
I and others have been saying that in a post-vax era, with cases de-coupled from hospitalizations, we need to shift our focus from cases to hospitalizations as a measure of risk and for the purpose of policy-making.
6
19
175
Replies
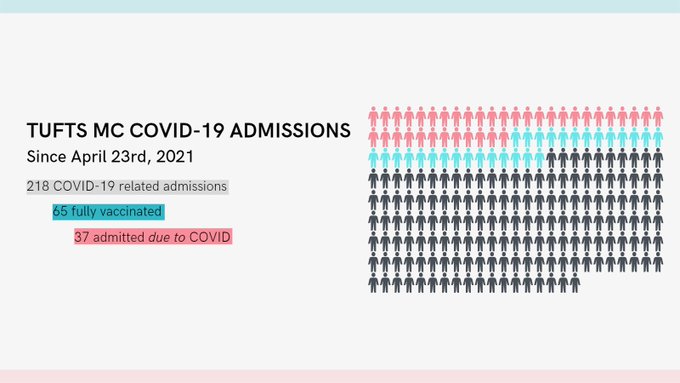
At my hospital, every COVID+ inpatient is evaluated by an Infectious Disease specialist. We are seeing more fully vaccinated patients admitted now than a few months ago. But it turns out many are in the hospital for reasons *other than* COVID. Why does that matter? 🧵
37
114
526
But if the hospitalization metric captures people admitted both *with* COVID and *for* COVID, decision-making will be based on flawed data. In August, Massachusetts DPH added a question about presence of symptoms to the daily reporting requirement. This isn’t working.
5
12
130
These are sick people admitted to the hospital with a variety of conditions (heart failure, appendicitis, etc) with symptoms that overlap with COVID, and the people entering the data are not clinicians.
3
10
92
@BranchWestyn
and I and others looked at inpatients with COVID in a large VA database. By defining moderate to severe COVID as low oxygen or use of supplemental oxygen, we were able to show decreasing severity of illness in the post-vax era.
2
10
98
@davidzweig
reported on this in
@TheAtlantic
but there was confusion among readers…to be clear, acknowledging that some patients with COVID are in the hospital for other reasons isn’t meant to minimize the suffering and death of others.

3
13
87
We need accurate data and metrics so we can understand the landscape of the pandemic and make appropriate decisions. I suggest that hospitals report COVID hospitalizations split into those who do and those who do not require supplemental oxygen. It’s not perfect, but it’s better.
13
11
149

@ShiraDoronMD
@bergerbell
It was hospitalizations in March 2020 until the shift was made to cases.
0
0
2


@ShiraDoronMD
Why only post vax era? Why didn’t it matter for children last year when it was found 45% of ped hospitalizations were coincidental to covid??
0
0
3