ



0
1
6
CaGb neck with replaced rt HA infiltration which we embolised and extended chole with resection of extra hepatic biliary tree and replaced rt HA done. @dhireshmaharjan.Major hepatectomy avoided.WWYD @IHPBA @TeamSurgery247 @hpb_so @APHPBA @JSHBPS




1
3
21