
Eric Hall
@Eric__Hall_
Followers
78
Following
0
Media
12
Statuses
28
We finished with an inspiring keynote by @melsulistio from @utswheart on humanity in medicine. The perfect bookend to an amazing conference. Thanks to all the organizers and speakers! @CardioNerds @CCCEnthusiasts #critcarecards24

1
4
15
Amazing panel discussion afterwards moderated by @AnnGageMD. Jacob Moller of DanGer Shock: "This was a first step. We really have to study how to manage these patients in the ICU." @CardioNerds @CCCEnthusiasts #critcarecards24.
0
3
5
Great follow up talk by Christian Hassager of DanGer Shock on importance of pt selection for tMCS. Subgroups suggest largest benefit in pts w/ low MAP, multivessel dz, younger age, earlier randomization. @CardioNerds @CCCEnthusiasts #critcarecards24

0
3
5
Very interesting talk by Kurt Huber on heterogeneity in CS & limitations of observational data in tMCS. Benefit primarily in selected AMICS patients w/o risk of hypoxic brain injury. Recent C3TN paper showed 5% of CS pts fit DanGER Shock criteria. @CardioNerds #critcarecards2024


0
2
7
Keynote address by @glennfishman on "Why I support critical care cardiology". It's ultimately about patient outcomes! Also extremely important for program growth and an "absolute necessity" in this era. @CardioNerds @CCCEnthusiasts #critcarecards24


0
2
9
Panel discussion on high risk airway including @EBohula @LMethvinMD @carlosalviar @ElliottMillerMD .- consider whether you truly have to intubate.- consider awake tube w/ numbing + low dose fent/midaz.- vasoactives hanging, +/- AV sheaths for ECMO.@CardioNerds #critcarecards24.
0
1
7
Great highlights by @LMethvinMD on CICU ventilator liberation .1. Daily screen for SBT .2. For pts on tMCS, consider whether they'll be able to sit up to protect airway.3. Optimize pre-extubation!.4.Have nipride ready, consider NIV.@CardioNerds @CCCEnthusiasts #critcarecards24

0
2
7
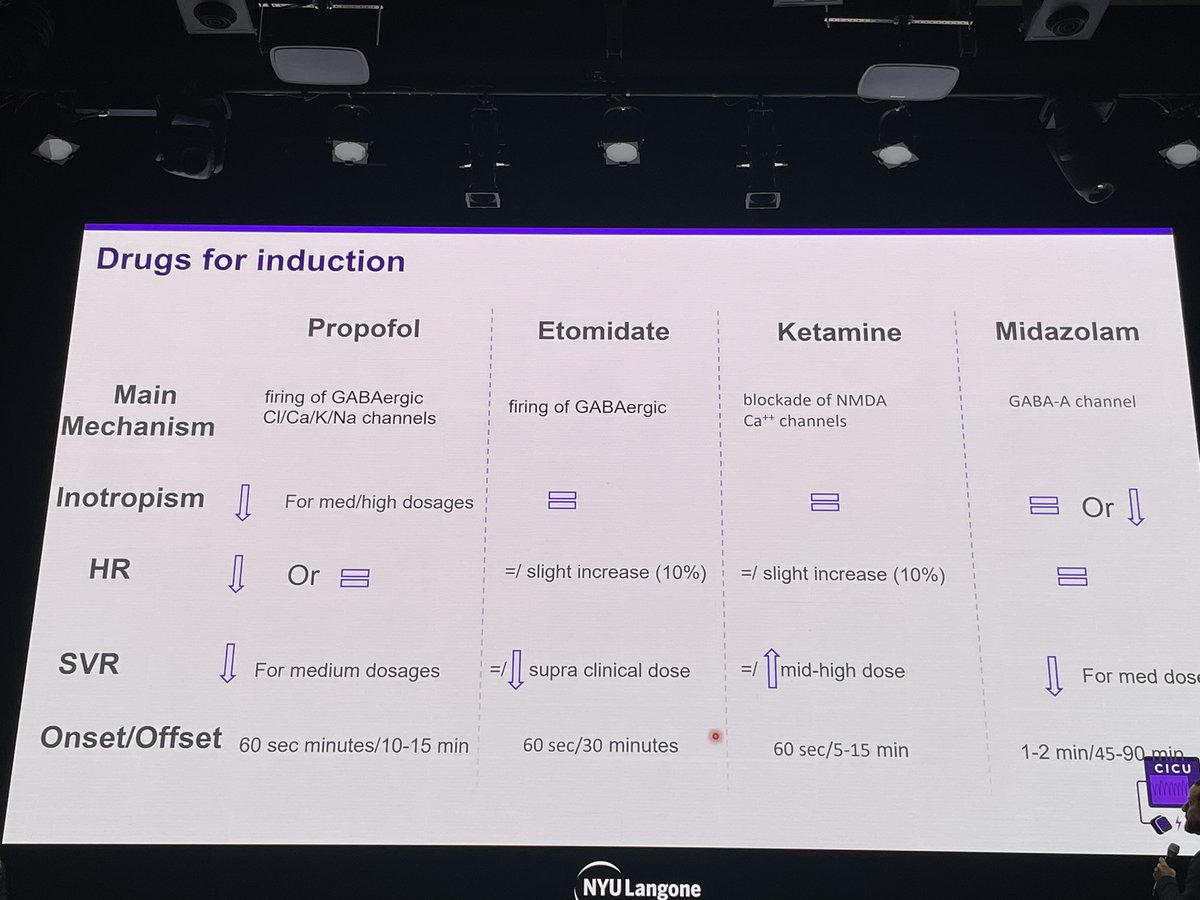
Checklist for intubation in pts with CS by Guido Tavazzi:.- make sure the IV works.- art line.- video laryngoscopy.- all induction meds can ⬇️ hemodynamics, esp at high doses. He prefers low dose fentanyl, etomidate, and rocuronium.@CardioNerds @CCCEnthusiasts #critcarecards24
0
2
9
Amazing pearls on post-cardiotomy RV failure by @AndreaElliottUM .Unique causes of post-op RVF.-inadequate cardioplegia (esp if only retrograde approach as in severe AI).- air embolism to RCA.- surgical injury to RCA or LCx.- protamine-induced PH.@CardioNerds #critcarecards24.
0
1
5
Great first talk by @Sam_Brusca on the RV.1. Most RV contraction is longitudinal; LV/septum contributes 40% .2. PAPI: good marker of RVPA coupling, cut-offs vary w chronicity.3. U-shaped relationship w PVR and lung vol, lowest at FVC.@CardioNerds @CCCEnthusiasts #critcarecards24.
0
1
8
We finished with a great session by Dr Courtney Bennett on noninvasive monitoring. Thanks to Dr Bennett, @AndreaElliottUM @JasonKatzMD @garima_d7 @YoavKarpenshif & many others for leading an amazing conference! Looking forward to the 2nd annual! @CardioNerds @UMN_CCCEdSummit

0
3
12
Very useful talk by @criticalecho followed by hands on session w/ PE devices. A few highlights:.-syncope+PE is concerning.-tPA often contradicted, 10-30% risk of major bleeding.-multiple devices exist for catheter directed lysis or mech thrombectomy.@CardioNerds @UMN_CCCEdSummit.
0
1
3
Great discussion among CICU experts including @JasonKatzMD @jason_bartos @AnnGageMD (complete with a birthday cake for @carlosalviar ). Consensus on avoiding routine LV unloading, deep sedation. @CardioNerds @UMN_CCCEdSummit @YoavKarpenshif.
2
3
10
Great case by @RickyHansra on pregnancy and ECMO. -pregnancy is a low SVR state, pts are afterload sensitive.-commonly deliver by c-section .-target SpO2>95%.-CVP, PCWP ⬆️ w/ contractions.-⬆️flows necessary to match ⬆️CO necessary.@UMN_CCCEdSummit @CardioNerds @YoavKarpenshif.
0
1
4
Really useful session on myocarditis. Have to consider the dx first. Early biopsy if unstable, high grade AVB, sustained VT + recent onset of sx. @UMN_CCCEdSummit @CardioNerds @YoavKarpenshif #CCCES2023.
0
4
7
Great session w/ @WesElyMD and colleagues on rehumanizing care/icu liberation.“Our job is to try to allow patients to get back to the life they had before the icu.”.Keys=ABCDEF bundle,esp early mobility+minimizing sedation.@CardioNerds @UMN_CCCEdSummit @JasonKatzMD @carlosalviar.
0
2
4
EEGs in the CICU:.-normal EEGs look like coarse VF.-epileptiform activity = PVCs of the brain. Abnormal synchronous firing of neuron groups.-seizures are like VT. Repetitive synchronous depolarizations. -status needs emergent tx w/in min.#CCCES2023 @CardioNerds @UMN_CCCEdSummit.
0
3
8
Great talk by @carlosalviar on heart-lung interactions in the CICU.-PPV ⬆️ RV afterload, ⬇️ preload and LV afterload.-delayed MV associated with ⬇️ survival in CS.-avoid hyperoxia.-PEEP ⬇️ MR, high PEEP ⬆️PVR.-avoid SIMV.@UMN_CCCEdSummit @CardioNerds @YoavKarpenshif @JasonKatzMD.
0
3
6
ECPR tips from @jason_bartos .-Goal 6-8min from pt arrival to ecmo flow.-15-17F arterial, 25F venous.-U/s access with fluoro confirmation.-DPC for all pts.@CardioNerds @UMN_CCCEdSummit @YoavKarpenshif @JasonKatzMD.
0
3
8
Take aways from the afternoon.-consider TEE during arrest for multiple reasons including hand placement during compression (avoid the LVOT).-subclavian access with ultrasound is very useful. And so is lung u/s.@CardioNerds @UMN_CCCEdSummit @YoavKarpenshif.
0
0
1