ML Chip Routt
@ChipRoutt
Followers
6K
Following
33K
Media
801
Statuses
5K
Positioned supine in OR with traction, the reductions were improved using lag screws where needed, and then FT screws supported the reductions achieved. Accurate reductions and safe/stable fixations with minimal necessary surgical insults are our optimal goals. Simple is good.
0
2
14
Our goal should always be to simplify the complex whenever possible. This unstable pelvic ring injury has deformity and related bladder/abdominal soft tissue injuries. She was resuscitated and distal femoral traction was applied. In the OR, we noted an incomplete left SIJ injury.
1
1
16
We recently enjoyed hosting 2 excellent visiting surgeons - from Brazil and Italy - these interactive daily experiences are incredibly valuable for so many reasons. From learning and relationship and other standpoints, “there just ain’t nothing quite like it!”. Salud!
1
2
21

A leaky defense isn’t the only problem for the Pittsburgh Steelers. Acrisure Stadium’s grass field has grown patchy in recent weeks, leading to slips and potential injuries. If an NFL team has trouble keeping grass safe and accessible, imagine a local high school that has a

turfandrec.com
Field is slated for resodding
0
2
0
The next day, she had symphysis pubis ORIF and revision of the loosened posterior screws. Her clinical course was uncomplicated thereafter. The symphysis pubis doesn’t always heal uneventfully…stay suspicious of everything!!
1
1
14
This 54yoF had a pelvic injury after MCA. Perc fixation was used with an anterior external fixation device. 8 weeks later in clinic, her pins were infected and loose. An X-ray showed no failure. The frame was removed and she had immediate pain. Another X-ray shows the failure.
3
6
34
Prior open prostatectomy/hysterectomy ops (+/- related XRT) can complicate anterior acetabular fracture surgery - dense scarring and prior wound infections are just 2 potential problems. Be patient with your dissections and precise with your usual retractors for the best result.
1
5
59

As the tools of hackers become more sophisticated, the technical defenses against cyber-attacks we are all used to are increasingly insufficient. Take it from the Head of IDI's Democracy in the Digital Age Program—an expert in cyber security policy—Dr. Tehilla Shwartz Altshuler,
47
79
268
You can use OR down time to interact with learners - bedsheet illustrations done in real time are injury focused and tailored to learners’ needs - I draw as we interact to emphasize our learning points and also to document the conversations - these also motivate more learning
1
2
51
UTH OrthoTrauma Family 2025 - the people who do the extra hard work everyday are what make it special
2
0
31
Zimmer Pelvic Fellows Course 2025 - this was our 7th annual event - 2 packed days - huge thanks to all
1
2
21
The reduction shown here is NOT GOOD!! Gaps-steps-pieces that haven’t been reduced properly on the postop imaging correlate with poor results. Realize that these articular fractures MUST and CAN actually be reduced rather than “accumulated” and covered with implants.
6
4
50
Bernie Morrey, MD - grand rounds should’ve been renamed today to “icon rounds” - amazing insights and experiences shared
6
2
30
We are sad to say goodbye to this crew of fantastic fellows, but also excited for all that’s ahead for them! Go do great things!
1
2
26
The AC frx surfaces had brisk bleeding so we quickly cleaned them and reduced the AC with manual limb traction and a spiked pusher. This quick maneuver stopped the frx related bleeding. Our preop plans and the sequence of exposure should always account for such circumstances.
1
1
9
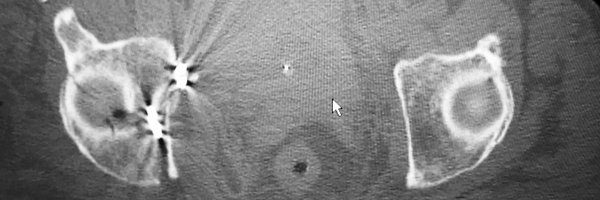
The plain pelvic and axial CT images demonstrate bladder displacement most likely due to bleeding from the left associated both column acetabular fracture. The surgeon should be well prepared to work expeditiously if/when the fracture surfaces bleed excessively at surgery.
2
1
33
Asymmetrical upper sacral dysmorphism is seen in this pediatric patient - these surface rendered images in pediatric (and adult too!) patients offer us excellent opportunities to better understand the natural history and details of this condition.
1
4
22
The upper sacral osseus fixation pathway obliquity is seen on the axial image. The second sacral segment shows much more bone area available for fixation screws. It’s crucial to understand sacral dysmorphism in order to accurately plan and perform safe posterior pelvic fixation.
1
0
5
Upper sacral dysmorphism is seen on these images. The outlet rendering shows the upper sacrum colinear with the iliac crests, residual disc, residual transverse processes (mamillary bodies), noncircular upper nerve root tunnel exits, and more acute alar slopes. The axials confirm
1
6
33
Our annual UTH Ortho research day has started - so much enthusiasm for excellent research - it gets us to the clinical solutions that we need. Plus Huge Congratulations to our resident graduates!!
0
1
15