
New
#APLS
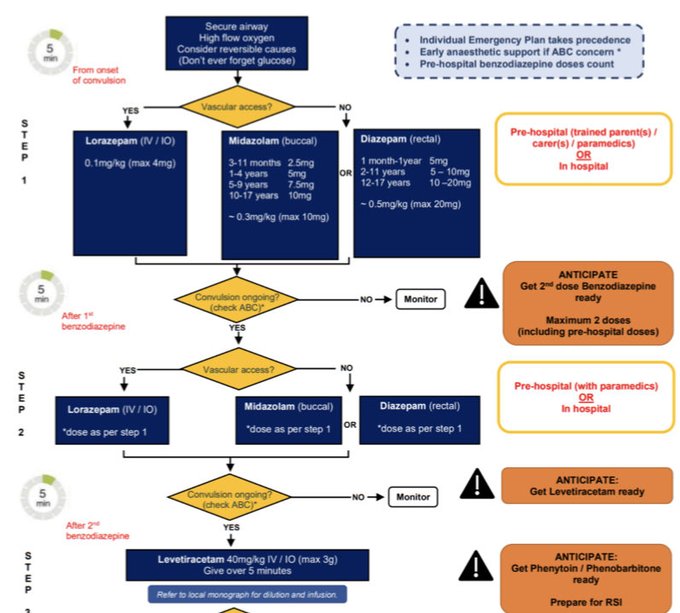
status epilepticus guideline published.
* Timings are tighter, new intervention every 5 mins
* Levetiracetam is 2nd line agent
Why? 90% self terminate within 4mins, but >5mins = 80% chance of >30min duration = ⬆️ risk of death.
Early intervention crucial
#FOAMed
8
116
268
Replies
For those following the original post, there is more to the algorithm. I initially wanted to raise awareness of the first 3 steps to
#paramedic
colleagues.
Onwards…
10mins after Levetiracetam, either
#RSI
with ketamine, or phenytoin/phenobarb infusion if not ready for RSI

0
4
13

@heli_med_james
Let’s hope JRCALC
@AACE_org
catch up swiftly and incorporate into prehospital guidance too!
2
1
7
@WilBroughton
@AACE_org
Yeah, absolutely! Particularly because it’s not a huge change to what we do already, just second dose faster. Would be great to have a comment in there about critical care teams for levetiracetam too…
#JRCALC
2
0
11

@heli_med_james
Thanks for sharing.
Why no IV diazepam when we know lorazepam is more often than not having a supply disruption, it is a fridge line and it is not in sch 17 exemptions for paramedics?
2
0
5
@rcfallon
I agree, it’s frustrating that the guideline sidelines a large group of clinicians involved in the management of these patients. Also don’t understand the focus on Lorazepam when Cochrane review found diazepam to be equally efficacious
0
0
6

@heli_med_james
Thanks for posting. Very much in favor of rapid, aggressive dosing. Curious, do you know why IM wasn't included?
1
0
0
@JoshuaStilley
No, I’m not sure. From my understanding, the evidence seems to suggest that IV/IN/IM/PR are all fairly comparable when it comes to seizure cessation. I guess suggesting delivery options which are needleless is safer in a fitting patient?
1
0
1

@JakePot82518129
For prehospital practice we tend to favour either buccal midazolam or rectal diazepam. From what I understand, all routes seem to be pretty comparable with regard to seizure cessation and benzos
1
0
0

@heli_med_james
Do you think ambulance services should be carrying Keppra on non specialist ambulances, especially in rural areas? I wonder what the incidence is for failed termination pre hospital? Sounds like a good piece of research to do…
2
0
1
@pt1408
It’s an interesting consideration. I think the issue would be buying and servicing syringe drivers (as it’s delivered via infusion) along with initial training and maintenance of competence for staff
0
0
0


@heli_med_james
When it happens that 10 minute interval feels like an awful long time to have someone still seizing in front of you.
Still better than the days when it was common to"titrate to effect" ie being afraid of Diazepam.
0
0
1